
Abstract
Background:
Evidence indicates that birth preparedness and complication readiness practice remain a significant problem and is not well practiced in many low-income countries, including those in East Africa. Although birth preparedness and complication readiness is practiced at low levels in most developing settings, existing literature suggests that cultural birth preparedness practices in Central Ethiopia remain underexplored, with limited empirical evidence documenting their nature and influence on maternal health outcomes. Therefore, this study aimed to assess cultural birth preparedness practices and associated factors in Central Ethiopia.
Methods:
A community-based cross-sectional study with a mixed approach was conducted from February 15 to March 16, 2023. A total of 634 mothers who gave birth within the last 6 weeks were selected by a systematic random sampling technique. Quantitative data were collected via pretested questionnaires and analyzed using bivariate and multivariable logistic regression. Variables with a p < 0.05 were considered statistically significant. For the qualitative data, five focus group discussions and 35 in-depth interviews were conducted to explore community cultural birth preparedness practices. Both inductive and deductive thematic analysis were employed in analyzing the qualitative data.
Results:
A total of 627 rural mothers from Gurage Zone were enrolled, with a response rate of 98.9%. The overall cultural birth preparedness was 84.2% (95% confidence interval: 79.8–89.3). A family size of five or more (adjusted odds ratio = 2.5; 95% confidence interval: 1.81–8.63), a birth interval of 2 or more years (adjusted odds ratio = 3.06; 95% confidence interval: 2.21–9.37), and multiparous (adjusted odds ratio = 2.32; 95% confidence interval: 1.06–10.75) were factors associated with cultural birth preparedness practices. In qualitative findings, material birth preparation, peer support group (networks), financial preparedness, engagement with traditional birth attendants, and spiritual practices were factors influencing the cultural birth preparedness practices.
Conclusion:
In this study, 84.2% of mothers practiced cultural birth preparedness. Family size, birth interval, and multiparity were associated with cultural birth preparedness practices. In addition, material, financial, peer, and spiritual supports further influenced these practices. These findings indicated that incorporating culturally acceptable birth-preparedness components into maternal health programs can strengthen community engagement, improve birth readiness, and reduce maternal complications.
Introduction
Maternal mortality and morbidity are still a great concern for developing countries. Globally, the World Health Organization (WHO) estimates that ~536,000 women die from pregnancy and childbirth-related complications each year, with 95% of these deaths occurring in sub-Saharan Africa and Asian countries. 1 In Ethiopia, one in 242 women will die of pregnancy-related causes, and one in 21 infants die before reaching the age of 1 year. 2 The Ethiopian government has enacted different strategies to avert this problem. Among those strategies is the health extension program launched in 2003 to improve rural community health status, and the urban health extension program introduced in 2009 based on the improvement obtained in the rural program. 3
By 2030, the sustainable development goals (3.1 and 3.2) target reducing the maternal mortality ratio to <70/100,000 live births globally and ending preventable deaths of newborns and children under 5 years of age.4,5 Even though some countries have made significant progress toward achieving these targets, several low- and middle-income countries, including Ethiopia, are still far from achieving them. 6 In Ethiopia, national efforts to enhance maternal and newborn health through strategies such as improving emergency obstetric care, expanding access to skilled birth attendance, and enhancing birth preparedness have led to reductions in maternal and neonatal death over the years; however, substantial gaps exist, particularly in addressing culturally related practices that influence childbirth outcomes.6–8
Culture is understood as the way of life of a people to learned behaviors, attitudes, and material expressions. 9 It is also a way of interpreting the world, developed and shared through interaction and communication. 10
Birth preparedness and complication readiness (BPCR) is a key strategy to reduce maternal morbidity and mortality and is an essential component of safe motherhood programs globally. Inadequate BPCR contributes to delays in seeking skilled birth attendants, leading to bad obstetric outcomes. 11 Promotion of BPCR has been shown to increase utilization of maternal health services and health-seeking behavior. 12 BPCR is the process of planning for normal birth and anticipating actions needed in an emergency.13,14 It promotes timely use of skilled maternal care by reducing delays. A birth plan includes identifying a skilled birth attendant, the closest appropriate facility, funds for birth and emergency expenses, transport, and compatible blood donors.15,16
The evidence revealed that every pregnant woman faces the risk of sudden and unpredictable life-threatening complications that could end in death or injury to herself or to her infant. BPCR is a relatively common strategy employed by numerous groups implementing safe motherhood programs in the world.14,17 However, it has not been well practiced in different regions of the world. Findings showed that in India, only 41% of pregnant mothers who attended a health facility had prepared for the birth. 18
Across the African countries, 38.5% in Burkina Faso 19 and 35% of mothers in Uganda 20 were prepared for birth. In Ethiopia, only a small proportion of mothers ranged from 16.5% in Arsi 21 to 37% in Gurage Zone Abeshgie district, 22 with a pooled prevalence of 32% prepared for birth. 23
There are significant differences in the components of BPCR across studies from different regions. For example, 48.9% of mothers in New Delhi, India, 18 83.3% in Burkina Faso, 19 69.6% in Goba Woreda, Oromia, Ethiopia, 24 54.1% in Wolayita zone, 25 and 65.9% in Abeshgie district 22 saved money for birth. However, gaps remain in preparing necessary materials for birth and identifying the place of delivery across these regions. Furthermore, in the Gurage Zone, 98.4% of mothers prepared food and clothing for the newborn, and 95.1% of mothers identified the place of delivery. In contrast, only 27.3% of mothers in Arba Minch Zuria identified a skilled attendant. 26
Culture and beliefs are the most determining factors for the implementation of BPCR. Women and their mothers were afraid that preparation of things for birth, especially baby clothes, would cause the death of the unborn baby. 27 The Gurage mothers save money with their neighbors who live in the community, and prepare food and clothes in a group term, which is termed as “gheze culture” for birth preparation. 22
Even though birth preparedness is practiced at a low percentage in most parts of developing countries, cultural factors have not been studied as a determining factor for birth preparedness practice. Existing literature suggests that cultural birth preparedness practices in Central Ethiopia remain underexplored, with limited empirical evidence documenting their nature and influence on maternal health outcomes. Therefore, this study aimed to assess the cultural birth preparedness practice and associated factors in Central Ethiopia.
