
Abstract
Background:
Alcohol use disorder is one of the primary causes of avoidable death, illness, and injury in many societies throughout the world. Although alcohol use disorder can influence the natural history of a disease, disease recurrence, quality of life, and treatment adherence in psychiatric patients, the data on its magnitude is scarce.
Objectives:
This study was aimed to determine the magnitude of alcohol use disorder and its determinants among patients with schizophrenia attending a mental specialized hospital in Addis Ababa, Ethiopia.
Methods:
An institutional-based cross-sectional study was conducted from May 15 to June 15, 2018. An alcohol use disorder identification test was employed among a sample of 414 randomly selected patients with schizophrenia. Alcohol use disorder was categorized as hazardous drinking (Alcohol Use Disorders Identification Test (AUDIT) score of 8–15), harmful drinking (AUDIT score of 16–19), and alcohol dependence (AUDIT score of 20 or above). The data were entered into Epi-Data 3.1 and exported to SPSS 20 for analysis. Logistic regression was fitted to identify factors associated with alcohol use disorder.
Results:
The prevalence of alcohol use disorder was 38.4% (95% confidence interval (CI) 33.7, 42.9). Of this, 22.4% of the patients had hazardous drinking, 8.4% harmful drinking, and 7.6% alcohol dependence. Factors associated with alcohol use disorder were male sex (adjusted odds ratio (AOR) = 5.8, 95% CI 2.55, 13.19), being single (AOR = 3.0, 95% CI 1.63, 5.51), divorced (AOR = 4.3, 95% CI 1.95, 9.47) and widowed (AOR = 3.5, 95% CI 1.39, 8.81), having family history of alcoholism (AOR = 3.8, 95% CI 1.98, 7.19), longer duration of illness (AOR = 3.9, 95% CI 1.83, 8.36), previous history of psychiatric diagnosis (AOR = 2.2, 95% CI 1.1, 4.34), and concomitant use of non-alcoholic substances (AOR = 3.7, 95% CI 2.06, 6.74).
Conclusions:
Almost four in ten patients with schizophrenia had alcohol use disorder. Male sex, single, divorced, and widowed, family history of alcohol use, long duration of illness, previous history of psychiatric diagnosis, and concomitant use of non-alcoholic substances were significantly associated with alcohol use disorder. Continuous counseling of at risk populations about alcohol consumption should be strengthened.
Introduction
Alcohol is a psychoactive substance with dependence-producing properties that has been extensively used in many cultures for centuries. Harmful use of alcohol leads to a widespread health problem as well as socio-economic burdens in societies.1–3 Alcohol ranks among the top 10 risk factor causes of disability-adjusted life years (DALYs) lost, both internationally and in all three income categories of countries. It has been estimated that 4.4% of DALYs lost are due to alcohol. 4
Alcohol use disorder (AUD) is a major cause or increases the risk for many health-related problems and complicates their treatment. 5 It has a major impact on public health and is a contributory factor for about 60 categories of diseases and injuries6–8 and 2.9 million deaths globally. 9 AUD is common in the general population, the risk is 2 times higher among psychiatric patients. 10 Such co-morbid conditions prolong the duration of the psychiatric disorder, higher rates of homelessness, increase the frequency of admissions, and lead to lower quality of life and social complications.11–13
Almost half of the schizophrenic patients have a co-morbid substance use disorder during their lifetime. 14 Many studies done throughout the 20 years show an increase of co-morbidity of disorders caused by harmful use or abuse of alcohol and other psychoactive substances in the population of schizophrenia.15,16 An additional diagnosis of AUD can affect the natural history of a disease, disease recurrence, patient quality of life, and treatment compliance in patients with schizophrenia. Higher proportions of drinkers had a longer duration of schizophrenic illness and longer in-patients stay on a mental health ward.17–19
Since AUDs can negatively affect compliance to treatment, effectiveness of medications, and increases the rate of hospitalization, there is a huge necessitate for screening and diagnosing co-morbid AUDs among patients with psychiatric disorders.20,21 Most patients in low and middle-income countries with severe psychiatric disorders do not get management for their mental illness including for their concurrent drug addiction in general.22–24 Therefore, early identification of AUD can be useful to prevent several complications, as well as an intervention opportunity to propose an integrated treatment to dual diagnosis patients.
Although a variety of traditional and modern alcoholic drinks are recognized to be used extensively in Ethiopia, to the level of our knowledge very limited studies have been conducted to determine the prevalence of AUD among patients with mental illnesses. So, this study was conducted to assess the magnitude of AUD and its associated factors among patients with schizophrenia attending care at a specialized mental hospital in Ethiopia.
