
Abstract
Background. Neonatal jaundice is more common and complicated in low and middle-income countries. However, there is no adequate evidences on the prevalence of neonatal jaundice and associated factors in Ethiopia. Methods. An institution-based cross-sectional study was conducted from 15 April to 15 June 2021 among 340 neonates admitted to neonatal intensive care unit at public specialized hospitals in Bahir Dar city. Results. The prevalence of neonatal jaundice was found to be 38.8%. Conclusion. The prevalence of neonatal jaundice was relatively high. Being male, prematurity, maternal Rh negative, neonatal Rh positive, maternal blood type AB, and ABO incompatibility were predictor variables of neonatal jaundice. Therefore, healthcare facilities in Bahir Dar city should provide opportunities for testing blood groups and Rh factors of all women early during antenatal care follow-up. Moreover, the treatment of neonatal jaundice has to be easily accessible in all primary health care units of the district.
Background
Neonatal Jaundice (NNJ) is the yellow discoloration of the skin, sclera, and mucosa caused by excess accumulation of bilirubin in the tissue and plasma. 1 NNJ is a very common clinical problem worldwide, occurring in up to 60% of term and 80% of preterm newborns in the first week of life. 2 Globally, every year, about 1.1 million babies would develop severe hyperbilirubinemia, and the majority reside in sub-Saharan Africa and South Asia. 2 According to the global burden of disease study in 2018, NNJ ranked seventh on the list of causes of mortality in the first 6 days of the neonatal period. 3 NNJ is also accountable for 70% of neonatal morbidity and 10% of mortality. 4
In Ethiopia, more than one-third of childhood death occurs within the first 28 days of age, which made among the top 10 countries with jaundice-related neonatal mortality. 5 NNJ is the most common clinical cause of hospital admissions that requires close attention, evaluation, and treatment, 6 which accounts for 75% of hospital readmissions to the neonatal intensive care unit (NICU) in the first week of life.7,8
Rhesus (Rh) incompatibility, ABO incompatibility, sepsis/infection, prematurity, birth trauma, family history of jaundice in siblings, and lack of breastfeeding are the main statistically significant factors associated with NNJ.9,10 To overcome the aforementioned problems, various interventions and prevention methods have been implemented so far including, antenatal care follow-up and screening, rapid and reliable diagnostic tools, maternal and healthcare provider education, feeding or hydration, effective phototherapy, exchange transfusion, intravenous immunoglobulin and phenobarbitone.11-13 The problem is more common and complicated in low- and middle-income countries, which has remained very high in sub-Saharan Africa.14,15
Some similar studies have been conducted in Ethiopia.1,4,10 However, this research focuses on Bahir Dar City, a region with unique cultural and social factors where traditional remedies are often practiced.8,16,17 This preference can influence the management of neonatal jaundice and lead to delays in seeking appropriate care. Moreover, The prevalence of NNJ in Ethiopia varies from 13.3% in St. Paulos Hospital Millenium Medical College to 44.9% in Tikur Anbessa specialized Hospital among admitted neonates.9,10 Localized studies are crucial for understanding regional variations in prevalence and associated factors. Furthermore, access to healthcare facilities and trained personnel is limited in the study area, which poses significant challenges for the effective management and prevention of neonatal jaundice. Knowing the burden will be an input for improving prevention, early detection, reducing the risks and overall management of pathological jaundice to reduce neonatal deaths by strengthening newborn care, which is one of priority issue in Ethiopian health policy. Therefore, this study aimed to assess the prevalence and factors associated with NNJ admitted to NICU at public specialized Hospitals in Bahir Dar city, northwest Ethiopia. Insights from this study will provide a comprehensive understanding of neonatal jaundice in a specific setting, which can lead to improved management, prevention, and overall neonatal care.
Methods and Materials
Study Design, Setting, and Population
An institution-based cross-sectional study was conducted from 15 April to 15 June 2021 at specialized hospitals in Bahir Dar city, the capital city of Amhara regional state. The city has 6 sub-cities, a total of 6 hospitals (2 public and 4 private hospitals), 10 health centers and a total population of 406,434. 18 The hospitals under study have a total of 32 NICU beds and experience approximately 865 admissions per month. All neonates admitted to NICU at specialized hospitals of Bahir Dar city during the study period were included in the study. Neonates with incomplete records of either of (blood group, Rh-factor, bilirubin level) and maternal charts with incomplete records of either of (blood group, Rh-factor screening tests) and neonates who didn’t have a mother (an attendant) and neonates of readmission during the data collection period were excluded from the study.
