
Abstract
Background:
Breastfeeding supports infant health and development. In Saudi Arabia, although most mothers initiate breastfeeding, fewer maintain exclusive breastfeeding for the first 6 months. This study explored the relationship between maternal knowledge, attitudes, counseling, and sociodemographic factors with breastfeeding initiation and exclusive breastfeeding.
Methods:
A cross-sectional survey was conducted among 507 Saudi mothers. Self-administered Arabic questionnaire was used to assess breastfeeding practices, knowledge, attitudes, counseling experiences, and sociodemographic characteristics. Data were analyzed using descriptive statistics, chi-square tests, and logistic regression.
Results:
While n = 457 (90.1%) initiated breastfeeding; however, only n = 183 (40%) practiced exclusive breastfeeding for 6 months. Knowledge significantly predicted initiation (OR = 3.664, CI = [1.98, 6.36], P = .05) but did not predict exclusive breastfeeding. Positive attitudes significantly predicted both outcomes (initiation: OR = 1.147, CI = [1.070, 1.230], P < .01; exclusive breastfeeding: OR = 1.090, CI = [1.045, 1.138], P < .01). Prenatal counseling was associated with higher exclusive breastfeeding rates. Marital status influenced breastfeeding initiation, but no sociodemographic factors were linked to exclusive breastfeeding.
Conclusion:
Enhancing maternal knowledge may increase the initiation of breastfeeding. Meanwhile, improving attitudes and offering prenatal counseling may help increase exclusive breastfeeding rates in Saudi Arabia. Therefore, interventions that target exclusive breastfeeding may improve its rates.
Introduction
Breastfeeding (BF) is one of the most effective methods for ensuring infant health. 1 Mother’s milk provides all the nutrients needed for infant growth and neurological development. 2 It also contains immunoglobulins that protect the newborn while their immune system is still developing, and it lowers the risk of illnesses later in life.1,2
Exclusive breastfeeding (EBF) has been shown to provide greater benefits to infants compared to regular BF. According to the World Health Organization, EBF is defined as feeding the newborn only human breast milk for the first 6 months of life, meaning no other food, liquid, or even water is provided, and BF is offered on demand. 3 EBF has been linked to optimal and normal growth in infants. For example, a cohort in Sierra Leone found that infants who were EBF showed greater weight and length gains compared to non-EBF infants (difference of approx. 40 g/week and 0.9 mm/week). 4 Additionally, a systematic review of infant feeding practices found that EBF may reduce the risk of excessive or rapid weight gain which itself is a known risk factor for later obesity. 5
Several studies have reported that EBF ensures infants receive colostrum, which is the first milk produced in the days following delivery. Colostrum is rich in proteins and antibodies that help protect against asthma, infectious diseases, and childhood cancers. 6 A systematic review reported that children under 7 years of age who were exclusively breastfed had a lower risk of asthma compared to those who were not exclusively breastfed. Additionally, a meta-analysis found that EBF was associated with a 23% lower risk of childhood leukemia, as well as a reduced incidence of gastrointestinal infections and upper and lower respiratory tract infections among infants aged 4 to 12 months.7 -9
Despite the well-documented benefits of EBF, studies have reported a steady and alarming decline in breastfeeding during the first year of infancy over the past 30 years,10,11 from 62% to just 2%, which is far below the World Health Assembly’s global targets of at least 50% EBF by 2025 and 60% by 2030. 3 Moreover, only a few studies have specifically examined the persistently low rates of EBF among women in Saudi Arabia.12 -14 Results from the national survey yielded similar findings: among 4872 mothers, 91.9% initiated BF, while only 23.9% exclusively breastfed. 12 A study conducted in the central region of Saudi Arabia (n = 322) found that only 28% of mothers maintained EBF during the first 6 months postpartum. 13 Another study reported an initiation rate of BF of 95% (n = 578), yet the EBF rate was only 1.7%. 14 Similarly, studies in the western region of Saudi Arabia showed high initiation rates but low continuation of EBF. In 2 studies (n = 600 and 128), initiation rates were 95% and 91%, respectively; however, only 25% and 11% of mothers, respectively, continued EBF.15,16
A limited number of studies have explored the factors contributing to the initiation of BF and the continuation of EBF among Saudi women. Some of these factors are the knowledge levels, attitudes, and sociodemographic factors. Although knowledge about BF was generally reported as relatively high, it showed no significant relationship with EBF in most cases. 16 Alsulaimani and Hegazi et al both found adequate to high levels of knowledge about EBF among Saudi women, but this knowledge had no significant impact on EBF practices.16,17 However, another study reported a positive association between knowledge levels and practicing EBF for 6 months. 18