Methods and materials
Study area and period
The study was conducted in rural areas of the Gurage Zone, Central Ethiopia, from February 15 to March 16, 2023. The Zonal administration is located in Wolkite town, which is 158 km from the capital city of Ethiopia, Addis Ababa. The zone has 16 woredas and five town administrations. According to the 2017 Ethiopian Central Statistical Agency population projection, the total population of the Gurage Zone is 1,635,311, of which 842,065 are females, and 793,246 are males. 28 The study setting was selected because maternal health service coverage in the zone remains low, with variable access to health facilities across rural woredas. 29 Further, health centers and primary hospitals are unevenly distributed, creating disparities in access to antenatal care, skilled birth attendance, and facility-based delivery. 29 A substantial proportion of women still give birth at home, often relying on traditional practices. 30 These characteristics make the Gurage zone an appropriate and relevant setting for exploring factors associated with cultural birth preparedness practices.
Study design and population
A community-based cross-sectional study with a concurrent mixed approach was conducted from February 15 to March 16, 2023. All mothers who gave birth and were living in the rural part of Gurage zone were the source population. All mothers who gave birth within the last 6 weeks and were living in the rural part of Gurage zone were the study population. All mothers who gave birth within the last 6 weeks and were living in the rural part of Gurage zone during the data collection period were included. Mothers who were seriously ill and were unable to participate in the study during the data collection period were excluded.
Sample size determination
For the quantitative data, the required sample size was calculated using the single population proportion formula 31 with the following assumptions: a proportion (p) of 50% (prevalence of cultural birth preparedness practices), a Zα/2 value of 1.96 at a 95% confidence level, and a 5% margin of error (d). After adding a 10% nonresponse rate, the sample size became: n = (Zα/2)2 p (1 − p)/d2; (1.96)2 × (0.5 × 0.5)/(0.05)2 = 422.4. Considering a design effect of 1.5, because the study employed a multistage sampling technique, and in the absence of prior intraclass correlation coefficient estimates, the final sample size was 634.
For the qualitative data, a thematic qualitative approach was implemented. A total of 35 in-depth interviews (IDIs) and five focus group discussions (FGDs) were conducted. Each focus group consisted of six mothers. The qualitative sample size was determined using the principle of data saturation.
Sampling technique and procedures
For the qualitative data, respondents were purposively selected from each kebele based on their indigenous knowledge and experience regarding cultural birth preparedness practices. In this study, elderly mothers, postnatal mothers, community women leaders, health extension workers (HEWs), and community culture practitioners were selected. Study participants were recruited through community leaders and with assistance from local HEWs. No prior relationship existed between the research team and the study participants. Participants were approached face-to-face. Data were collected through 35 IDIs and five FGDs, each consisting of six mothers, to explore individual mothers’ personal experiences and capture collective views, social norms, and community-level perspectives on cultural birth preparedness practices.
Qualitative outcomes of the study reached saturation after the 35 IDIs and five FGDs, and a few additional interviews were conducted to confirm that no new information was emerging from the respondents. The IDIs were conducted at the mothers’ homes to provide a comfortable and familiar environment, allowing mothers to speak freely, whereas the FGDs were carried out at community venues that were convenient and neutral for all participants, ensuring privacy and confidentiality. A total of 35 IDIs were conducted for depth and thematic consistency, while FGDs reached saturation after four discussions, with a fifth FGD conducted to confirm theme stability.
For quantitative data, a multistage sampling method was employed to determine the final sample size. The Gurage zone has 16 woredas. From these, five woredas were selected using a simple random sampling technique. Then, 48 Kebeles were selected out of the 150 Kebeles of the woredas by simple random sampling. A total of 1361 mothers who gave birth within the last 6 weeks were living in the selected Kebeles. The number of study participants in each of the kebeles was allocated proportionally based on the monthly report of mothers who gave birth. Finally, systematic random sampling was used to select the study participants in each kebele as K = N/n = 1361/634, where K is the skipping interval, which was approximately two from the sampling frame derived from HEW records of the kebeles (Figure 1).

Schematic representation of sampling procedures for cultural birth preparedness practices, and associated factors among mothers in Gurage zone, Central Ethiopia, 2023.
Study variables
The dependent variable of interest was the cultural birth preparedness practice. Independent variables included age, marital status, ethnicity, religion, mother’s educational status, partner’s educational status, mother’s employment status, family income, parity, family size, birth interval, history of previous abortion, history of stillbirth, and place of delivery.
Operational definitions
Cultural birth preparedness practice refers to the traditional culturally specific practices that expectant mothers and their families follow to prepare for childbirth. 32
Mothers who scored at or above the average value (⩾50%) were considered to have practiced cultural birth preparedness, while those who scored below the average value (<50%) were considered not to have practiced it. 33
Rituals refer to the cultural practices and festivals that reflect cultural values and are performed during the pregnancy period in the community. 34
Data collection tools
Data were collected using a pretested, structured interviewer-administered questionnaire that was adapted from reviewing the literature of similar studies.22,27,32,35,36 The questionnaire was initially prepared in English. The English version was translated into the local languages and translated back to English to ensure internal consistency. The questionnaire contained sociodemographic characteristics, reproductive-related factors, and questions related to cultural birth preparedness practices. The sociodemographic characteristics were assessed by eight-item questionnaires, reproductive-related factors were assessed by six-item questionnaires, and the cultural birth preparedness practice was assessed using a six-item questionnaire, addressing preparation of foods, saving money, identifying the place of birth, identifying traditional birth attendants (TBAs), identifying caregivers, and preparing clothes and materials for birth. The items required categorical responses (yes or no), with one point awarded for each correct answer and zero for each incorrect answer. The overall cultural birth preparedness practice for each participant was calculated by summing the scores from the six questions, resulting in a possible range of 0–6.
