
Abstract
Objective. Improving diagnostic ability of pediatric sepsis is of great significance for reducing the mortality of sepsis. This study explored the discriminatory capacity of nutritional index (PNI) in pediatric sepsis. Methods. We retrospectively enrolled 134 children with suspected sepsis and collected their clinical and laboratory data. Receiver operating characteristic curves (ROC), decision curve analysis (DCA) and net reclassification improvement (NRI) were performed to compare the predictive significance of the PNI, procalcitonin (PCT) and their combination. Results. Among 134 patients, 65 children were diagnosed with sepsis and 69 children with non-sepsis. PCT and PNI were independently associated with pediatric sepsis. PCT was superior to PNI to predict pediatric sepsis. The model based on PCT + PNI improved the predictive capacity than them alone, as demonstrated by ROC, DCA and NRI, respectively. Conclusion. PNI was independently associated with pediatric sepsis, and addition of PNI could improve the capacity of PCT to predict pediatric sepsis.
Background
Pediatric sepsis is a major public health problem across the worldwide, which is considered as a leading cause of death for children. 1 Although mortality of sepsis in children has presented a great decline, the morbidity of pediatric sepsis has shown an increase in the past 20 years. 2 Therefore, it is great of importance for early recognition of pediatric sepsis in order to improve prognosis.
Currently, several biomarkers have been widely used to rapidly discriminate pediatric sepsis, such as C-reactive protein (CRP), procalcitonin (PCT), pediatric risk of mortality score (PRISM III), while there is so far no single biomarker that could accurately diagnose sepsis. 3 Accumulating evidence has indicated that the systemic inflammatory and nutritional markers, for example, neutrophil-to-lymphocyte ratio (NLR), 4 platelet-to-lymphocyte (PLR), 4 C-reactive protein-to-albumin ratio (CAR) 5 have been extensively investigated to predict sepsis in adult. Recently, Zhong et al found that NLR was a potential index for predicting severe pediatric sepsis, and the combination of NLR, PCT and PRISM III was superior to them alone. 6 In addition, NLR 7 and CAR 8 also showed the association with neonatal sepsis risk. To this respect, these data imply that the systemic inflammatory and nutritional markers may provide us helpful value for discriminating sepsis.
The prognostic nutritional index (PNI), a novel inflammatory index is calculated based on peripheral lymphocyte count and level of serum albumin (Alb), which is considered as a parameter for individual nutritional and immune status, and is associated with prognosis of various cancer9,10 and inflammatory diseases, such Kawasaki disease, 11 septic acute kidney injury 12 and mortality of sepsis in adults. 13 The study reported by Li et al indicated that PNI was associated with the presence of neonatal sepsis. 14 Thus, we speculate that PNI could be useful in the discrimination of pediatric sepsis. However, there are no available published investigation regarding the predictive value of PNI for sepsis in children. PCT is a commonly used parameter in clinical settings for predicting sepsis with high specificity. However, it is important to note that PCT values can also be elevated in non-septic conditions, resulting in false-positive results.15,16 Multiple efforts are advised to identify sepsis, 3 which should improve the accuracy. It has not been reported whether PNI could enhance the ability of PCT to predict sepsis in children to date.
In current study, we aimed to evaluate the following hypotheses: (Ⅰ) PNI could discriminate pediatric sepsis; and (Ⅱ) compared with PCT alone, the discriminative ability could be improved by the combination of PNI and PCT.