Various studies have evaluated attitudes among Saudi women toward BF and EBF practices.3,16,18 -21 One study reported that approximately 52.3% of 384 Saudi women demonstrated a positive attitude toward BF. 16 Another study of 178 women found that 62.2% held positive attitudes, while 37.8% reported negative attitudes; however, only 24.7% of mothers practiced EBF during the first 6 months. 19 Another study reported favorable attitudes toward specific aspects of breastfeeding: 71.6% of participants acknowledged its benefits for babies over formula, 68.8% recognized maternal benefits, and 58% held positive views about BF overall. 19 However, none of these studies conducted inferential statistical analyses to examine the relationship between attitudes and BF or EBF practices using validated tools.3,19 -21
Additionally, studies have explored the association between sociodemographic factors and the phenomenon of low EBF rates among Saudi women. Factors such as older maternal age, 14 unemployment, and lower education levels were associated with higher rates of EBF.14,18,21 -24 Pregnancy intervals of ≥1 year and multiparity (having 3 or more children) also showed a positive association with EBF. Social factors, including receiving information about BF from female relatives or receiving formal BF education, were found to increase the likelihood of practicing EBF for 6 months.16,17,22
Despite clear evidence of the benefits of BF and EBF, national and regional studies consistently show high rates of BF initiation but sharp declines in EBF continuation during the first 6 months. Although some research has explored this phenomenon, existing studies, to the best of our knowledge, are limited in addressing multiple factors associated with both BF initiation and EBF. For example, factors such as BF attitudes have not been fully examined in relation to both BF initiation and EBF within a single study. Moreover, most studies have relied primarily on descriptive analysis for either BF initiation or EBF. Thus, our study aimed to expand the body of knowledge by broadly exploring this phenomenon, including multiple factors, using reliable tools and inferential statistical analyses for both BF initiation and EBF. This approach provides a better understanding of breastfeeding practices among Saudi women. Our study had the following objectives: (a) to evaluate the relationship between BF initiation and EBF rates and knowledge levels of BF; (b) to determine the association between BF initiation and EBF rates and attitudes toward BF; (c) to determine the association between receiving BF counseling and EBF rates; and (d) to examine the associations between BF initiation and EBF rates and sociodemographic factors.
Methodology
Study Design and Sampling
A cross-sectional study design was employed, and the required sample size of 428 participants was calculated using G*Power software based on convenience sampling. 25 This sample size was deemed sufficient to detect small to medium effect sizes, corresponding to odds ratios (OR) of ≤0.5 or ≥1.9. We based the calculation on an alpha level of .05 (α = .05) and a statistical power of 0.95 (β = .05).
Recruitment and Data Collection
Ethical approval was obtained from institutional review board at the Faculty of nursing, King Abdulaziz University (Institutional Review Board. Reference number IF.27) on November 6, 2022. We recruited participants from the outpatient clinics waiting area King Abdulaziz University. After explaining the study purpose, the researcher screened women to assess eligibility. The inclusion criteria were limited to Saudi mothers aged 18 to 45 years whose youngest child was 2 years old or younger. Restricting the sample to Saudi women helped ensure homogeneity in sociodemographic characteristics and minimized potential cultural confounding factors. The age limit for the youngest child aligned with common religious and cultural breastfeeding practices in Saudi Arabia, which encourage feeding up to 2 years of age. 26
Women who met the eligibility criteria received a link to the online Arabic survey via phone. Prior to completing the survey, electronic informed consent was obtained from each participant. Data collection took place from January 2023 to April 2023.
Instruments
Outcome Variables
This study measured 2 main outcomes: the initiation of BF and EBF. For the first outcome, participants were asked to report whether they had breastfed their youngest child (Yes/No). For the second outcome, participants were asked if they had given their youngest child anything (including water or herbs) in addition to breast milk during the first 6 months (Yes/No).
Independent Variables
The survey consisted of 5 parts measuring the following variables: level of BF/ EBF knowledge, attitudes toward EBF, BF feeding practices, and whether participants had received EBF counseling.
Sociodemographic Variables
The first section of the questionnaire included items about age, education level, household income, number of children, and more. Also, this part included questions about BF, such as the time of BF initiation or the reason for not using BF.