The questionnaires were evaluated for reliability and validity. Internal consistency was assessed using Cronbach’s α, which yielded a value of 0.91, while content validity was ensured through the content validity index and content validity ratio as evaluated by field experts to confirm the relevance and essentiality of the items. All data collectors and supervisors were trained for 2 days and performed practical exercises to familiarize themselves with the questionnaires. Fifteen diploma midwife data collectors who have prior experience in data collection collected the quantitative data. Five BSc midwives were used as supervisors.
Qualitative data were collected using interview questionnaires and FGDs to supplement the quantitative data. The IDI and FGD guides were structured into sections covering key thematic areas related to cultural birth preparedness practices. Each section included open-ended questions with probes to explore participants’ experiences in detail. The IDIs lasted ~60 min, and the FGDs lasted 90 min each to explore shared cultural birth preparedness practices. Seven BSc midwives with prior experience in qualitative data collection conducted the FGDs and IDIs. Each session was audio-recorded after obtaining written informed consent from the participants. The place and time of the interviews were selected to be convenient for the respondents. The principal investigator (maternal health researcher) and supervisors selected the participants, and the discussions and interviews were conducted until saturation of ideas occurred. The supervisors moderated the discussions, while the data collectors took notes and recorded all the information from the FGDs.
Data quality management
Data quality was ensured during collection, coding, entry, and analysis. Before data collection, training, and orientation were given to data collectors and supervisors. Adequate follow-up was also made with them during data collection. Moreover, the questionnaire was pretested on 5% (32 sample mothers) of the participants in Geta woreda before the actual data collection to ensure clarity, consistency, and logical sequencing of the questions, and necessary modifications were made. In addition, the supervisor and principal investigator were supervising the whole activity of the data collection process and checked the filled questionnaires every day for completeness and correctness, and necessary corrections were made on time. For qualitative data, field notes were taken during the FGDs and IDIs, and a tape recorder was used to support accurate transcription. After each session, the recordings and notes were reviewed to ensure completeness, consistency, and clarity of data. Furthermore, the trustworthiness of the study was ensured following Guba and Lincoln’s criteria. 37 Credibility was enhanced through member checking and triangulation, dependability through an audit trail, confirmability through reflexive notes, and transferability by providing detailed descriptions of the study objectives.
Statistical analysis
The data were coded, cleaned, and entered by Epi-Info version 3.5.1 and exported to Statistical Package for Social Science (SPSS) version 25 for analysis. Descriptive statistics, including texts, charts, tables, and proportions, were used to describe the data. Bivariate and multivariable logistic regression analyses were performed to see the association between outcome and explanatory variables. Variables that were found to be statistically significant in the bivariate analysis (p < 0.25, which is the cut point) were entered into the multivariable logistic regression model. A p < 0.05 was considered statistically significant in this study.
A variable having a p < 0.05 in the multivariable logistic regression analysis was considered a determinant factor for cultural birth preparedness practices. The regression model fitness was checked using Hosmer and Lemeshow goodness of fit, and was well fitted at a p value of 0.41. Multicollinearity was confirmed for interactions between independent variables through the variance inflation factor, which showed no collinearity. The odds ratio (OR) with a 95% confidence interval (CI) was used to assess the association between explanatory variables and the outcome variable. The audio-taped qualitative data were transcribed into English. Then, codes were identified and tallied to generate categories, which were later used to establish themes based on the objective of the study. In this study, both inductive and deductive thematic analysis approaches were conducted, and the findings were triangulated with the quantitative findings.
Ethical approval and consent from participants
Ethical clearance was obtained from the Institutional Review Board of Wolkite University (ref. no. IRB/252/2023) on January 12, 2023. The study was conducted based on the ethical standards of the Declaration of Helsinki. Following the approval, an official letter was taken from the research directorate, given to the Gurage Zone Health Department, then a letter of cooperation from the zonal health department to the seven respected woreda and town health offices. Then, a letter from the woreda health office was given to each selected Kebele to initiate the permission process to collect data. Participants were informed about the purpose of the study and their rights, including the right to refuse participation, the confidentiality of their information, and voluntary participation. Written informed consent was subsequently obtained. Moreover, consent from participants with no formal education was obtained after the information sheet was read aloud in the local language and documented by thumb impression with a witness. Additionally, written informed consent was obtained from the legally authorized representatives of all under 18 years before enrollment. All participant data, including transcripts and audio recordings, were stored securely in password-protected digital files accessible only to the research team. Confidentiality was strictly maintained throughout the study process, and all electronic data were kept on secure devices.
Results
Among 634, a total sample of 627 study participants were interviewed, giving a response rate of 98.9%, and the results were presented as follows under subheadings.
Sociodemographic characteristics of the study participants
One-third of the respondents, 209 (33.3%), were in the age group of 36–40 years (33 ± 2.3 SD) at a 95% CI. The majority, 89.5%, were married, and 86% were Gurage in ethnicity. A total of 208 (33.2%) were followers of the Muslim religion. Regarding mothers’ employment, 64.8% were housewives, and 392 (62.5%) had not attended formal education, followed by 70.9% of their partners who had also not attended formal education. Additionally, 302 (48.1%) of the respondents earned a monthly income of more than 3000 ETB (Table 1).
Sociodemographic characteristics of respondents in Gurage Zone, Central Ethiopia, 2023 (n = 627).