Population
All neonates in Bahir Dar city were the source population while those neonates admitted to NICU at specialized hospitals of Bahir Dar city were the study population.
Sample Size and Sampling Procedures
The sample size was calculated using single population proportion formula by considering that a previous study has demonstrated the prevalence of neonatal jaundice was 28.4% 19 with an assumption of a 95% confidence interval (CI), 5% margin of error, and 10% non-response rate, then the final sample size of 344 study participants were selected by using a systematic random sampling technique. Then neonates were selected at each second interval on the registration of NICU among the admitted neonates.
There are 2 public specialized hospitals in Bahir Dar city that provide NICU services. Then, proportional allocation was done to each hospital based on the neonates flow per 2 months from the previous 2 months’ data of NICU in each hospital.
Variables and Measurements
The dependent variable was neonatal jaundice while maternal and neonatal socio-demographic characteristics, neonatal factors, and obstetric factors were the independent variables.
Operational Definitions
Pathological jaundice: Is the focus of this study and is defined as the onset of neonatal jaundice within the first 24 hours of life and/or a serum bilirubin level exceeding 5 mg/dl within 24 hours. 21
ABO incompatibility: is a blood type mismatch between the mother and baby that can lead to jaundice and other issues in the newborn. 21
Data Collection Tools and Procedures
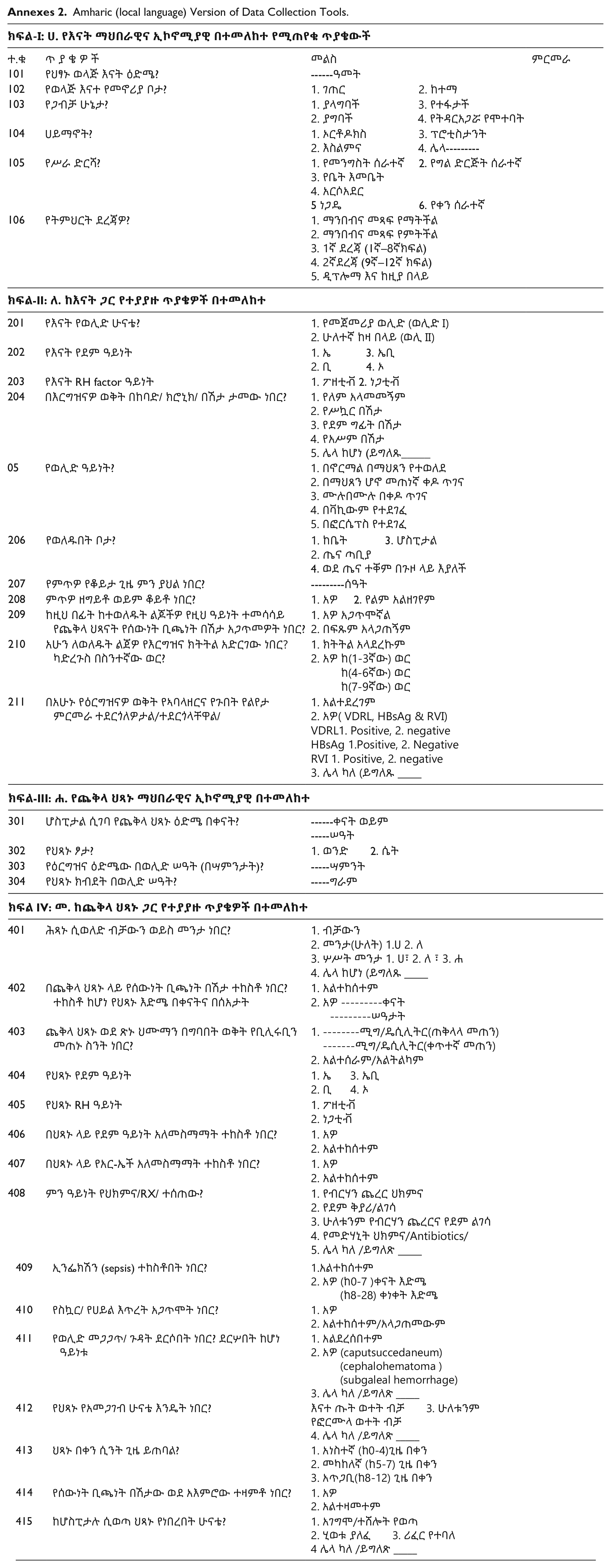
The data was collected by using pretested structured interviewer-guided questionnaires and checklists. The data collection tool was developed by reviewing different literature.9,19 The interviewer-guided questionnaires comprise 3 parts; socio-demographic characteristics of both the neonate and the mother, obstetric as well as neonatal related factors while the checklist contains a neonatal and maternal medical chart.