Level of BF Knowledge
We used a tool adopted from Mahat et al 24 to assess maternal knowledge about BF. The tool consisted of 10 items, each with 2 response options: “Yes” and “No.” We awarded 1 point for each correct response and 0 points for an incorrect response, yielding a total possible score of 10. A score of ≤5 was classified as indicating a poor knowledge level, while a score of ≥6 indicated a good (high) knowledge level. In the study by Mahat et al 24 conducted in an African population, the tool demonstrated good reliability, with a Cronbach’s alpha of .85.
Attitudes Toward BF
We used an 11-item questionnaire with a Likert scale (from “strongly agree” to “strongly disagree”) to assess women’s attitudes toward BF. 27 Each item was scored from 1 (negative attitude) to 4 (positive attitude), resulting in a total possible score of 44. Scores of ≤22 indicated a negative attitude toward EBF, while scores of ≥23 indicated a positive attitude. The tool was previously utilized in an African population, where it demonstrated an acceptable level of reliability with a Cronbach’s alpha of .80.
Receiving BF Counseling
Participants were asked whether they received BF counseling (Yes/No). Two additional questions addressed the timing of receiving BF counseling (prenatal or postnatal) and the topics covered during counseling.
Translation and Validation
A professional translator translated the questionnaire from English to Arabic. It was then reviewed by 2 researchers holding PhD degrees in maternity and pediatric health to establish content validity. A total of 38 women, who were not included in the final analysis, evaluated the questionnaire for readability and clarity.
We made minor modifications in response to the feedback. In the present study, the level of BF knowledge and attitudes toward BF scales demonstrated acceptable levels of reliability, with Cronbach’s alpha values of .72 and .78, respectively.
Data Analysis
Prior to data analysis, data cleaning procedures were conducted, resulting in the removal of 18 participants due to missing data. For data analysis, we used the Statistical Package for the Social Sciences, version 27. For sample characteristics, we used descriptive statistics. Categorical variables were presented as frequencies and percentages, while continuous variables were presented as means and standard deviations. Data analysis included the following statistical approaches: we used Pearson’s chi-square test of independence to assess the relationship between the outcomes (BF practices—BF/EBF) and sociodemographic variables as well as the receipt of BF counseling; goodness-of-fit chi-square tests were used to examine BF initiation timing and its association with BF rates; binary logistic regression was applied to evaluate the relationship between participants’ levels of BF knowledge and attitudes and the outcomes (initiation of BF and EBF), with a 95% confident interval (CI), a P-value ≤.05 considered statistically significant for all tests; and finally, Cronbach’s alpha was used to evaluate the internal consistency reliability of the BF knowledge and attitude tools.
Ethical Approval and Informed Consent
The following informed consent was used during sample recruitment and data collection. Each participant was required to sign the online consent form before completing the survey. The consent began with the statement: This study is approved by the Institutional Review Board at the Faculty of Nursing, King Abdulaziz University November 6, 2022, (Reference Number: IF.27). The study was led by Dr. Sarah Alkhaifi from King Abdulaziz University, Faculty of Nursing. Participants were informed that the purpose of the study was to explore BF and EBF practices among Saudi mothers by examining their knowledge, attitudes, counseling experiences, and sociodemographic backgrounds. After that the participants were screened for eligibility criteria, included being a Saudi mother between 18 and 45 years old with a youngest child aged 2 years or younger. Eligible participants were asked to complete an online survey taking approximately 10 to 15 minutes. They were informed that participation was entirely voluntary, with the option to skip any question or withdraw at any time without consequences. Responses would remain strictly confidential, with no identifying information collected, and findings reported in aggregate form. Although no direct risks or benefits were anticipated, the study aimed to contribute to improved maternal-child health services in Saudi Arabia. By completing the survey, participants confirmed their understanding of the study, eligibility, and willingness to participate. For any questions or concerns, participants were advised to contact the principal investigator Dr. Sarah Alkhaifi’s email address and phone number.
Results
Sample Characteristics
The majority of participants were aged 30 to 39 years (41.2%), with a mean age of 32.1 years (SD = 7.3). Most were married (94.3%) and resided in the western region of Saudi Arabia (48.5%). Regarding education, 57.4% held a university degree, while 28.4% completed secondary education. The majority were housewives (73.0%), and 46.5% reported a monthly income below 5000 Saudi Riyals. In terms of delivery, 64.1% had a normal vaginal delivery, 35.9% underwent a cesarean section, and 47.7% had 1 to 2 children (Table 1).
Sample Characteristics (N = 507).