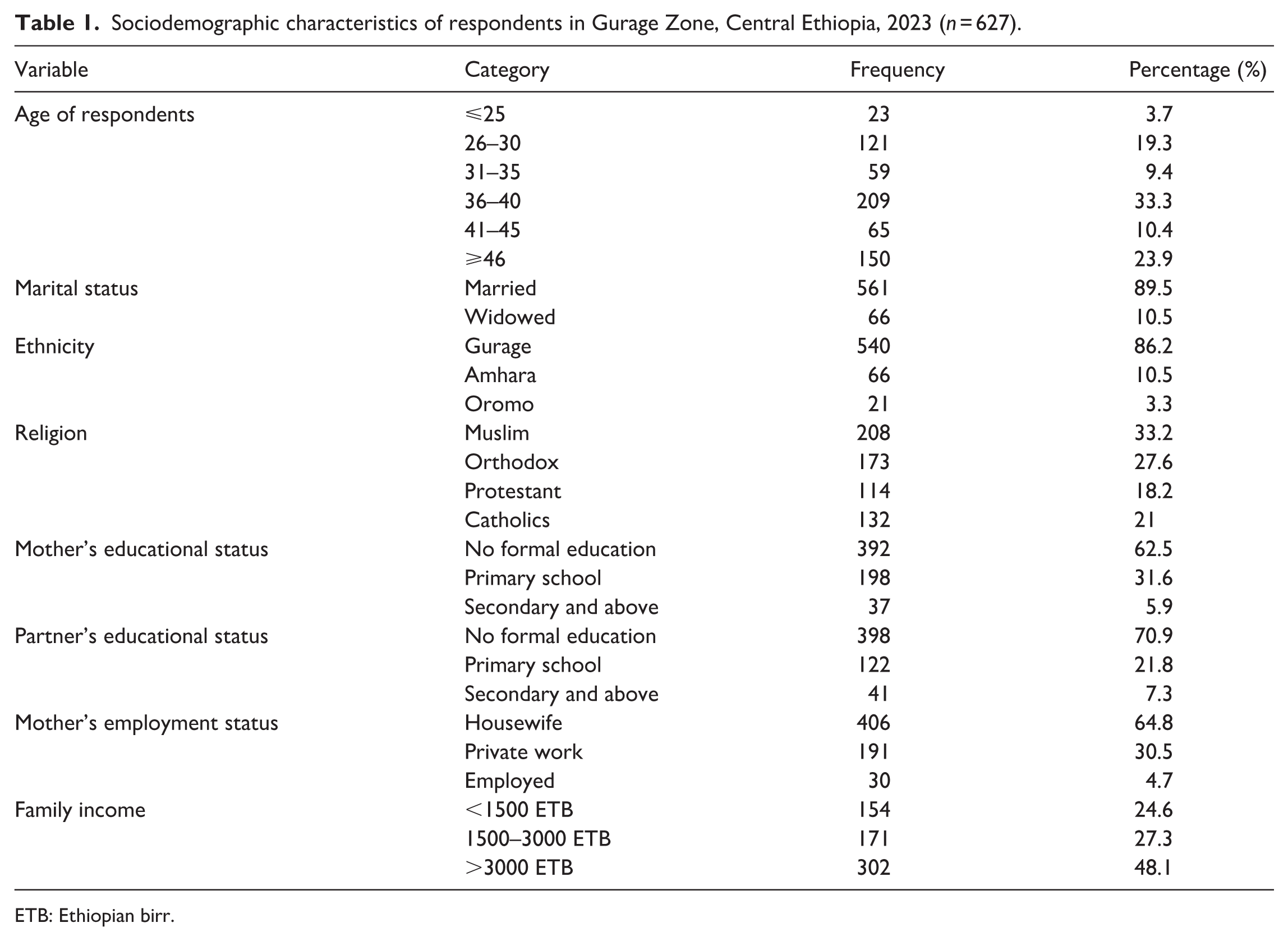
ETB: Ethiopian birr.
Reproductive-related factors of study participants
According to the results of this study, more than four-fifths (81.5%) of the participants were multiparous, and 234 (45.8%) of the respondents had a birth interval of <2 years. A total of 519 (82.8%) of the participants delivered at health facilities. Additionally, 249 (39.7%) of respondents had a family size of five or more. In this study, 89 (14.2%) of mothers reported a history of previous abortion, and 112 (17.9%) reported a history of stillbirth (Table 2).
Reproductive-related factors of study participants in Gurage Zone, Central Ethiopia, 2023 (n = 627).

The prevalence of cultural birth preparedness practice
The overall cultural birth preparedness practice was found to be 84.2% (95% CI: 79.8–89.3; Figure 2).
