
Abstract
Objective:
Multidrug-resistant Mycobacterium tuberculosis is a public health threat in resource-limited countries where it is easily disseminated and difficult to control. The aim of this study was to determine the prevalence of tuberculosis, rifampicin-resistant/multidrug-resistant Mycobacterium tuberculosis, and associated factors among presumptive tuberculosis cases attending the tuberculosis clinic of Adare General Hospital located in Hawassa city.
Methods:
A hospital-based cross-sectional study was conducted among 321 tuberculosis suspected patients from April to July 2018. Socio-demographic, environmental, and behavioral data were collected using a structured questionnaire. Sputum specimens were analyzed using GeneXpert. Data entry was made using Epi info version 7 and analyzed by SPSS version 20. Logistic regression models were used to determine the risk factors. A p-value less than 0.05 was taken as a cut point.
Results:
In this study, the prevalence of Mycobacterium tuberculosis was 98 (30.5%) with 95% confidence interval (25.5–35.8), and the prevalence of rifampicin-resistant/multidrug-resistant Mycobacterium tuberculosis among the 98 Mycobacterium tuberculosis confirmed cases was 4 (4.1%). The prevalence of rifampicin-resistant/multidrug-resistant Mycobacterium tuberculosis among the tuberculosis suspected patients was 1.24%. Participants who had a history of treatment with anti-tuberculosis drugs were more likely to develop rifampicin-resistant/multidrug-resistant Mycobacterium tuberculosis.
Conclusions:
This study identified relatively high rifampicin-resistant/multidrug-resistant Mycobacterium tuberculosis among tuberculosis suspected patients in the study area. Early detection of drug-resistant Mycobacterium tuberculosis should be given enough attention to strengthen the management of tuberculosis cases and improve direct observation therapy short-course and eventually minimize the spread of rifampicin-resistant tuberculosis strain in the community.
Introduction
Tuberculosis (TB) is a communicable chronic disease caused by Mycobacterium tuberculosis (MTB). About one-third of the world’s population is latently infected with MTB. TB is among the top 10 causes of mortality throughout the globe from a single pathogen. In 2019, about 10 million people were infected with MTB. 1 MTB resistance to anti-TB drugs can be either primary or acquired. Primary drug resistance of MTB is a resistance that is observed among patients without prior exposure to anti-TB drugs, while acquired drug resistance is a resistance observed among previously treated TB patients.2,3 Rifampicin is one of the most powerful anti-TB drugs used for the management of TB. 4
Antibiotic resistance in MTB is not a result of a single mutation. Instead, it is due to repeated mutation in several genetic loci. Rifampicin works by binding to the RNA polymerase, β-subunit, of MTB and prevents the elongation of messenger RNA. 5 Most of the rifampicin-resistant MTB (RR-MTB) harbor mutations in the rpoB gene that codes for the β-subunit of the RNA polymerase. 6 In the majority of RR-MTB strains, mutations occur in 81 base pairs spanning codons 507–533 of the rpoB gene. 7
Rifampicin resistance has been utilized as a successful surrogate marker for multidrug-resistant MTB (MDR-MTB). Following the World Health Organization (WHO) guideline issued in 2017, all cases of RR-MTB, including those with MDR-TB, should be treated with second-line MDR-TB treatment regimens. 8
About half a million new cases of RR-MTB were reported in 2018; among this, 78% were infected with MDR-MTB. 8 Emergence and spread of drug-resistant MTB are a challenge in the African region, especially in sub-Saharan Africa where TB control is difficult due to poor health infrastructure, limited resources, and lack of awareness. 9 Data on the burden of MDR-MTB from Africa are limited due to lack of laboratory facilities, poor surveillance mechanisms, poor reporting procedures, and outdated database system. 10 About 60,000 MDR-MTB cases occur annually in the sub-Saharan region which represents about 14% of the world’s MDR-MTB burden. 11 Ethiopia stands 15th out of the 27 high-priority countries in the world and 3rd in Africa next to South Africa and Nigeria. 12 According to the second survey conducted in Ethiopia, the prevalence of RR-MTB in Ethiopia was lower than 2%. 13 In 2016, in Ethiopia, there were 219,186 new and 156,602 prevalent TB cases and 48910 TB-related deaths. 14
Drug resistance develops due to the inappropriate choice of drugs, irregular drug supplies, and factors related to patients such as poor adherence to treatment, imprisonment, and poor compliance with treatment.15–17 Drug-resistant MTB can be controlled by identifying and effectively treating sputum smear-positive cases. Furthermore, prophylaxis and health education have an essential role in controlling the spread of MDR-TB. 18 The WHO recommends DOTS (direct observation therapy short-course) and the Stop TB strategies to address the needs of the poor and vulnerable population. 19 The Federal Ministry of Health (FMoH) introduced the DOTS to Ethiopia in 2000, and it is the most cost-effective strategy for TB control in Ethiopia. 20
Unless individuals infected with drug-resistant MTB are treated appropriately, they will continue disseminating MTB in the community and accelerate the epidemics. The impact of MDR-MTB is serious especially in low-income countries like Ethiopia, where health resources, finances, and the number of skilled personnel are limited. 21 Although better techniques such as fluorescent microscopy and GeneXpert (Cepheid) are on expansion for TB diagnosis in Ethiopia, acid fast Bacilli (AFB) is still the mainstay in most parts of the country.