All neonatal data were taken from the admission book of the NICU after a full investigation was completed, and the diagnosis was confirmed. The data collection tool was first prepared in English, translated to Amharic (the local language) then retranslated to English to check for its consistency. The data was collected by 2 BSc nurses and 1 BSC nurse supervisor.
Data Quality Assurance and Control
Both data collectors and supervisors were trained by the principal investigator about the data collection techniques. Before the actual data collection, a pretest was conducted on 5% of the study population at Debark general hospital with similar characteristics to those in the study. Every day, all questionnaires were reviewed and checked at the end of the data collection and any errors were corrected accordingly by the principal investigator, supervisor, and data collectors.
Data Processing and Analysis
Data were cleaned, entered into Epi Info version 7, and exported to SPSS version 25 statistical software for analysis. A scatter plot was used to identify outliers and the model fitness was checked using the Hosmer-Lemeshow goodness of fit test which was the significance value (P = .83) and multicollinearity was checked by multicollinearity diagnosis with small inter-correlations or variance inflation factors (VIF = 1.67) was taken. Binary logistic regression analysis was computed to identify associating factors with NNJ. Variables with a P-value of less than .25 during bivariable regression were entered into multivariable logistic regression using the backward likelihood ratio. Then an Adjusted Odd Ratio (AOR) with a 95% confidence interval (CI) and P-value < .05 were considered to declare the significant factors and strength of association. Descriptive statistics such as frequency, percentages, mean, and standard deviation were presented in the form of texts and tables.
Results
Maternal and Neonatal Socio-Demographic Characteristics
A total of 340 neonates were participated in this study. The mean age of their mothers was 27.14 (SD: ±5.3) years and about 41.8% were within the range of 25 to 29 years. Almost all of the mothers 98.2% were orthodox in religion, 97.1% were married, and 57.4% were urban dwellers (Table 1).
Socio-demographic Characteristics for NNJ Among Neonates Admitted to NICU at Public Specialized Hospitals in Bahir Dar City, Northwest Ethiopia, 2021(n = 340).

Obstetric Related Factors
More than half 55.3% of the respondents were primi para and nearly half were spontaneous vaginal delivery (SVD). Nearly two-thirds were delivered at the hospital, 8.5% had prolonged labor but only 1.8% had a previous history of a sibling with jaundice, and 8.2% had a chronic illness during their current pregnancy, of which 7.4% were hypertension (Table 2).
Obstetric-related Factors for NNJ Among Neonates Admitted to the NICU of Public Specialized Hospitals of Bahir Dar City, Northwest Ethiopia, 2021(n = 340).

Neonatal Factors
Among the selected neonates, 40.9% were premature with a gestational age of 28 to 36 weeks, more than one-fourth (30.9%) were low birth weight, and 16.2% were twins. Neonatal sepsis predominantly occurred in three-fourth (76.2%) of neonates, of which, the early onset of neonatal sepsis accounts for more than three-fourth (68.2%) of neonates. In this study, more than one-fourth (25.9%) develop hypoglycemia, 10.9% had birth trauma, 32.6% had predominantly neonatal blood type “A” and the majority 91.2% were with positive Rhesus (Table 3).
Neonatal Factors for NNJ Among Neonates Admitted to the NICU at Public Specialized Hospitals of Bahir Dar City, Northwest Ethiopia, 2021(n = 340).

Abbreviations: EONS, early onset of neonatal sepsis (within 7 days); LONS, late onset of neonatal sepsis (8-28 days).
Prevalence of Neonatal Jaundice
The prevalence of NNJ among neonates admitted to the NICU of public specialized hospitals of Bahir Dar city was found to be 38.8% (95% CI = 34, 44).