Breastfeeding Practices
The vast majority of mothers (90.1%) reported initiating BF (n = 457), while only 9.9% did not (n = 50). However, EBF rates declined considerably, with only 40% of mothers practicing EBF for 6 months (n = 183; see Table 2). Among the 50 mothers who did not initiate BF, the most commonly reported reason was the perception of insufficient milk supply (66%), which was the dominant barrier to BF initiation in this group (χ2(3) = 45.68, P < .01). Among the 457 mothers who initiated breastfeeding, 72.9% (n = 333) did so within 24 hours, while 27.1% (n = 124) initiated after 24 hours postpartum (Table 2).
Distribution of Participants According to Breastfeeding Practices, knowledge, Attitude, and Counseling (N = 507).
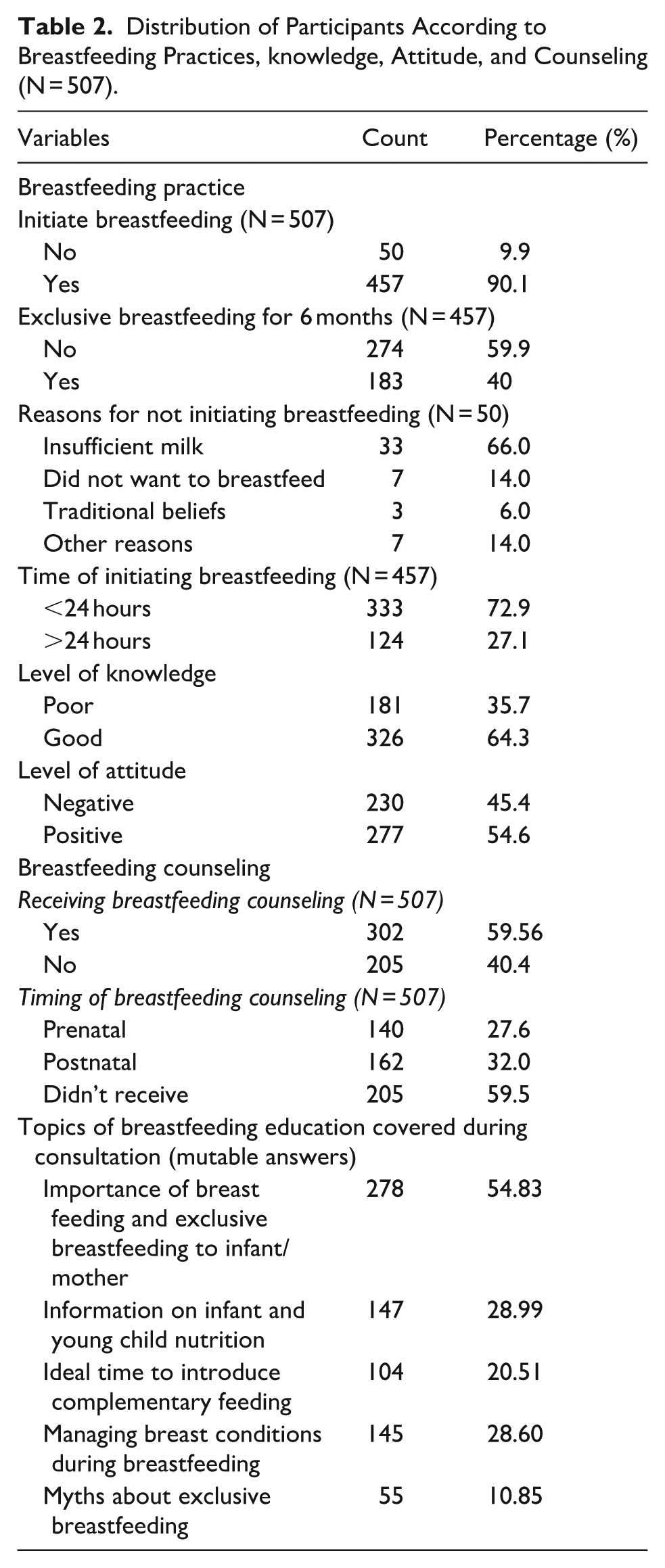
This difference was statistically significant (P < .01), indicating a higher proportion of early initiation within 24 hours in the study sample. Among the 507 mothers surveyed, 59.6% (n = 302) received BF consultation, while 40.4% (n = 205) did not (Table 2).
Level of Knowledge and Attitudes Toward Breastfeeding Practices
Regarding the level of BF knowledge, 64.3% of the participants demonstrated a good level of knowledge (n = 326), while 35.7% had a poor level of knowledge (n = 181). In terms of attitude, 54.6% of participants exhibited a positive attitude (n = 277), whereas 45.4% showed a negative attitude (n = 230; see Table 1).