Methods
Patients
A retrospective, single-center study was conducted in this study. A total of 134 children with suspected sepsis were admitted to the Affiliated Hospital of Southwest Medical University from January 2016 to December 2016. Suspicion of sepsis must have fever (rectal temperature > 38.5℃) or hypothermia (rectal temperature <35℃) and suspected infection, plus 1 or more of the following standard: (1) Tachypnoea or respiratory distress; (2) Tachycardia or mottled, cold or pale skin; (3) Irritability, food rejection, altered mental status, fainting or meningeal signs; (4) Petechiae or ecchymosis. 17 Sepsis was defined as having fever (rectal temperature > 38.5℃) or hypothermia (rectal temperature <35℃), tachycardia (without tachycardia in hypothermia), with at least one of the following organ dysfunction: altered consciousness, hypoxemia, elevated serum lactate, or bounding pulse. 18 The inclusion of criteria: (Ⅰ) patient with suspected sepsis; (Ⅱ): 28 days < age < 18 years. There were the following exclusion criteria: (Ⅰ) younger than 28 days or older than 18 years; (Ⅱ) incomplete laboratory data including total and differential leukocyte counts, albumin (Alb), platelet counts (PLT), procalcitonin (PCT), and CRP; (Ⅲ) repeated admissions; (Ⅳ) subjects with hematological system, digestive diseases, immunological system, chronic inflammatory disease, heart diseases, malignancies, malnutrition and hypoproteinemia. In our study, we contained septic shock in sepsis. Among all cases with suspected sepsis, the cases were considered as the non-sepsis group excluding the cases diagnosed with sepsis. This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and proved by the ethics committee of Affiliated Hospital of Southwest Medical University (No.KY2024061). In this retrospective analysis, individual consent was waived.
Data Collection
From electronic medical records, patient demographics, diagnostic and laboratory results within 24 hours of admission were collected. Laboratory findings were collected, such as white blood cell (WBC), neutrophil, lymphocyte, and PLT counts, CRP, PCT, and Alb. NLR, PLR, and CAR were calculated as described by Li et al.11,19 PNI = Alb (g/L) + 5 × total lymphocyte count (109/L).
Statistical Analysis
Statistical analyses were done with SPSS version 22.0 (IBM Corp., USA), the logreg package of R 6.2.0 software, the rmda package of R 1.6 software and sklearn package of Python 0.22.1 software. Continuous data were presented as the median (interquartile range) or mean± standard deviation (SD), and were compared with independent t-test or Mann–Whitney U test, as appropriate. Categorical data were shown as numbers (percentage), and were compared with Chi-square test. Variables with a P-value < .05 in the univariate logistic regression analysis were used for the multivariate logistic regression analysis. The independent risk factors were used to establish a nomogram. The receiver operating characteristic (ROC) was constructed to assess the predictive value of PCT, PNI and the model based their combination. The method of DeLong’s test was selected to compare the difference among them. In addition, the discriminative ability also was assessed with calibration plot, decision curve analysis (DCA) and net reclassification improvement (NRI). A 2-sided P value < .05 was considered statistically significant.
Results
Baseline Characteristics for the Study Population
The demographic and laboratory findings were shown in Table 1. Among 134 children with suspected sepsis (median age 11.0[3.0, 35] months), there were 63 males (47.02%), and there were 70.9% patients with respiratory diseases. Sixty-five patients were finally diagnosed with sepsis, while the rest of 69 patients having signs of infection were considered as the non-sepsis group. Compared with the non-sepsis group, the sepsis group had higher NEU, CPR, PCT, NLR, and CAR, and lower PNI, LYM, PLT as well as Alb (all P < .05). There were insignificant differences between 2 groups regarding gender, age, weight, WBC, Hb, PLR, the occurrence of respiratory infection.
Baseline Characteristics for Non-Sepsis Group and Sepsis Group.

Abbreviations: CRP, C-reactive protein; PNI, prognostic nutritional index; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; CAR: creactive protein to albumin ratio; PLT, platelet counts; WBC, White blood cell; LYM, Lymphocytes, NEU, neutrophils; PCT, procalcitonin.
Correlation Between PNI and Biomarkers of Sepsis
The correlation analysis showed that PNI was inversely associated with CRP (r = −.4529, P < .0001) and PCT (r = −.3606, P < .0001) (Figure 1A and B), respectively.