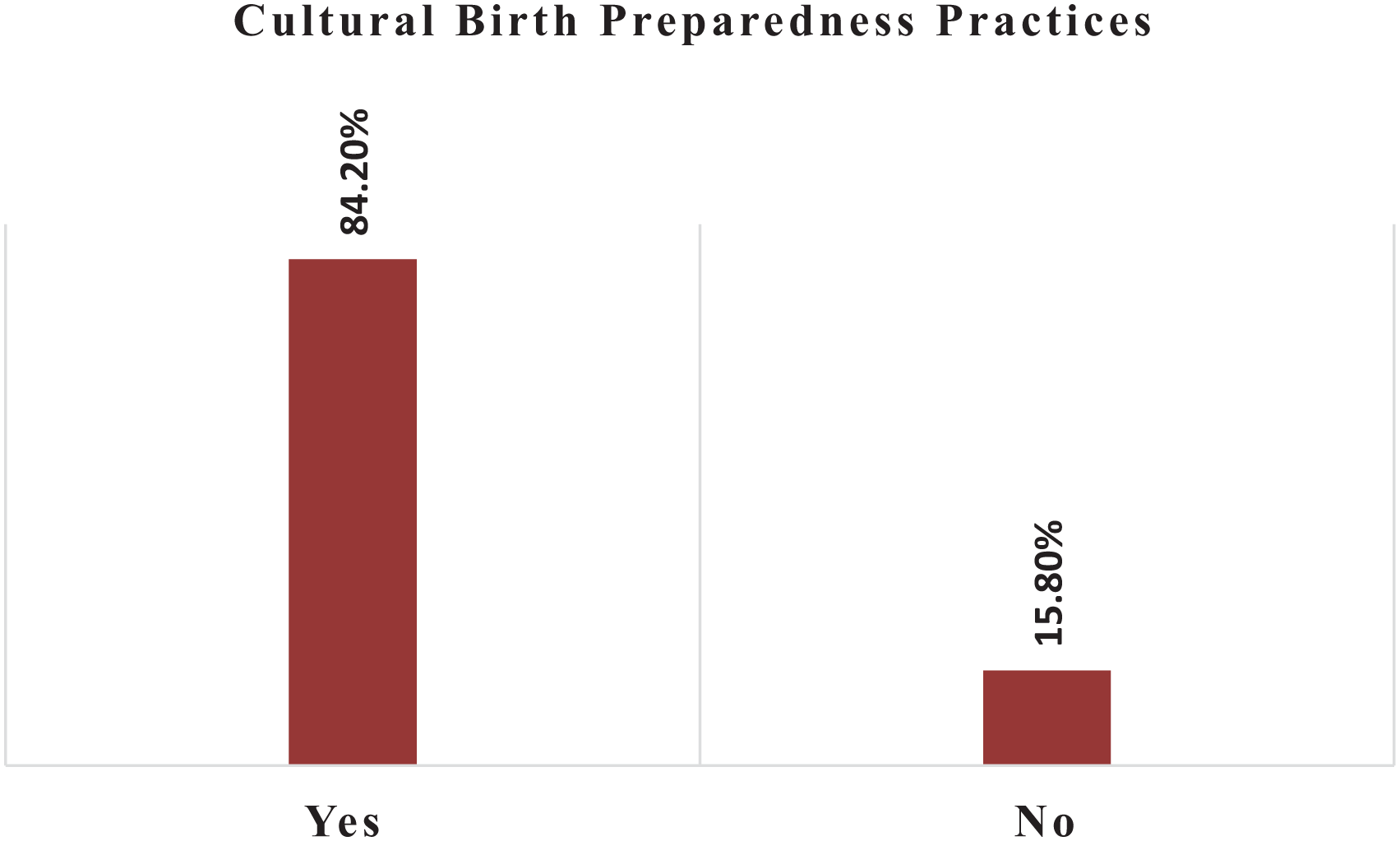
The proportion of women practicing a cultural birth preparedness among mothers in Gurage Zone, Central Ethiopia, 2023 (n = 627).
The majority of respondents (89.2%) had arranged for someone to provide support during an emergency. According to the findings of this study, 42.7% of the participants sought to identify TBAs as their birth attendants (Table 3).
Distribution of cultural birth preparedness practices among respondents in Gurage Zone, Central Ethiopia, 2023 (n = 627).

Cultural birth preparedness practices
Qualitative findings, the results of the FGD and IDI data, revealed, under the main theme, four interrelated themes describing how women and their communities practice cultural birth preparedness. Those themes are materials (items) preparations for childbirth, peer-based support groups (networks), spiritual and ritual practices, financial preparedness for childbirth, and engagement with TBAs in the communities.
Material (items) preparation for childbirth
In this study, mothers prepared materials or items for the birth of their child through existing culture based on their indigenous knowledge for birth preparedness. “A 42-year-old FGD mother stated that mothers prepare for birth by storing food with other neighbors before delivery, preparing items for receiving the newborn at the time of delivery, and arranging supportive women for assistance during and after delivery.” These reflect mother’s communal practices of childbirth preparation in the study area.
Peer-based support groups (networks)
In this study, mothers mentioned the peer-based support groups for birth preparedness, which is culturally practiced in the communities and make them unique from other regions. In addition, when a woman becomes pregnant and approaches childbirth, women from the same batch form a group and help each other prepare for birth. “A 28-year-old respondent stated, ‘When I was pregnant for the first time, my friends told me their experience and invited me to their Gheze (group turn). Then they helped me with ‘kocho (cultural food in the Gurage Zone)’ one month before delivery.” This indicated how pregnancy-related responsibilities are shared within social networks in the communities for birth preparedness.
Spiritual and ritual practices
This study identified the prayer ceremonies as birth preparedness; the rituals reinforce spiritual readiness and emotional support near childbirth. When mothers were close to delivery, a prayer ceremony was prepared for the women of the community. A 60-year-old study participant responded, “In our community, when a pregnant mother is near delivery, she will prepare foods and invite community women to attend her ceremony called ‘Yeshet sheret’.” “A prayer will be done for her to make the labor easy.” These ceremonies make the mothers spiritually and emotionally ready for childbirth.
Financial preparedness for childbirth
In this study, participants described culturally supportive financial strategies for child birth preparedness and managing childbirth emergencies. During IDI and FGD, the respondents mentioned saving money for emergency purposes. A 39-year-old mother said, “Before delivery, all family members save money and keep it with trusted neighbors, even without the rest of the family members being aware of it, for emergency purposes at the time of delivery.” These cultural practices demonstrate special norms used for risk management.
Engagement with traditional birth attendants
In the study, the mothers reported identifying TBAs before childbirth to assess the progress of labor. At the time of the IDI, respondents mentioned the identification of TBAs. “A 53-year-old mother said that before delivery, we try to identify traditional birth attendants to assess the condition of the baby and labor. Their decisions are respected in our society regarding childbirth, and we seek further treatment only if they cannot manage it.” This showed the strong cultural authority of TBAs in childbirth-related decision-making in the communities (Table 4).