Material and methods
Study setting and period
The study was conducted in Amanuel Mental Specialized Hospital (AMSH) located in Addis Ababa, the capital of Ethiopia. It is the only specialized mental hospital giving the service for patients with psychiatric disorders coming from the whole countryside. Of 61,580 patients who received treatment in 2017, 16,615 were related with schizophrenia. On average, about 2700 outpatients with schizophrenia get follow-up services each month. The study was conducted from 15 May to 15 June 2018.
Study design and population
A cross-sectional study was conducted. The source population included patients with schizophrenia on follow-up treatment at AMSH while the study adult population included patients who were diagnosed as per the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) or 5th Edition (DSM-5) criteria, and on follow-up at hospital during the study period.
Inclusion criteria
Participants age 18 years and above were included in the study.
Exclusion criteria
Patients who were severely ill and not capable to give required information were excluded from the study.
Sample size determination and sampling technique
The sample size was estimated using single population proportion formula with 95% confidence interval (CI), 5% marginal error, 10% non-response rate, and the proportion of AUD of 42.7% (prevalence taken from a study conducted at Jimma, southwestern Ethiopia). 25 Finally, the estimated sample size is 414. Using systematic random sampling technique, every other patient was included in the study after the first one was selected randomly.
Study variables
Dependent variables: Alcohol use disorder.
Independent variables:
• Socio-demographic factors: age, sex, marital status, educational status, residence, and occupation.
• Clinical factors: duration of illness, chronic medical illness, and previous history of a psychiatric diagnosis other than schizophrenia.
• Other substance use: Khat, Nicotine, and others.
Operational definitions
Alcohol use disorder: “A total Alcohol Use Disorders Identification Test (AUDIT) score of eight or more was used to define probable ‘alcohol use disorder.’ A total AUDIT score of 1–7 indicated social drinking, a score of 8–15 indicated ‘hazardous drinking,’ a score of 16–19 indicated ‘harmful drinking,’ and a score of 20 or above indicated probable alcohol dependence.” 26
Chronic medical illness: additional co-morbid chronic medical illness with schizophrenia.
Previous history of psychiatric diagnosis: having a previous history of mental illness other than schizophrenia.
Concomitant Substance use: those who use any substance (khat, tobacco, and others) other than alcohol.
Data collection tools and procedure
The Alcohol Use Disorders Identification Test (AUDIT) was used to collect data. AUDIT is a 10-item alcohol screening instrument and emphasizes the identification of AUD in the last 12 months. AUDIT, developed by the World Health Organization, has been found to be effective in identifying people with a drinking problem such as hazardous drinking, harmful drinking, and alcohol dependence. 26 The Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) (V.3.1) was used to assess the substance use of the respondents other than alcohol. 27 Clinical characteristics were obtained from yes/no answers of respondents and patients’ medical records.
Data were collected by five trained psychiatric nurses. Data collectors and supervisors were trained for 2 days on the purpose of the study, details of the questionnaire, interviewing techniques, the importance of the privacy, and ensuring the patients’ confidentiality.
Data quality control
Data were collected using a standardized questionnaire which was translated into the local language (Amharic) and back to English by individuals with good command of English. The questionnaire was pretested on 5% of the sample size on schizophrenic patients in St. Paul’s Hospital Millennium Medical College.
Data processing and analysis
The data were processed using Epidata version 3.1 and analyzed using SPSS version 20. Findings were described using percentages and frequencies. Bivariable and multivariable logistic regression was fitted to identify factors associated with AUD. Association was described using odds ratio (OR) along with its 95% CI. 28 Variables with p-value < 0.25 in the bivariable logistic regression were entered into the multivariable logistic regression. Finally, variables with p-value < 0.05 in the multivariable logistic regression were considered as significantly associated with AUD.
Ethical considerations
Ethical clearance was obtained from the Ethical Review Committee (ERC) of AMSH (Ref NO: Am/146/4/214). Before the questionnaire was administered, informed voluntary written consent was obtained from each study participant. Confidentiality was maintained at all levels of the study through collecting anonymous data. Patients with AUD were linked to substance-related specialist.
Results
Socio-demographic description
Among 414 psychiatric outpatients enrolled in the study, 406 consented to participate, resulting in a response rate of 98%. The mean age of the respondent was 36.6 (± 10.2 SD) years. Majority of the respondents were males (77.3%), live in urban areas (76.1%), and unemployed (67.5%). Close to four in ten (38.2%) respondents attended secondary school (Table 1).