Relationships Between Knowledge, Attitudes, and Breastfeeding Practices
Logistic regression analysis showed that having a good level of knowledge was significantly associated with increased odds of initiating BF (OR = 3.66, 95% CI: [1.98, 6.36], P = .05), indicating that participants with good knowledge had approximately 3.66 times greater odds of initiating BF compared to those with poor knowledge. However, knowledge level was not a significant predictor of EBF (OR = 1.06, 95% CI: [0.92, 1.21], P = .39; see Table 3).
Relationship Between Participants’ Knowledge, Attitudes, and Breastfeeding Practices.

Table 3 shows that maternal attitudes toward BF were a statistically significant predictor of both initiating BF and EBF. Positive attitude was associated with higher odds of initiating BF (OR = 1.14, 95% CI: [1.07, 1.23], P < .01), indicating that each unit increase in attitude score raised the odds of initiating BF by approximately 14.7% compared to those with a negative attitude. Similarly, positive attitude was a significant predictor of EBF (OR = 1.09, 95% CI: [1.04, 1.13], P < .01), suggesting a 9% increase in the odds of EBF for each unit increase in attitude score.
Relationships Between BF Practices and Receiving and Timing of Counseling
Receiving BF counseling was not significantly associated with BF initiation (P = .588), with initiation rates of 90.7% among counseled mothers and 89.3% among those not counseled (see Table 4). However, counseling was significantly associated with EBF (P = .05). Mothers who received counseling had an EBF rate of 40.7%, compared to 29.3% among those who did not receive counseling. Additionally, the timing of counseling was significantly associated with EBF rates (P < .01). Participants who received prenatal counseling demonstrated an EBF rate of 67.9%, compared to 25.0% for postnatal counseling and 29.7% for no counseling (see Table 4).
Pearson’s Chi-Square Results Assessing the Association Between Receiving and Timing of Counseling with Breastfeeding Initiation and Exclusive Breastfeeding.

Relationships Between Breastfeeding Practices and Sociodemographic Variables
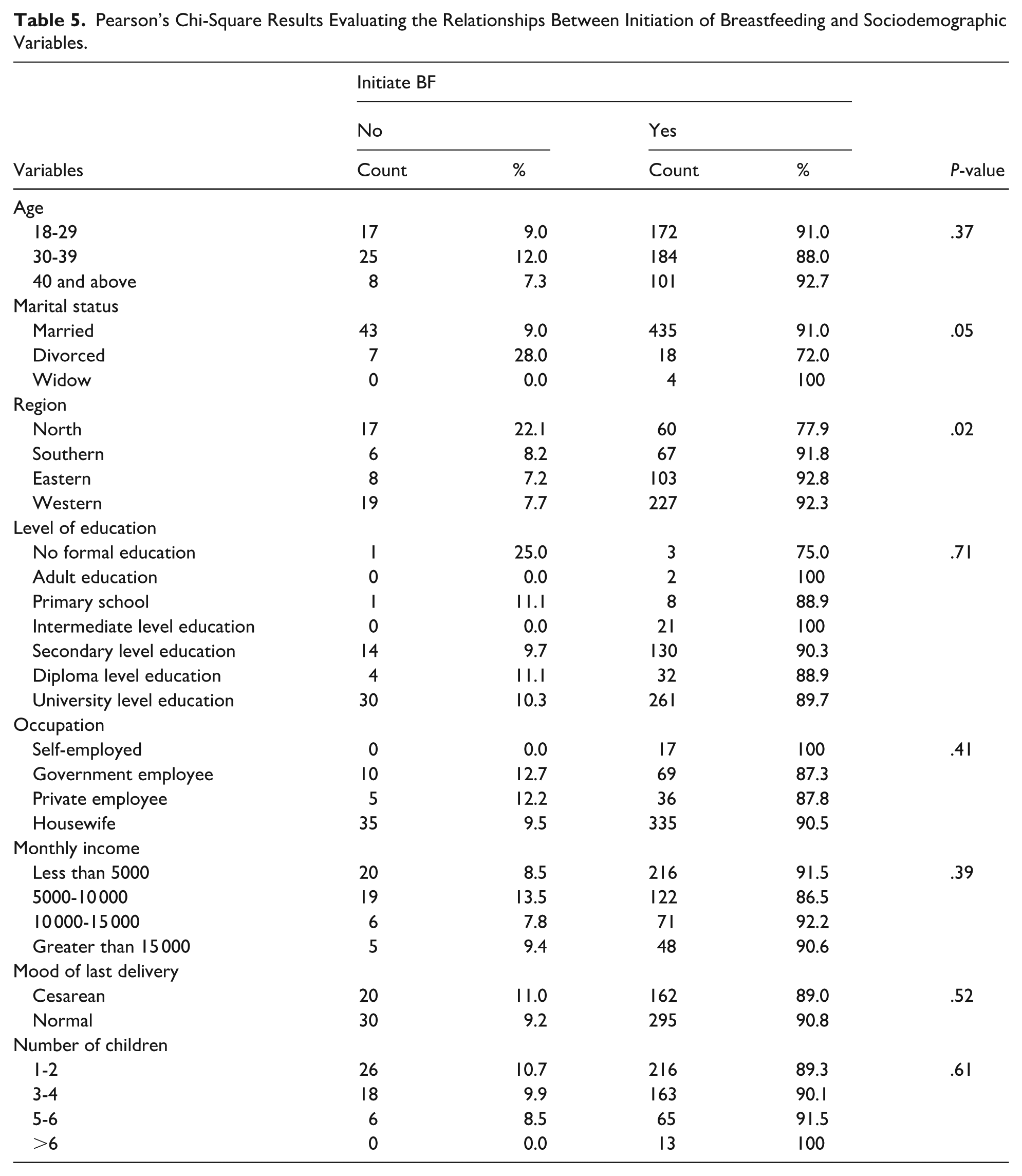
Table 5 shows that marital status and region were the only sociodemographic variables significantly associated with the initiation of BF. Being married was associated with higher rates of BF initiation (91.0%) compared to divorced women (72.0%; P = .05). Regarding region, participants residing in the eastern (92.8%) and western (92.3%) regions reported the highest rates of BF initiation, while those in the northern region reported lower initiation rates (77.9%; P = .02). In contrast, none of the sociodemographic variables were significantly associated with EBF (the results are presented in Table 6).
Pearson’s Chi-Square Results Evaluating the Relationships Between Initiation of Breastfeeding and Sociodemographic Variables.
Pearson’s Chi-Square Results Evaluating the Relationships Between Exclusive Breastfeeding and Sociodemographic Variables.

Discussion
Findings from our study emphasized similar BF and EBF practices as reported in other studies. Although initiation rates among mothers were high (90.1%), continuation of EBF for 6 months dropped to 40%. This pattern is further supported by a study conducted in nationally in Riyadh involving 252 mothers, which found that although 95% (n = 240) initiated BF, the majority introduced formula (83.4%, n = 210) and other fluids (94%, n = 237) within the first 6 months, resulting in an EBF rate of only 1.7% (n = 4) 28 Reinforcing this trend, a study from Al-Zulfi city (n = 306) reported that 93.1% (n = 286) of mothers breastfed during the first 6 months, yet only 19.3% (n = 59) adhered to EBF throughout that period. 20 Similarly, in a sample of 614 mothers from Riyadh and Dammam, the BF initiation rate was 76% (n = 467), but only 37% (n = 227) maintained EBF for 6 months. 29 Collectively, these findings reveal a consistent pattern: although BF initiation is widely practiced, sustained EBF remains suboptimal.