Southern Nations, Nationalities, and People’s Region (SNNPR) has a population of about 18 million, and more than 90% of the population lives in rural communities. Whereas diagnosis and treatment of TB are carried out in hospitals and health centers, directly observed therapy (DOT) is decentralized to health centers in SNNPR. Furthermore, at the community level, DOT is provided at the health posts. A study by Datiko et al. 22 reported 960 presumptive TB cases from a total of 38,304 studied subjects in three zones of SNNPR (Hadiya, Gurage, and Sidama). The point prevalence (smear-positive) of TB cases from Hadiya, Gurage, and Sidama zones (now Sidama region) was 148, 139, and 80 per 100,000 population, respectively. 22
According to the FMoH guidelines of Ethiopia, if MTB from TB suspected patients becomes resistant to rifampicin by GeneXpert, they will be considered as drug-resistant (DR-TB) and referred to the MDR-TB treatment initiative center (TIC). Then, the patient will be admitted to the TIC and the sputum specimens will be collected and referred to the regional laboratory for confirmation and monitoring using culture method, line probe assay (LPS), microscopy, and drug sensitivity tests. A standard second-line treatment will be given to all MDR/RR-confirmed cases daily under direct observation by a health care worker at a health care center and family DOT supporter(s) at home. The regimens include at least four second-line anti-TB drugs that are certain or expected to be effective, and the duration is a minimum of 18 months after culture conversion. 23
MDR-MTB is of high public health important problem in developing countries. In this regard, there is a scarcity of published data in the Hawassa area. The aim of this study was to determine the prevalence of TB, RR/MDR-MTB, and associated factors among presumptive TB cases attending the TB clinic of Adare General Hospital (AGH) located in Hawassa, Southern, Ethiopia.
Methods
Study design and period
A hospital-based cross-sectional study was conducted from April to July 2018.
Study area
This study was conducted at AGH which is found in Hawassa city. Hawassa is the capital of the SNNPR, Ethiopia. It is situated on the shores of Lake Hawassa in the Great Rift Valley and is located 275 km to the South of Addis Ababa, Ethiopia. According to the 2011 report from the housing and population census, the projected population of Hawassa city Administration was 374,034, out of which 190,757 were male and 183,277 were female.24,25 AGH was established in 1962 in the name of Hawassa clinic. In 2011, it was upgraded to Adare Primary Hospital and now it is known as AGH. Currently, AGH serves about 1,368,341 people. About 200 patients visit TB clinic of AGH per month.
Study population
Source population includes all patients with lower respiratory tract infections who visited AGH TB clinic during the study period. The study population was all TB suspected patients who visited AGH and fulfill the eligibility criteria.
Eligibility criteria
Patients who were suspected of TB, aged greater than or equal to 18 years, able to give sputum specimens, and willing to participate were included in this study. TB suspected patients who were unable to give sputum samples and complete information were excluded from the study.