Codebook for themes on cultural birth preparedness and rituals among participants in Gurage Zone, Central Ethiopia, 2023.
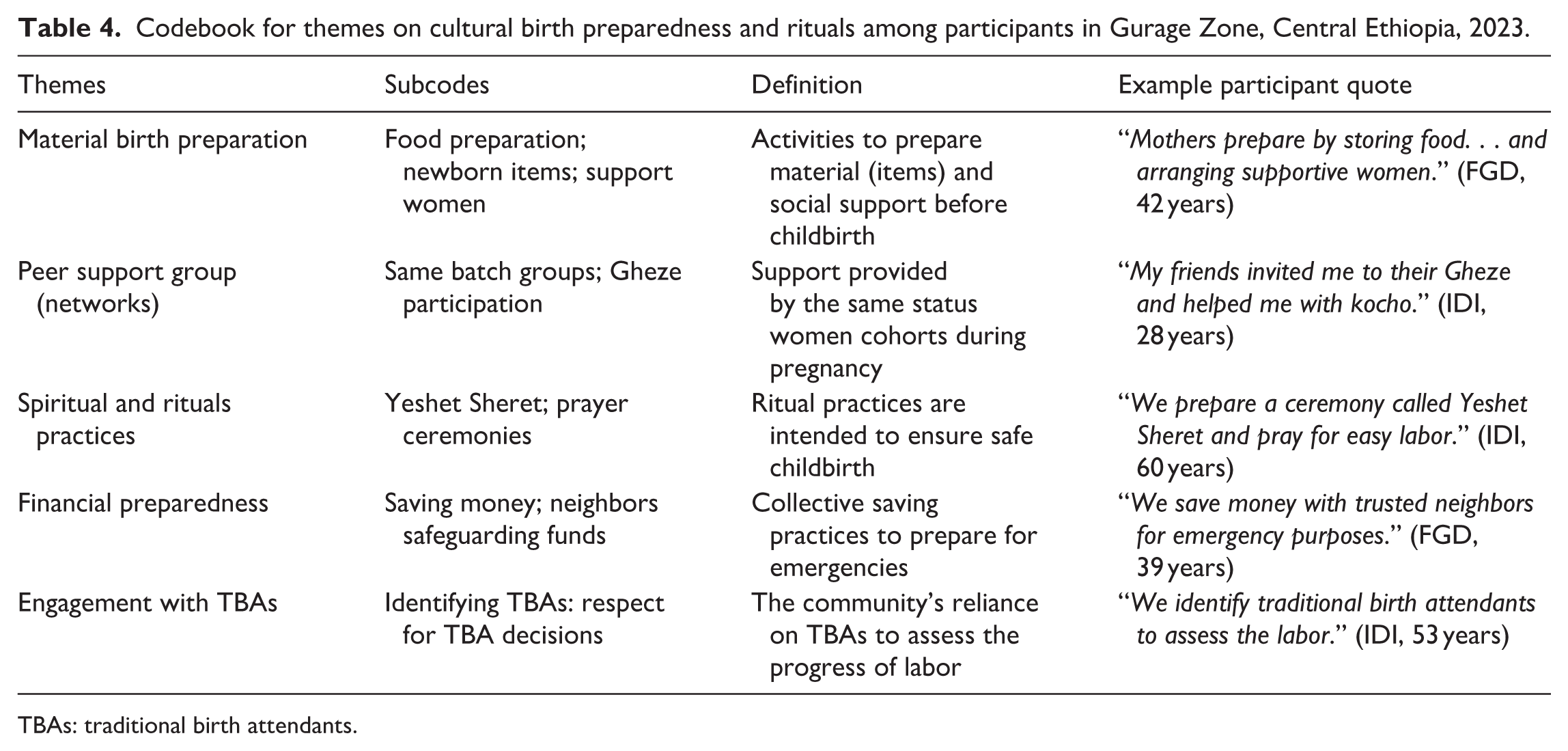
TBAs: traditional birth attendants.
Factors associated with cultural birth preparedness practices
In binary logistic regression analysis, candidate variables were selected for multivariable logistic regression at a p ⩽ 0.25. The variables like women’s educational status, women’s employment status, family income, parity, place of delivery, birth interval, and family size regarding cultural birth preparedness practices were identified as candidate variables for multivariable logistic analysis. Those candidate variables were entered into a multivariable logistic regression using the backward method to determine the final determinants of cultural birth preparedness practices by controlling for the potential confounders. In multivariable analysis, three variables, including family size, parity, and birth interval, were factors associated with cultural birth preparedness practices after confounders were adjusted in the final model.
Mothers who had five or more family size were 2.5 times (adjusted OR (AOR) = 2.5; 95% CI: 1.81–8.63) more likely to practice a cultural birth preparedness than those who had ⩽3 family size. Multiparous mothers were 2.32 times (AOR = 2.32; 95% CI: 1.06–10.75) more likely to practice cultural birth preparedness than primiparous mothers.
Mothers who gave birth with a 2 -year or more birth interval were 3.06 times (AOR = 3.06; 95% CI: 2.21–9.37) more likely to practice a cultural birth preparedness as compared to those who gave birth with <2 years’ birth interval (Table 5).
Bivariate and multivariable analysis of factors associated with cultural birth preparedness practice in Gurage Zone, Central Ethiopia, 2023 (n = 627).