A similar pattern has also been reported internationally. In Lebanon, a nationally representative survey found that (89.5%, n = 1005) of infants had ever been breastfed, yet only 12.3% were exclusively breastfed at 6 months of age. 30 Similarly, in the USA, (85.7%, n = 19, 309) of children were ever breastfed, and 27.9% were exclusively breastfed at 6 months. 31 In African countries, a survey covering 25 countries (n = 17, 431) reported an average EBF prevalence of 49%, though this varied markedly by country. For example, 83% of infants in Burundi were exclusively breastfed, exceeding the World Health Organization target for 2030, whereas only 19% of mothers in Gabon reported EBF. 32
In our study, “insufficient milk” was the most frequently reported reason for not initiating breastfeeding, cited by 66.0% of mothers. This reason was given much more frequently than other reasons, such as not wanting to breastfeed (14.0%) or adherence to traditional beliefs (6.0%). Two studies conducted in the central region of Saudi Arabia reported similar findings. Among the 93.1% (258 of n = 306) who initiated BF, only 19.3% (59 of 306) practiced EBF, of whom 53.3% (31 of 59) cited the perception of insufficient milk production.12,20 Additionally, another study reported a similar finding, with insufficient milk cited by 37.3% (94 of n = 252) of mothers. 29 These findings are not limited to the Saudi context; similar trends have been reported in Iran and China, where (28%, n = 800) and (30.7%, n = 218) of mothers, respectively, cited insufficient milk as a reason for discontinuing breastfeeding.33,34
This study highlights that mothers’ attitudes play an important role in predicting actual BF practices, including both the initiation of BF and EBF. Even though most published studies have focused solely on descriptive analysis, they are consistent with our finding that 54.6% of women demonstrated a positive attitude toward BF. For example, in Taif City, two studies reported positive attitudes among 52.3% of 384 participants and 46.8% of 387 participants,19,21 while a study in Buraydah City found that 63.4% of 415 participants held positive attitudes toward BF. 35 Only one study, conducted in the northern region of Saudi Arabia (n = 124), showed a positive association between attitude and the intention to engage in BF. However, our analysis demonstrated a clear association with actual BF practice. 36
Studies using inferential analyses from other countries similarly support our findings. In Egypt, mothers with positive attitudes toward extended BF tended to breastfeed for longer durations, although the study did not specifically report on EBF. 37 In Indonesia and Ghana, positive maternal attitudes significantly increased the likelihood of EBF.38,39
In our study, most of the women (64.3%) reported a good level of BF knowledge. In the literature, knowledge levels have been described as ranging from unsatisfactory, moderate or excellent.17,18,29 Nevertheless, the associations between level of knowledge initiating of BF and EBF practices have been modestly reported in Saudi Arabia. One study found that knowledge was weakly but positively correlated with the duration of BF (r = .11, P < .03), although it did not specify whether this referred to EBF or BF. 40 Internationally, a positive association between maternal breastfeeding knowledge and breastfeeding practices, including early BF initiation and sustained EBF, has been widely documented in studies from Lebanon, India, Nigeria, and China.41 -44