Study variables
Dependent variables: Prevalence of MTB and RR-MTB.
Independent variables: Factors that could be associated with the prevalence of RR-MTB, such as residence, history of cigarette smoking, history of treatment with the anti-TB drug, average monthly income, and history of imprisonment, were considered under the independent variables.
Operational definition
Presumptive TB denotes a patient with signs and symptoms of TB such as night sweat, loss of appetite, loss of weight, fever, and cough which lasts for 2–3 weeks. 26
Urban is the region surrounding a city; it can refer to cities, towns, and suburbs.
Rural is any population, housing, or territory not in an urban area.
Sample size determination and sampling technique
The sample size was determined using a single population proportion formula by taking the prevalence of rifampicin-resistant TB (RR-TB) among presumptive TB patients reported from Northern parts of Ethiopia (2.3%), 17 5% margin of error, 95% confidence level (CI), and 10% non-response rate. Accordingly, the sample size was 39. However, this sample size was too small and we considered two factors such as treatment history with anti-TB drugs and failure to follow-up to obtain the maximum sample size using a power of 80% and CI of 95% (Table 1). Using the power analysis, we took the largest sample size, which is 326. A convenience sampling technique was used to recruit the 326 study participants

Sample size determination using power analysis, 2018.
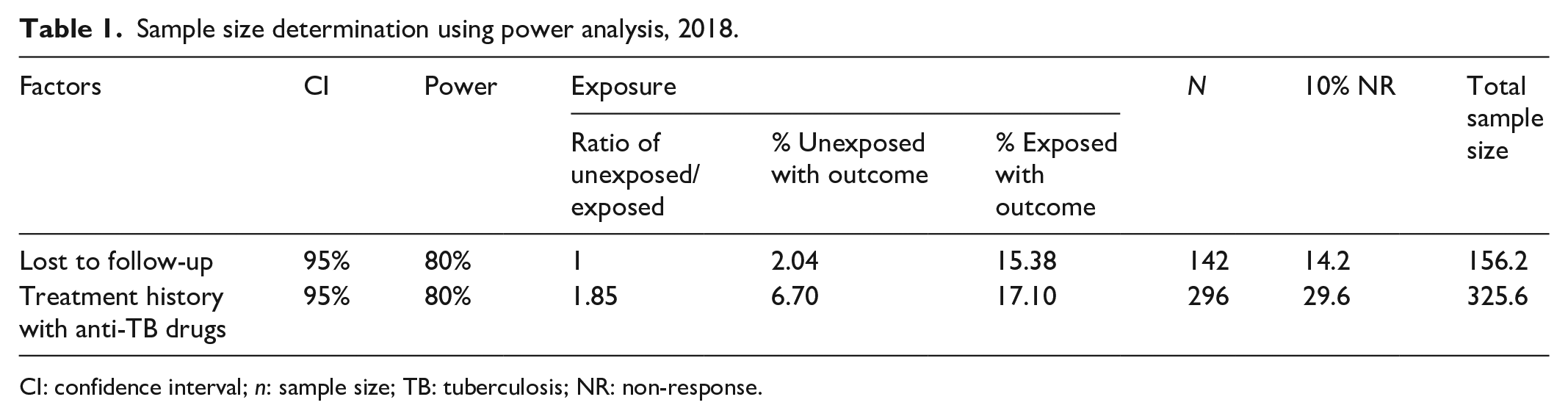
CI: confidence interval; n: sample size; TB: tuberculosis; NR: non-response.
where n is the sample size; Z is the standard normal distribution value at the 95% CI, which is 1.96; P is the prevalence of RR-TB, which is 2.3%; and D is the margin of error, taken as 0.05%.
Data collection
After written consent was obtained from all study participants, a structured questionnaire adapted from a previous study conducted in Kenya 27 and Ethiopia 17 was used to collect the socio-demographic, behavioral, environmental, and treatment-related characteristics. The questions were presented to the study participants by face-to-face interview (Supplement material).