Factors Associated With Neonatal Jaundice
In the multivariable logistic regression model, neonatal male sex, prematurity, maternal Rh negative, neonatal Rh positive, maternal blood group AB, mode of delivery, and ABO incompatibility were significantly associated with NNJ.
Accordingly, NNJ among males was 2 times more likely to be at risk compared to females (AOR = 2.15; 95%CI = 1.27, 3.63). Moreover, neonates with a gestational age of 28 to 36 weeks were nearly 8 times more likely to develop NNJ compared to those with a gestational age of greater than 42 weeks (AOR = 7.64; 95% CI = 2.04, 28.60). Likewise, neonates born from mothers with Rh-negative were 6 times more likely to develop NNJ compared to Rh-positive mothers (AOR = 6.29; 95% CI = 2.37, 16.71). Similarly, mothers who had blood group “AB” were 79% less likely at risk to develop NNJ than mothers with blood group “A” (AOR = 0.21; 95% CI = 0.06, 0.72).
Likewise, neonates who were delivered by instrumental delivery (forceps, vacuum) were nearly 3 times more likely to develop NNJ than neonates who were delivered by SVD (AOR = 2.91; 95% CI = 1.32, 6.42). Moreover, neonates with Rh positive were 6 times more likely to develop NNJ than neonates who were Rh negative (AOR = 6.36; 95% CI = 1.92, 21.08) and neonates who had ABO incompatibility were 15 times more likely to develop NNJ compared to those who had no ABO incompatibility (AOR = 15.33; 95% CI = 4.99, 47.09) (Table 4).
Bivariable and Multivariable Logistic Regression Analysis of Maternal, Neonatal, and Obstetric-Related Factors of NNJ Among Neonates, Admitted to the NICU at Public Specialized Hospitals in Bahir Dar City, Northwest Ethiopia, 2021(n = 340).

Abbreviations: COR, crude odds ration; AOR, adjusted odds ratio, CI, confidence interval.
Statistically significant at P-value <.05.
Discussion
In this study, the overall prevalence of neonatal jaundice (NNJ) was 38.8% (95% CI = 34, 44). The finding of this study was relatively consistence with a study conducted in Kenya 26 and Ethiopia 9 where the prevalence of NNJ was reported to be 34.4% and 44.9% respectively.
However, the prevalence of NNJ in this study was lower than a study conducted at Bloemfontein, South Africa where the NNJ prevalence was 55.2% 27 and a comparative cross-sectional study conducted in Kelantan, Malaysia 63%, 28 This variation might be due to differences in study designs in which the previous studies used retrospective chart review, geographical areas, time gap, and sociocultural parameters among study populations.
In contrast, the prevalence was higher than a study conducted in Benin 20.19%, 29 and specific studies in Ethiopia like Dessie town public hospitals (13.3%), 10 and University of Gondar Comprehensive Specialized Hospital (28.4%). 19 The discrepancy in prevalence rates could be due to several factors, including differences in study population characteristics, methodological approaches, or regional variations in disease incidence. Variations in diagnostic criteria, data collection methods, or sample sizes between studies can also contribute to differences in reported prevalence rates.
This study had shown that the odds of developing jaundice among male neonates was 2 times higher as compared to female neonates. This finding was in line with studies conducted in Ghana 30 and Nigeria.31,32 The higher odds of developing jaundice among male neonates could be attributed to biological differences, such as variations in bilirubin metabolism or liver function between genders.
In this study, prematurity was found to have a significant effect on developing neonatal jaundice. Neonates who were delivered before term (<37 weeks) were nearly 8 times more likely to develop NNJ compared to those with a gestational age of greater than term and above. This finding was in line with studies done at Tikur Anbessa Specialized Hospital in Addis Ababa and public hospitals in Dessie town.9,19 This might be related to preterm neonates having immature livers had decreased ability to conjugate the excess bilirubin level.
The result of this study indicated that the maternal Rh factor had a significant effect on NNJ. Neonates born from mothers with Rh-negative were 6 times more likely to develop NNJ as compared to neonates born from Rh-positive mothers. The increased likelihood of neonatal jaundice (NNJ) in neonates born to Rh-negative mothers is likely due to Rh incompatibility. When an Rh-negative mother carries an Rh-positive fetus, her immune system may produce antibodies against the fetal red blood cells, leading to hemolysis. This destruction of red blood cells results in elevated bilirubin levels and a higher risk of jaundice in the newborn.