Considering the results of our study and previous research, we can speculate that mothers’ attitudes toward BF may have a greater impact on EBF practices than knowledge alone. The social ecological model provides a valuable framework to understand this dynamic because it recognizes that health behaviors are shaped by multiple, interacting levels. 45 At the individual level, beliefs, educational attainment, and self-efficacy influence attitudes, such as a mother’s belief in her ability to maintain EBF for 6 months. At the interpersonal level, partner and family support play critical roles. 39 Our study found that BF initiation was more among married women. At the community level, cultural norms shape expectations, with housewives and mothers with more than 3 children reporting positive attitudes toward BF.13,17,36 At the societal level, structural barriers such as unsupportive workplaces or hospitals hinder EBF, whereas receiving BF counseling has been shown to promote EBF, as demonstrated in this study and supported by findings from other studies.13,23,35,46 These insights highlight the importance of adopting a comprehensive intervention to promote attitudes toward EBF.
Previous findings from the literature, interpreted through the social ecological model, suggest that attitudes toward BF are complex and shaped by interrelated factors across individual, interpersonal, community, and societal levels. Thus, future research should aim to measure these influences using reliable, theory-based tools and develop culturally relevant instruments grounded in Saudi women’s lived experiences, potentially through phenomenological research as an important next step.
In our study, receiving BF counseling was an important factor of EBF practices, but timing of receiving the consultation was also significant. This finding is further supported by the work Alyousefi and Al-Madani et al, who found that attending prenatal breastfeeding classes significantly increased the likelihood of EBF for 6 months.23,47 Intervention studies further support this effect: in India (n = 356), women who received antenatal counseling had higher rates of early BF initiation (91.85% vs 63.64%) and EBF (86.52% vs 67.92%) compared to the control group. 48 Similarly, in Bangladesh (n = 350), counseling during the third trimester increased early BF initiation (89.1% vs 77.4%) and EBF (73% vs 27%) compared to controls. 49
These results show the need for BF education and counseling sessions to begin during the prenatal period rather than being limited to the postpartum period. Providing education during pregnancy gives mothers time to process information, prepare psychologically, and address perceived barriers—particularly concerns about insufficient milk supply.48,49 It also helps establish a foundation for managing BF challenges and enhances maternal self-efficacy. 48 Such an approach should be considered for integration into all routine prenatal care visits, ensuring alignment with World health Organization recommendations within the local cultural contexts.
Strengths and Limitations
This study addressed an important public health concern in Saudi Arabia, where EBF rates have declined considerably over recent years. Unlike many previously published studies that rely primarily on descriptive statistics, this research employed both descriptive and inferential analyses to provide a deeper understanding of factors influencing breastfeeding practices. Furthermore, the study included a relatively larger sample size compared to most national studies in this field. However, the use of convenience sampling from a single hospital may affect the generalizability of the findings to mothers across different regions of Saudi Arabia, which is one of the limitations of this study. Additionally, the cross-sectional design prevents the establishment of causal relationships between predictors such as knowledge and attitudes and actual breastfeeding practices. The reliance on self-reported data may also introduce recall or social desirability bias. Although validated instruments were used to measure knowledge and attitudes, these tools were originally developed for other cultural settings and may not fully capture contexts relevant to Saudi women. Finally, the study did not account for potential confounding variables such as healthcare provider qualifications or the influence of spousal, family, and community support on breastfeeding behaviors.