Description of socio-demographic characteristic of respondents at AMSH, Addis Ababa, Ethiopia, 2018.

AMSH: Amanuel Mental Specialized Hospital; SD: standard deviation; other religion: Catholic, Wakefata; other ethnicity: Wolayta, Silte, Tigre.
Clinical characteristics of the study participants
Half of the respondents (50.0%) had above 5 years duration of illness and 40.6% were using non-alcoholic substances. About 7.6% of the patients had additional medical illnesses, of those hypertension was the most common (3.9%) followed by diabetes mellitus (2.5%). A total of 71.7% participants reported family history of alcohol use and 20.7% had previous history of a psychiatric diagnosis other than schizophrenia (major depressive disorder (9.6%) and bipolar disorder (8.4%) (Table 2).
Description of clinical characteristic of study participants at AMSH, Addis Ababa, Ethiopia, 2018.

AMSH: Amanuel Mental Specialized Hospital; other substance: cannabis, other traditional substance.
Prevalence of alcohol use disorder
The overall prevalence of AUD was 38.4% (95% CI 33.7, 42.9). Of this, 91 (22.4%) had hazardous drinking, 34 (8.4%) harmful drinking, and 31 (7.6%) alcohol dependence. Most of the respondents (61.6%) were social drinkers (Figure 1).

Alcohol use disorders among schizophrenic patients according to their degree (level) of severity at AMSH, Addis Ababa Ethiopia, 2018.
Factors associated with alcohol use disorder
In the bivariable analysis, sex, marital status, level of education, living arrangement, job, family history of alcohol use, duration of illness, previous history of a psychiatric diagnosis, co-morbid medical illness, and other non-alcoholic substance use were significantly associated with AUD. In the multivariable logistic regression, however, only gender of respondent, marital status, family history of alcohol use, duration of illness, previous history of a psychiatric diagnosis, and non-alcoholic substance remained statistically significant at p-value < 0.05.
Males were 6 times (adjusted odds ratio (AOR) = 5.8, 95% CI 2.55, 13.19) more likely to have AUD compared with females. Being single (AOR = 3.0, 95% CI 1.63, 5.51), divorced (AOR = 4.3, 95% CI 1.95, 9.47), and widowed (AOR = 3.5, 95% CI 1.39, 8.81) was also significantly associated with AUD. Patients who reported a family history of alcoholism were four times (AOR = 3.8, 95% CI 1.98, 7.19) more likely to have AUD. The odds of having AUD was 3.9 (AOR = 3.9, 95% CI 1.83, 8.36) among patients with longer duration of illness as compared with patients having the illness less than 5 years. Patients who had a previous history of a psychiatric diagnosis other than schizophrenia were more likely to have AUD (AOR = 2.2 95% CI 1.1, 4.34) as compared with patients not having a previous history of a psychiatric diagnosis other than schizophrenia. Patients who reported using non-alcoholic substances were four time (AOR = 3.7 95% CI 2.06, 6.74) to have AUD as compared with those not reported using non-alcoholic substances (Table 3).
Factors associated with alcohol use disorder among patients with schizophrenia at AMSH, Addis Ababa, Ethiopia may, 2018.