Participants were instructed to bring a sputum specimen in a clean, sterile, and screw-cupped container. The sputum specimens were examined using GeneXpert (Cepheid). 28 Briefly, 1 mL of sputum was mixed with 2 mL of a buffered reagent to liquefy the sputum and incubated at room temperature for 10 min. After incubation, 2 mL was transferred to a cartridge in order to release the target DNA, and then the cartridge was loaded into GeneXpert (Cepheid) machines. The result was displayed on the computer screen after 2 h of processing.
Data management and quality control
The quality of data was ensured using standardized data collection materials and proper training. The questionnaire was pre-tested among 5% of the sample size at Hawassa University Comprehensive Specialized Hospital before the actual study was undertaken. All laboratory procedures were carried out according to Standard Operating Procedure (SOP). GeneXpert (Cepheid) assay has an inbuilt internal quality control (IQC) system within the test cartridge. Moreover, external quality control was also used.
Data analysis
Data were entered using Epi info version 7 and analyzed using SPSS (Statistical Package for Social science) version 20 computer software. Data were summarized using descriptive measures and presented in tables. Binary and multivariable logistic regressions were used to determine factors associated with the prevalence of RR/MDR-MTB. Variables from binary logistic regression with a p-value less than 0.2 were further analyzed by multivariable logistic regressions. A p-value <0.05 was considered as a significant association.
Results
Socio-demographic characteristics
A total of 321 TB suspected patients participated in this study, with a response rate of 98.5%. Most of the participants were within the age group of 29–39 years. The mean age of participants was 38.5 (±14.5). Out of the total study participants, male accounted for 184 (57.3%). Participants who completed the primary level of education accounted for 127 (39.6%). One hundred eight (33.6%) study participants earned less than 1000.00 Ethiopian Birr (ETB) per month (Table 2).
Socio-demographic characteristics of TB suspected patients at Adare General Hospital, Hawassa, South Ethiopia, 2018 (N = 321).

TB: tuberculosis; n: number.
Among the study participants, 72.9% and 8.1% reside in a house with two or less number of rooms and had a history of smoking cigarettes. Twenty-two (6.9%) of the participants had a history of TB treatment; 18 (81.8%) took the anti-TB drug for less than 6 months,14 (63.6%) took medication at the regular time, and 9 (40.9%) had a person to remind medication time (Table 3).
Behavioral, environmental, and treatment-related characteristics of TB cases visiting TB clinic at Hawassa Adare General Hospital, South Ethiopia, 2018.

TB: tuberculosis.
Prevalence of MTB and RR/MDR-MTB
From a total of 321 TB suspected cases, 98 (30.5%, 95% CI: 25.5%–35.8%) were positive for MTB. The prevalence of RR/MDR-MTB among TB suspected and confirmed TB cases was 1.24% (95% CI: 0.3%–2.8%) and 4.1% (95% CI: 1%–8.2%), respectively.
Factors associated with RR/MDR-MTB
From various factors assessed in this study, only the history of treatment with anti-TB drugs was significantly associated with the prevalence of RR/MDR-MTB. Participants with a past history of treatment with anti-TB drugs were more likely to develop RR/MDR-MTB (adjusted odds ratio (AOR), 16.70; 95% CI: 1.02, 273.59). Other factors such as urban residents, previous cigarette smoking, average monthly income, and history of imprisonment were not significantly statistically associated with the prevalence of RR/MDR-MTB (Table 4).
Factors associated with the prevalence of rifampicin-resistant/multidrug-resistant Mycobacterium tuberculosis among TB suspected cases attending Adare General Hospital, Hawassa, 2018 (N = 321).

TB: tuberculosis; RR/MDR-MTB: rifampicin-resistant/multidrug-resistant Mycobacterium tuberculosis; n: number; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; ETB: Ethiopian Birr.
Statistically significant (p-value <0.05).
Discussion
The prevalence of MTB found in this study (30.5%, 95% CI: 25.5%–35.8%) was high compared to the prevalence reported from Debremarkos, Ethiopia (23.1%), 17 Addis Ababa, Ethiopia (13.5%), 29 and Adama, Ethiopia (13.2%). 30 In contrast, it was low compared to reports from East Gojam, Ethiopia (32.2%). 31 The prevalence of MTB in this study was in line with the study conducted in Ghana (31.4%). 32 The variation might be due to socio-demographic factors, population differences, the case definition for inclusion, and the laboratory method used. Using molecular methods may yield high prevalence compared to AFB microscopy since it has high sensitivity.