Implications
Findings from this study suggest that improving knowledge levels may enhance the initiation of breastfeeding and increase EBF rates. Providing breastfeeding counseling during the prenatal period and integrating it into routine pregnancy visits may further support these outcomes. In addition, setting clear national target goals for both BF and EBF rates is essential for effectively measuring progress, guiding monitoring efforts, and informing policy and programmatic adjustments tailored to Saudi Arabia’s context. We also recommend longitudinal studies to evaluate the effectiveness of counseling on maternal self-efficacy and on the initiation and continuation of BF and EBF practices from the prenatal period through at least 6 months postpartum. Finally, qualitative research exploring the lived experiences of breastfeeding mothers is needed to develop effective tools for assessing attitudes and refining counseling strategies and interventions to better meet the needs of Saudi women.
Conclusions
This study identifies a clear gap between the high rates of BF initiation and the low rates of sustained EBF in Saudi Arabia. Although 64.3% of participants reported good BF knowledge, this factor only predicted BF initiation. In contrast, positive attitudes were significant predictors of both BF initiation and EBF; however, 45.4% of participants reported negative attitudes toward EBF. To improve EBF rates, our findings highlight the importance of providing BF counseling during pregnancy, which may enhance breastfeeding knowledge and promote positive attitudes toward EBF early in the prenatal period.
Footnotes
Acknowledgements
None.
Ethical Considerations
Ethical approval for this study was obtained from the Institutional Review Board on November 6, 2022 (reference number: 24-23), through the Faculty of Nursing at King Abdulaziz University, Saudi Arabia, Jeddah.
Consent to Participate
Written informed consent was obtained from all participants in accordance with these standards. The researcher clearly explained the study’s objectives, procedures, and any potential risks or benefits before distributing the survey. Participants were assured that their information would remain confidential, and all personally identifiable data were excluded from the manuscript and related documents to ensure anonymity.
Consent for Publication
Study Title: Breastfeeding and Exclusive Breastfeeding Practices Among Saudi Mothers.
Principal Investigator: Dr. Sarah Abdulkareem Abdulahmeed Alkhaifi.
Institution: Faculty of Nursing, King Abdulaziz University.
IRB Approval Date: November 6, 2022.
IRB Reference Number: IF.27.
Author Contributions
The first author, Sarah Alkhaifi, made substantial contributions to the study’s design and conceptualization, supervised data recruitment, collection, and analysis, participated in the interpretation of results, and drafted the entire manuscript. The remaining authors, including Shouq Bashawyah, Abeer AlSulami, Zahra Hashroof and Sarah Aljoudi equally contributed to the study’s conceptualization, data recruitment and collection, and assisted in drafting the manuscript. The order of authorship for this manuscript was agreed upon by all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study are currently unavailable for approximately one year, as they are being used in a subsequent research project. After this period, the data will be made available upon reasonable request for academic or research purposes, subject to evaluation and approval by all co-authors.
Invitation and Purpose of the Study
You are invited to take part in a research study that aims to examine breastfeeding and exclusive breastfeeding practices among Saudi mothers by assessing their knowledge, attitudes, counseling experiences, and sociodemographic characteristics.
Eligibility Criteria
You may participate if you:
• Are a Saudi mother
• Are between 18 and 45 years old
• Have a youngest child aged 2 years or younger
What Participation Involves
If you agree to participate, you will be asked to complete an online survey in Arabic. The survey will take approximately 10–15 minutes and can be completed at your convenience in a private or quiet setting.
Voluntary Participation
Your participation is completely voluntary. You may skip any question or withdraw from the study at any time without any penalty or loss of benefits.
Confidentiality
No personally identifiable information will be collected. All responses will remain strictly confidential and will be reported only in aggregated form to ensure your privacy.
Risks and Benefits
There are no expected risks or direct personal benefits from participating in this study. However, your participation may help support improvements in maternal and child health services in Saudi Arabia.
Consent Statement
By selecting “I agree” and completing the survey, you confirm that:
● You have read and understood the information above
• You voluntarily agree to participate in this research study
____ I agree to participate
____ I do not agree to participate
Other Journal Specific Statements as Applicable
None.