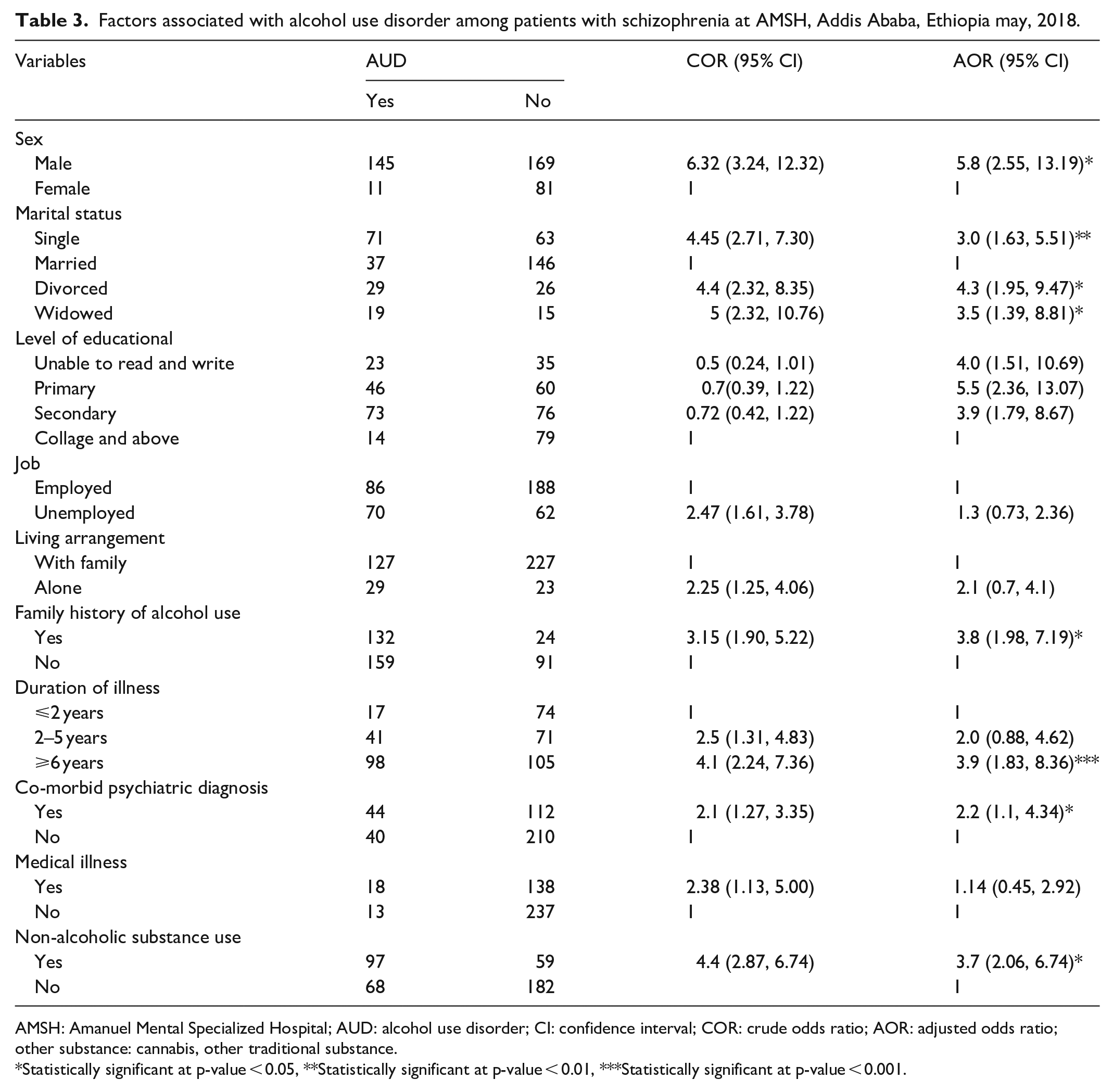
AMSH: Amanuel Mental Specialized Hospital; AUD: alcohol use disorder; CI: confidence interval; COR: crude odds ratio; AOR: adjusted odds ratio; other substance: cannabis, other traditional substance.
Statistically significant at p-value < 0.05, **Statistically significant at p-value < 0.01, ***Statistically significant at p-value < 0.001.
Discussion
In this study, AUD and its associated factors were assessed among schizophrenic patients attending a specialized mental health hospital in Addis Ababa. We found that almost four in ten (38.4%) of schizophrenic patients had AUD. Of this, 22.4% had hazardous drinking, 8.4% had harmful drinking, and 7.6% had alcohol dependence. Most of the respondents (61.6%) were social drinkers. Factors associated with AUD were being male, single, divorced and widowed, family history of alcoholism, longer duration of illness, having previous history of a psychiatric diagnosis, and using non-alcoholic substance.
This finding is consistent with previous studies in Ethiopia, Jimma (42.7%) 25 and Gondar (36.2%), 29 South Africa (41.2%), 30 Australia (38%), 31 and Switzerland (35.1%). 32 This indicates AUD is a challenge among patients with schizophrenia regardless of settings. Given the challenge of being on long term antipsychotic drug therapy, schizophrenia patients require a buddy that would support in the adherence process and/or counsel on the hazards of alcohol on their health and adherence process.
The result is, however, higher than community-based studies from Addis Ababa (2.7%) 33 and Butajira (3.7%), 34 Ethiopia. It is similarly higher than findings from primary care clinics in South African (17.6%), 35 and population-based studies in Thailand (10.9%) and Singapore (3.6%).36,37 In addition to the difference in the study setting—a specialized mental health hospital and community based, the difference might be attributed to the difference in the identification tool vs. Cut down, Annoyed, Guilty, and Eye-opener (AUDIT vs. CAGE). Relatively, CAGE is designed to detect more severe AUDs and therefore could underreport the burden. Studies from Tanzania, Australia, and United State reported higher proportion of AUD, 59.3%, 38 77.3%, 39 and 57%, 17 respectively. This could be explained by the difference in the study population and design.