This finding revealed that 12.1% of mothers were Rh-negative, out of which 6.8% of Rh-negative mothers’ neonates developed neonatal jaundice (NNJ). This finding is consistence with studies conducted in Ethiopia.1,33,34 The finding that 6.8% of Rh-negative mothers’ neonates developed neonatal jaundice (NNJ) likely reflects Rh incompatibility issues, where the Rh-negative mothers had a higher risk of producing antibodies against Rh-positive fetal blood cells, leading to jaundice in their newborns. According to this finding, neonates who were Rh-positive were 6 times more likely to develop NNJ than those neonates of Rh negatives. This may be due to the hemolytic disease of the newborn (HDN), where Rh-positive neonates are more prone to hemolysis caused by maternal antibodies in cases of Rh incompatibility. This condition leads to elevated bilirubin levels and a higher risk of jaundice.
In this study, neonates with maternal blood group AB had 79% lower odds of developing NNJ as compared to neonates from maternal blood group A. This might be due to lower incidence of blood group incompatibility. Blood group AB mothers have fewer naturally occurring antibodies against other blood groups compared to blood group A mothers, which reduces the likelihood of hemolysis and subsequent jaundice in their neonates. However, a study in Ethiopia identified maternal blood group O as a significant risk factor for neonatal jaundice (NNJ). 35 This is because maternal blood group O can have naturally occurring anti-A and anti-B antibodies that cross the placenta and cause hemolysis in neonates.
This finding also indicates that the mode of delivery significantly affects neonatal jaundice (NNJ). Neonates delivered instrumentally (using forceps or vacuum) had nearly 3 times higher odds of developing jaundice compared to those delivered by safe vaginal delivery (SVD). This finding was supported by a population-based cohort study conducted in Australia, 36 Iran, and Japan.36,37 The similarity is likely due to common risk factors associated with instrumental deliveries, such as increased trauma or bruising, which can elevate the risk of neonatal jaundice (NNJ) across different populations.
In this study, ABO incompatibility had a significant effect on developing neonatal jaundice. The odds of developing jaundice among neonates who had ABO incompatibility was 15 times higher as compared to those who had no ABO incompatibility. This finding was supported by the study conducted in Mekkha 38 The significantly higher odds of neonatal jaundice in cases of ABO incompatibility is due to hemolysis caused by maternal antibodies against fetal blood group antigens. This hemolysis leads to elevated bilirubin levels and an increased risk of jaundice in affected neonates. This results in hemolytic disease of the newborn, where maternal IgG antibodies specific to the ABO blood group system cross the placenta and cause hemolysis of fetal red blood cells. This hemolysis is a major cause of severe hyperbilirubinemia, acute bilirubin encephalopathy, and kernicterus. 39
Limitations of the Study
The limitation of this study was that it didn’t detect the contribution of G-6PD deficiency due to the inaccessibility of routine screening for the enzyme deficiency in the study area. In addition, the data registered on the neonatal and maternal medical charts might have reliability insufficiency and this might be another limitation of this study.
Conclusions
The overall prevalence of neonatal jaundice at public specialized hospitals in Bahir Dar city, was high. Being male, prematurity, maternal Rh negative, neonatal Rh positive, maternal blood group AB, mode of delivery, and ABO incompatibility were significantly associated with NNJ. It is recommended that healthcare facilities in Bahir Dar city should provide opportunities for testing the blood groups and Rh factors of all women as early as possible during ANC follow-up. Moreover, healthcare workers working in the delivery room are better to give great care to avoid birth trauma during instrumental delivery. The treatment of NNJ currently given only in referral and specialized hospitals has to be easily accessible and available in primary hospitals and health centers of the district. Service accessibility for G-6PD screening also has to be considered.