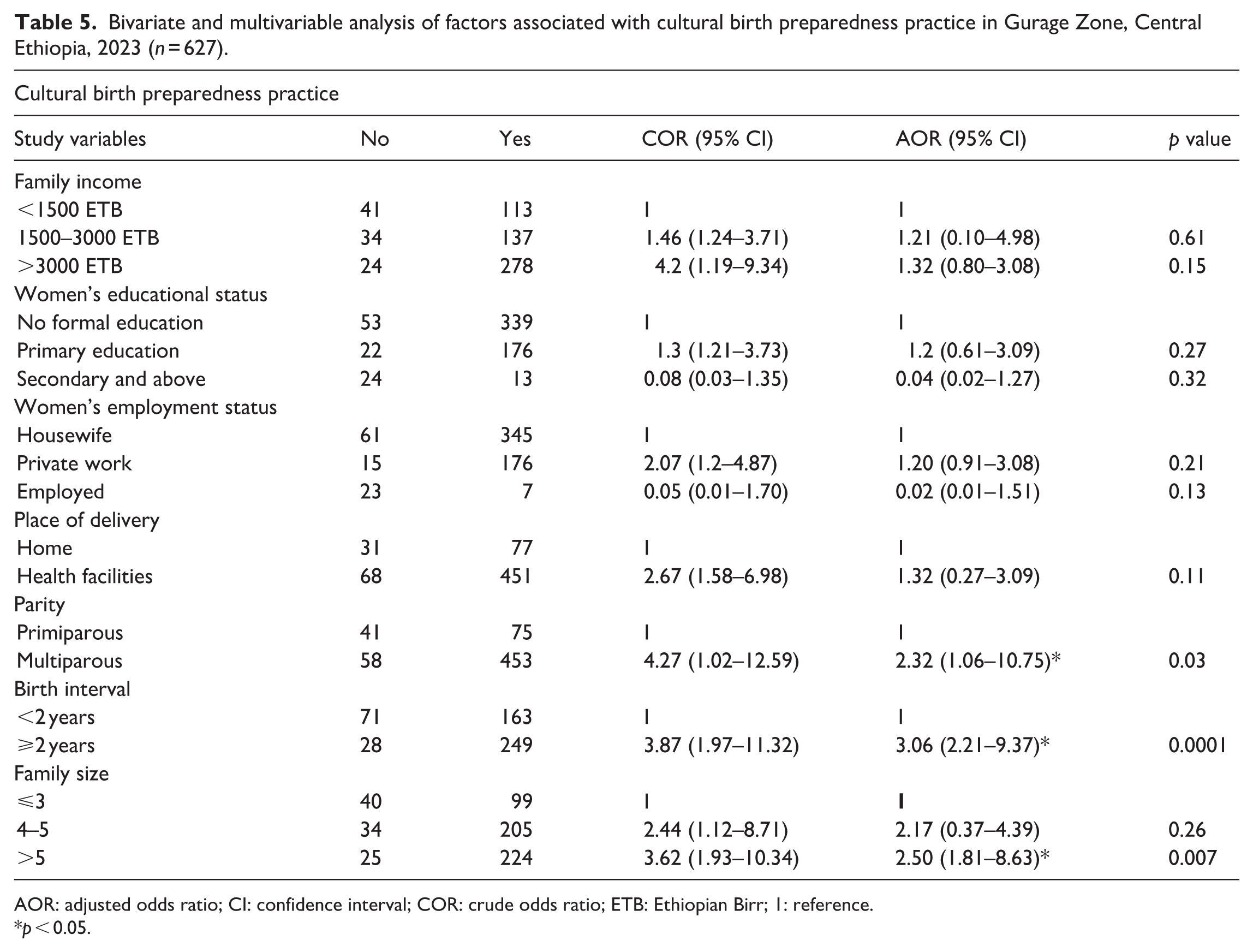
AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; ETB: Ethiopian Birr; 1: reference.
p < 0.05.
Discussion
Birth preparedness is critical for maternal health and pregnancy outcomes. Thus, unpracticed birth preparedness is the root cause of major intrapartum complications, which are associated with maternal morbidity and mortality. This community-based mixed study design identifies factors associated with cultural birth preparedness practices in the study settings. Family size, birth interval, and parity were factors associated with cultural birth preparedness practices in this study.
In this study, more than four-fifths (84.2%) of respondents practiced a cultural birth preparedness. This finding is higher than that of a study conducted in Tanzania (58.2%). 35 The difference might be due to variations in study design and area of focus. This study focused on existing cultural birth preparedness practices in the Gurage zone and aimed to elaborate on existing cultural practices to enhance modern birth preparedness practices (Supplemental Material).
In our study, more than 95% of the respondents reported storing food for birth, saving money, deciding on the place of delivery, and preparing materials for birth as components of the birth preparedness plan. The qualitative findings support these results, as study respondents reported that they save money, prepare traditional foods and items, and arrange support for birth preparation before delivery. This finding is supported by a study conducted by Kebebush Zepre and Mirgisa Kaba in the Guraghe Zone, Abeshige District. 22 This may be due to community practices and familiarity with birth preparedness plans through indigenous knowledge.