The prevalence of RR/MDR-MTB we identified (4.1%, 95% CI: 0.3%–2.8%) was higher than the nationally reported prevalence of RR-MTB, which was less than 2%. 13 It was also higher than the globally reported prevalence of RR-TB, which was less than <1%.33,34 This variation could be explained by differences in socio-demographic factors, access to health care facilities, and differences in the study population.
Our finding was low compared to RR-MTB reported from Swaziland (7.7%). 35 However, it was in line with the prevalence of RR-TB reported from Ghana (4.52%) 32 and Congo (3.2%). 34 Unlike this study, a high proportion of RR-MTB (7.3%-23.4%) was reported from different parts of Nigeria.36–39 Low prevalence of RR-MTB (2.3%) from Debremarkos, Ethiopia 17 and comparable prevalence of RR-MTB from Gondar, Ethiopia were reported. 40 This variation could be attributed to socio-demographic factors, environmental factors, and differences in the study population.
In this study, 14.3% of participants with a history of TB treatment were positive for RR/MDR-MTB. Based on this finding, participants who had a previous history of treatment with anti-TB drugs were more likely to develop RR/MDR-MTB compared to participants without a history of previous TB treatment (p = 0.048). Similarly, a study from Nigeria2,37 and Brazil 41 reported a significant association between history of treatment and RR-MTB. Studies conducted in different parts of Ethiopia also reported an association between a history of treatment with the anti-TB drug and high prevalence of RR-MTB.17,20 These findings indicate that inappropriate exposure to anti-TB drugs could have increased the development of drug-resistant MTB by selecting drug-resistant MTB strains. Although a significant association was not observed, there was a high prevalence of RR/MDR-MTB among participants whose residence was in the urban area (6.8%), whose income was less than or equal to 2000.00 ETB (9%), those with a history of imprisonment (25%), and those who smoke a cigarette (14.3%).
Limitation of the study
Since the sputum sample was not collected under observation, the actual source cannot be confirmed. The participants may not remember all information asked during data collection; therefore, the data are not completely free of recall bias. As the number of positive cases are small, it is difficult to draw true association between dependent and independent variables. The convenience sampling technique we used also may have resulted in selection bias.
Conclusion
The prevalence of MTB among TB suspected patients at AGH was 30.5%. The prevalence of RR/MDR-MTB among TB confirmed cases was 4 (4.1%). The prevalence of RR-MTB among TB suspected cases was 1.24%. Study participants with a previous history of treatment with anti-TB drugs were more likely to develop RR/MDR-MTB. Early detection of drug-resistant MTB should be given enough attention to strengthen the management of TB cases and improve DOTs and eventually to minimize the spread of RR-TB strain in the community.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211045541 – Supplemental material for Prevalence of Mycobacterium tuberculosis infection and rifampicin resistance among presumptive tuberculosis cases visiting tuberculosis clinic of Adare General Hospital, Southern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121211045541 for Prevalence of Mycobacterium tuberculosis infection and rifampicin resistance among presumptive tuberculosis cases visiting tuberculosis clinic of Adare General Hospital, Southern Ethiopia by Degineh Belachew Andarge, Tariku Lambiyo Anticho, Getamesay Mulatu Jara and Musa Mohammed Ali in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank all staff of Adare General Hospital who were working at TB clinic for their support during data collection. We also acknowledge all study participants for their willingness to take part in the study.
Author contributions
D.B.A. designed the experiment, laboratory work, and data analysis T.L.A. designed the experiment, supervision, and analysis. G.M.J. designed the experiment, supervision, and analysis M.M.A. was involved in data analysis and manuscript preparation. All authors have read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Institutional Review Board of Hawassa University College of Medicine and Health Sciences (Reference number: IRB162/10). The purpose and procedure of the study were explained to the study participant. Data were collected after written informed consent was obtained from participants. All methods were carried out in accordance with relevant guidelines and regulations as mentioned by the Declaration of Helsinki.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Data availability
All relevant data are available within the paper.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.