Footnotes
Annexes
Amharic (local language) Version of Data Collection Tools.
| ክፍል-I: ሀ. የእናት ማህበራዊና ኢኮኖሚያዊ በተመለከተ የሚጠየቁ ጥያቄውች | |||
|---|---|---|---|
| ተ.ቁ | ጥ ያ ቄ ዎ ች | መልስ | ምርመራ |
| 101 | የህፃኑ ወላጅ እናት ዕድሜ? | ------ዓመት | |
| 102 | የወላጅ እናተ የመኖሪያ ቦታ? | 1. ገጠር 2. ከተማ | |
| 103 | የጋብቻ ሁኔታ? | 1. ያላግባች 3. የተፋታች |
|
| 104 | ሀይማኖት? | 1. ኦርቶዶክስ 3. ፕሮቲስታንት |
|
| 105 | የሥራ ድርሻ? | 1. የመንግስት ሰራተኛ 2. የግል ድርጅት ሰራተኛ |
|
| 106 | የትምህርት ደረጃዎ? | 1. ማንበብና መጻፍ የማትችል |
|
| ክፍል-II: ለ. ከእናት ጋር የተያያዙ ጥያቄዎች በተመለከተ | |||
| 201 | የእናት የወሊድ ሁናቴ? | 1. የመጀመሪያ ወሊድ (ወሊድ I)2. ሁለተኛ ከዛ በላይ (ወሊ II) | |
| 202 | የእናት የደም ዓይነት | 1. ኤ 3. ኤቢ |
|
| 203 | የእናት RH factor ዓይነት | 1. ፖዘቲቭ 2. ነጋቲቭ | |
| 204 | በእርግዝናዎ ወቅት በከባድ/ ክሮኒክ/ በሽታ ታመው ነበር? | 1. የለም አላመመኝም |
|
| 05 | የወሊድ ዓይነት? | 1. በኖርማል በማህጸን የተወለደ |
|
| 206 | የወለዱበት ቦታ? | 1. ከቤት 3. ሆስፒታል |
|
| 207 | የምጥዎ የቆይታ ጊዜ ምን ያህል ነበር? | ---------ሰዓት | |
| 208 | ምጥዎ ዘግይቶ ወይም ቆይቶ ነበር? | 1. አዎ 2. የልም አልዘገየም | |
| 209 | ከዚህ በፊት ከተወለዱት ልጆችዎ የዚህ ዓይነት ተመሳሳይ የጨቅላ ህጻናት የሰውነት ቢጫነት በሽታ አጋጥመዎት ነበር? | 1. አዎ አጋጥሞኛል |
|
| 210 | አሁን ለወለዱት ልጀዎ የእርግዝና ክትትል አድርገው ነበር? ካድረጉስ በስንተኛው ወር? | 1. ክትትል አላደረኩም |
|
| 211 | በአሁኑ የዕርግዝናዎ ወቅት የኣባላዘርና የጉበት የልየታ ምርመራ ተደርጎለዎታል/ተደርጎላቸዋል/ | 1. አልተደረገም2. አዎ( VDRL, HBsAg & RVI)VDRL1. Positive, 2. negativeHBsAg 1.Positive, 2. NegativeRVI 1. Positive, 2. negative3. ሌላ ካለ (ይግለጹ _____ | |
| ክፍል-III: ሐ. የጨቅላ ህጻኑ ማህበራዊና ኢኮኖሚያዊ በተመለከተ | |||
| 301 | ሆስፒታል ሲገባ የጨቅላ ህጻኑ ዕድሜ በቀናት? | ------ቀናት ወይም |
|
| 302 | የህጻኑ ፆታ? | 1. ወንድ 2. ሴት | |
| 303 | የዕርግዝና ዕድሜው በወሊድ ሠዓት (በሣምንታት)? | -----ሣምንት | |
| 304 | የህጻኑ ክብደት በወሊድ ሠዓት? | -----ግራም | |
| ክፍል IV: መ. ከጨቅላ ህጻኑ ጋር የተያያዙ ጥያቄዎች በተመለከተ | |||
| 401 | ሕጻኑ ሲወለድ ብቻውን ወይስ መንታ ነበር? | 1. ብቻውን2. መንታ(ሁለት) 1.ሀ 2. ለ3. ሦሥት መንታ 1. ሀ፣ 2. ለ ፣ 3. ሐ4. ሌላ ከሆነ (ይግለጹ _____ | |
| 402 | በጨቅላ ህጻኑ ላይ የሰውነት ቢጫነት በሽታ ተከስቶ ነበር? ተከስቶ ከሆነ የህጻኑ እድሜ በቀናትና በሰአታት | 1. አልተከሰተም2. አዎ ---------ቀናት ---------ሠዓታት | |
| 403 | ጨቅላ ህጻኑ ወደ ጽኑ ህሙማን በግባበት ወቅት የቢሊሩቢን መጠኑ ስንት ነበር? | 1. --------ሚግ/ዴሲሊትር(ጠቅላላ መጠን) -------ሚግ/ዴሲሊትር(ቀጥተኛ መጠን)2. አልተሰራም/አልትልካም | |
| 404 | የህጻኑ የደም ዓይነት | 1. ኤ 3. ኤቢ2. ቢ 4. ኦ | |
| 405 | የህጻኑ RH ዓይነት | 1. ፖዘቲቭ2. ነጋቲቭ | |
| 406 | በህጻኑ ላይ የደም ዓይነት አለመስማማት ተከስቶ ነበር? | 1. አዎ2. አልተከሰተም | |
| 407 | በህጻኑ ላይ የአር-ኤች አለመስማማት ተከስቶ ነበር? | 1. አዎ2. አልተከሰተም | |