In the current study, when a woman becomes pregnant and is near childbirth, women of the same group form a support group to help each other prepare for birth. Additionally, as delivery nears, community leaders prepare a ceremony for the woman. This finding is supported by a study conducted in Malaysia on cultural beliefs and traditional childbirth practices, which reported that most women stated their husbands prepared items for childbirth, such as money, sarong, nappies, baby clothes, rope, ginger, herbal medicine, boiled water, wood, and a bamboo bed. 36
In this study, 58.2% of the respondents reported identifying TBAs within their communities, even though the WHO recommends skilled care. This finding contradicts modern birth preparedness and should be discouraged in society to reduce infections, complications, and maternal morbidity and mortality. This is further supported by the qualitative findings, where “A 53-year-old mother said that before delivery, we try to identify traditional birth attendants to assess the condition of the baby and labor. Their decisions are respected in our society regarding childbirth, and we seek further treatment only if they cannot manage it.” This study is supported by studies conducted in Northern Ethiopia, 38 Nigeria, 39 and Ghana. 40
This study identified that factors associated with birth preparedness practices, such as family size, birth interval, and parity, were found to be statistically associated with cultural birth preparedness practices. Mothers who had a family size of five or more were 2.5 times more likely to practice a cultural birth preparedness than mothers who had a family size of <3. The possible justifications may be that mothers with larger family sizes have more experience with childbirth, which could make them more aware of cultural practices related to birth preparedness. This finding was strengthened by the qualitative results, where women described collective cultural practices such as preparing food together, organizing “Gheze” group support, and involving multiple family members in cultural and spiritual practices. These cultural roles and shared responsibilities appear more feasible in larger families. Similar findings were reported in Nigeria 12 and Ghana. 41 The evidence indicated that mothers living in larger families were more likely to be prepared for childbirth, due to their lived experience, internal support networks, and shared indigenous knowledge about childbirth readiness practices. 42
Mothers who had a birth interval of 2 years or more were 3.06 times more likely to practice cultural birth preparedness. The possible reason is that longer birth intervals allow mothers more time for recovery and adequate preparation for childbirth, which may lead to adherence to cultural birth preparation practices. The qualitative findings support this evidence, as study respondents explained that longer birth intervals provide time to save money, prepare traditional foods and items, and arrange support for birth preparation and women’s groups before delivery. In addition, mothers who give birth frequently may be less prepared for birth due to work overload and crowded environments. This is supported by the Ethiopian demographic health survey. 43 The findings showed that mothers with short birth spacing may be less prepared due to health depletion, workload, or lack of recuperation time, for which the WHO recommends waiting at least 24 months between live births to reduce the risk of adverse maternal and child health outcomes.43,44
Multiparous women were 2.32 times more likely to practice a cultural preparedness plan than primiparous mothers. This might be due to multiparous mothers practicing a cultural preparedness plan due to previous childbirth experience and awareness of indigenous traditional practices compared to primiparous mothers. The qualitative findings also confirmed that experienced mothers are more aware of cultural birth preparedness, know how to engage with communities’ prayer ceremonies, and have established networks that guide them in preparing for birth using indigenous knowledge. The evidence showed that mothers with previous birth experience may practice cultural birth preparedness for delivery and its complications. 45
Therefore, these findings highlight important gaps in cultural birth preparedness practices and rituals among mothers in rural areas of Central Ethiopia. The quantitative and qualitative evidence suggest that enhancing cultural birth preparedness to support modern BPCR practices can help to reduce maternal morbidities and mortalities. Improving the quality of antenatal care, group support, prayer ceremonies, preparing for birth using indigenous practices, along with providing counseling and awareness about BPCR, could significantly improve maternal health and has the potential to reduce maternal morbidity and mortality in the study area.
Strengths and limitations of the study
This study uses a mixed-study design, which was used to explore cultural birth preparedness practices. The study also attempts to elaborate on the indigenous knowledge of mothers living in rural areas of Central Ethiopia. Although efforts were made to minimize potential limitations, this study is based on self-reported survey data, which may be influenced by recall bias and social desirability bias, as mothers might provide more socially acceptable responses. Additionally, since a cross-sectional study was used, causal relationships could not be established.
Conclusion
In this study, 84.2% of mothers practiced cultural birth preparedness. The study participants engaged in indigenous cultural ceremonial activities for birth preparation and readiness. Family size, birth interval, and parity were factors associated with cultural birth preparedness practices. In addition, material, financial, peer, and spiritual supports further influenced these practices. These findings indicate that incorporating culturally acceptable birth-preparedness components into maternal health programs can strengthen community engagement, improve birth readiness, and reduce maternal complications. Hence, the Zonal Health Office is encouraged to incorporate culturally acceptable birth-preparedness components that support modern BPCR plans. Thus, this study concludes that by intervening in modifiable factors, birth preparedness practices among mothers can be increased.
Recommendations
The following recommendations were given based on the findings to the concerned bodies: Gurage Zone Health Office is encouraged to design interventions targeting BPCR in rural settings, integrate modern BPCR and cultural BPCR counseling into routine antenatal care programs, and strengthen acceptable rituals in communities. In addition, early healthcare-seeking behaviors among near-term pregnant mothers should be encouraged in the communities rather than relying on seeking TBAs.
Health care providers need to enhance community education on maternal health care, including modern BPCR, through HEWs, and scale up maternal antenatal care (ANC) coverage at the community level. HEWs/community health workers are encouraged to create awareness on cultural birth preparedness practices that align with modern BPCR and birth spacing in order to enhance maternal health outcomes. Furthermore, a qualitative study is recommended to explore cultural birth preparation and rituals across Ethiopia, to enhance birth preparedness practices.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261440627 – Supplemental material for Cultural birth preparedness practices and associated factors among mothers in rural areas of Central Ethiopia: A concurrent mixed-methods design
Supplemental material, sj-docx-1-smo-10.1177_20503121261440627 for Cultural birth preparedness practices and associated factors among mothers in rural areas of Central Ethiopia: A concurrent mixed-methods design by Seid Jemal Mohammed, Aberash Beyene Derribow, Mebratu Demissie, Keyredin Nuriye Metebo, Aynalem Belay and Mangistu Abera in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank Wolkite University for allowing us to conduct the research and for granting ethical approval. The authors also extend their gratitude to the Gurage health office for their valuable support, study participants, data collectors, and the supervisor for their unreserved efforts and willingness to participate in this research study.
Author contributions
S.J.M., M.A., and A.B.D. participated in the conception and design of the study, data acquisition, data analysis, and interpretation, and contributed to drafting the article. M.A. and S.J.M. performed the statistical analysis. M.A. and S.J.M. also participated in the coordination of the study and assisted with editing the English language. A.B.D., A.B.D., M.D., and K.N.M. reviewed the draft article for intellectual content and participated in its revision. All authors read and approved the final article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study will be deposited in a public repository in accordance with the journal’s transparency policy and will be made openly available upon acceptance.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.