In congruent with studies conducted in Ethiopia, 25 Tanzania, 38 Kenya, 40 India, 41 and Serbia, 42 males were more likely to have AUD compared with females. Given the overall lower alcohol consumption among females, compared with males, this result was not unexpected. It was likely both psychosocial and biological etiologies lead to the greater risk of AUD in men. Males are known to engage in risky behaviors, including heavy alcohol consumption, and this is considered a male norm.43,44
Being single, divorced, and widowed was also significantly associated with AUD. This finding was consistent with studies in Nigeria, 45 India, 46 and Brazil. 47 This could be explained by the fact that single persons were free of family control and consumed alcohol as married persons. In addition, they were able to make independent decisions throughout their lives and results in participating in alcoholic beverages. The other reason might be single in marital status had less responsibility to their family than married one and they participated in drinking than their counterparts.
Patients with family history of alcoholism were found to have AUD compared with their counterparts, a result which was reported in Jimma 25 and Sweden. 48 This is due to both schizophrenia and AUDs have biological/heredity effects, the overlap between alcohol use problems and other psychiatric problems could indicate similar etiological factors in the development of such problems. In line with a study reported in India, schizophrenic patients with longer duration (>6 years) were more likely to have AUD. 46 Patients who had a previous history of a psychiatric diagnosis other than schizophrenia were more likely to have AUD as compared with patients not having a previous history of a psychiatric diagnosis other than schizophrenia. This might be because people with such diagnoses have highly impaired judgment and insight as well as aggressiveness and uncontrolled emotions. This was supported by a study conducted in Sweden. 48
Patients who reported using substance other than alcohol (smoking and Khat) were more likely to have AUD. A similar findings were reported from Jimma, 25 Serbia, 42 and Sweden. 48 It was widely believed that schizophrenic patients smoke to increase hepatic clearance and to restore the dopamine blockage of certain antipsychotic medications to diminish their side effects.28,49 More recently, it became obvious that cigarette smoking may also be reinforcing for patients because it improves psychiatric symptoms, most notably negative and cognitive symptoms.50,51 However, there is little support for this view, as clinical studies are lacking and the results of available studies are not conclusive. In addition, it might be due to behavioral concordance of using one type of substance with other substances, and, perhaps the illness dictates the use of multiple substances at the same time.
Limitation of the study
This study has some important limitations that should be kept in mind when interpreting the results. The cross-sectional nature of the study design does not confirm a definitive cause-and-effect relationship. Some variables like duration of illness and family history of alcohol use rely on the patient’s history that might have recalled bias which could be higher among schizophrenic patients. Social desirability bias regarding alcohol use might be introduced as the result of the face-to-face interview in the vicinity of the hospital.
Conclusions
Almost four in ten patients with schizophrenia suffer from AUD. Being male sex, single, divorced and widowed, having family history of alcohol use, long duration of illness, previous history of psychiatric diagnosis, and using non-alcoholic substance use were significantly associated with AUD. Strong screening for alcohol and counseling on its effect on schizophrenic patients should be instituted. There is a need for objective measuring system for AUD.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211048748 – Supplemental material for Alcohol use disorder and its determinant factors among patients with schizophrenia attending treatment at mental specialized hospital, Addis Ababa, Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121211048748 for Alcohol use disorder and its determinant factors among patients with schizophrenia attending treatment at mental specialized hospital, Addis Ababa, Ethiopia: A cross-sectional study by Habtamu Tadesse, Yohannes Mirkana and Tadesse Misgana in SAGE Open Medicine
Footnotes
Acknowledgements
We thank the Amanuel Mental Specialized Hospital for facilitating the research work. We also thank the data collectors, supervisors, and the study participants.
Author contributions
H.T. conceived and designed the study. H.T., Y.M, and T.M. adopted data collection instruments and acquisition of data. H.T., Y.M, and T.M. carried out the data management. H.T. analyzed the data and interpreted findings. T.M. drafted the manuscript with a critical revision from H.T. and Y.M. All authors read the final version and approved for submission.
Data availability
The data used to support the findings of this study are available from the corresponding author upon a reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Ethical Review Committee of Amanuel Mental Specialized Hospital (approval number: Am/14604/214).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.