| 408 | ምን ዓይነት የህክምና/RX/ ተሰጠው? | 1. የብርሃን ጨረር ህክምና2. የደም ቅያሪ/ልገሳ3. ሁለቱንም የብርሃን ጨረርና የደም ልገሳ4. የመድሃኒት ህክምና/Antibiotics/5. ሌላ ካለ /ይግለጽ _____ | |
| 409 | ኢንፌክሽን (sepsis) ተከስቶበት ነበር? | 1.አልተከሰተም2. አዎ (ከ0-7 )ቀናት እድሜ (ከ8-28) ቀነቀት እድሜ | |
| 410 | የስኳር/ የሀይል እጥረት አጋጥሞት ነበር? | 1. አዎ2. አልተከሰተም/አላጋጠመውም | |
| 411 | የወሊድ መጋጋጥ/ ጉዳት ደርሶበት ነበር? ደርሦበት ከሆነ ዓይነቱ | 1. አልደረሰበተም2. አዎ (caputsuccedaneum) |
|
| 412 | የህጻኑ የአመጋገብ ሁናቴ እንዴት ነበር? | እናተ ጡት ወተት ብቻ 3. ሁለቱንምየፎርሙላ ወተት ብቻ4. ሌላ ካለ /ይግለጽ _____ | |
| 413 | ህጻኑ በቀን ሲንት ጊዜ ይጠባል? | 1. አነስተኛ (ከ0-4)ጊዜ በቀን2. መካከለኛ (ከ5-7) ጊዜ በቀን3. አጥጋቢ(ከ8-12) ጊዜ በቀን | |
| 414 | የሰውነት ቢጫነት በሽታው ወደ አእምሮው ተዛምቶ ነበር? | 1. አዎ2. አልተዛመተም | |
| 415 | ከሆስፒታሉ ሲወጣ ህጻኑ የነበረበት ሁናቴ? | 1. አገግሞ/ተሸሎት የወጣ2. ሂወቱ ያለፈ 3. ሪፈር የተባለ4 ሌላ ካለ /ይግለጽ _____ | |
Acknowledgements
We are grateful to the directors of public hospitals in Bahir Dar city. We would also extend our appreciation to supervisors, data collectors, and study participants.
Author Contributions
AMZ conceptualized the study. TZT and GMB contributed during data extraction and analysis. AMZ and TZT wrote the result interpretation and prepared the first draft. SMJ and GMB contributed during the conceptualization, interpretation of results, and substantial revision. AMZ, TZT, SMJ and GMB revised and finalized the final draft manuscript. All the authors read and approved the final version of the manuscript.
Availability of Data and Materials
Data will be available upon reasonable request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
All the ethical procedures were followed in accordance with the declaration of Helsinki. Ethical clearance was obtained from the ethical review committee of the school of nursing on behalf of the institutional review board of the University of Gondar (S/N/164/7/2013). Informed written consent was obtained from the legal guardian/next of kin to participate in this study after a brief explanation of the research objectives and data collection process of the study. Participants were also informed about their right to withdraw at any time or to skip a single question or many questions. Finally, the confidentiality of the information was maintained by omitting personal identifiers and using coding.
Consent for Publication
It is not applicable.