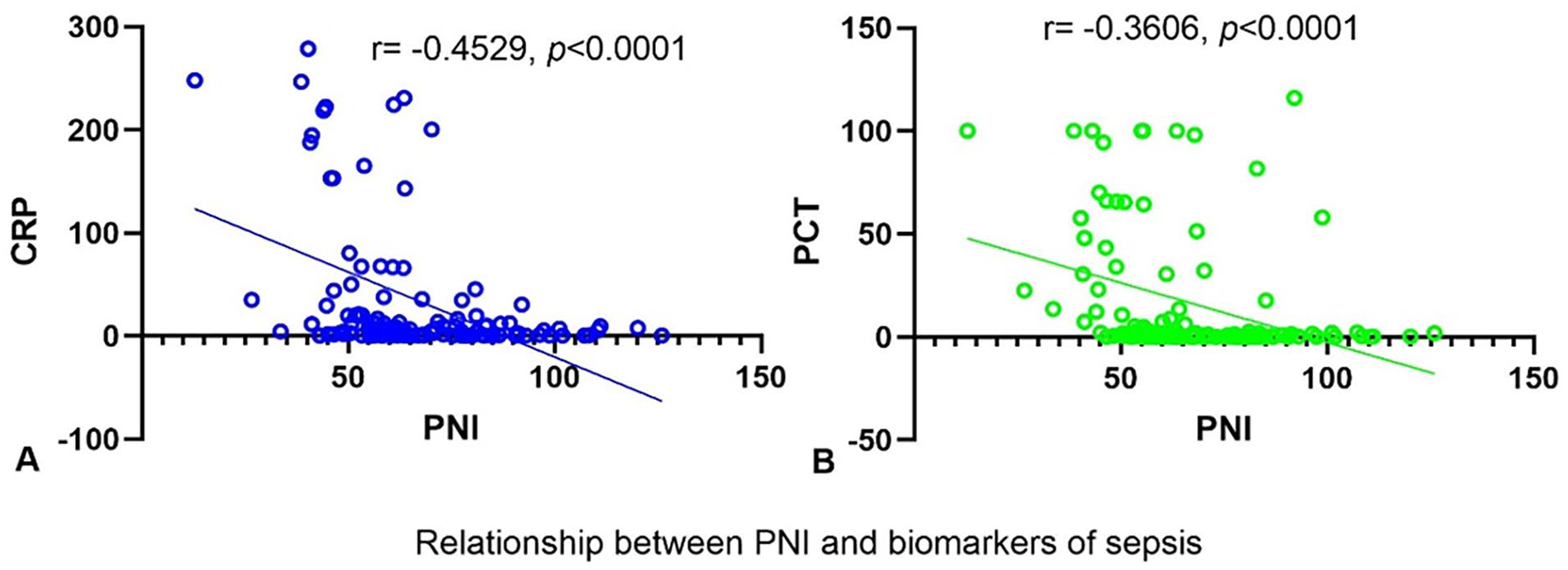
Correlation between PNI and CRP (A)/PCT(B).
Logistic Regression Analysis
Univariate logistic analysis was performed to assess the association of potential variables with the presence of sepsis. The results indicated that PCT (P = .001), NLR (P = .001), PLR (P = .036), CAR (P = .004) and PNI (P < .001) were considered be the risk factors for sepsis (because NEU, LYM, PLT, CRP and Alb had been included in NLR or CAR or PLR, they were excluded from the analysis). Multivariate logistic analysis showed that PCT (P = .006) and PNI (P = .028) were independently associated with presence of sepsis (Table 2).
Univariate and Multivariate Logistic Analysis in Relation to Sepsis.

Abbreviations: PNI, prognostic nutritional index; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; CAR, C-reactive protein to albumin ratio.
Diagnostic Performance of PCT and PNI
The area under the receiver operating characteristic curve (AUC), sensitivity, specificity of PCT and PNI to predict sepsis were presented in Table 3 and Figure 3A. The AUC for PCT was 0.848 with 72.3% sensitivity and 94.2% specificity, while the AUC for PNI was 0.766 for prediction of sepsis, yielding 91.3% sensitivity and 47.7% specificity.
Values of PCT, PNI and Their Combinations on the Basis of ROC Curves.
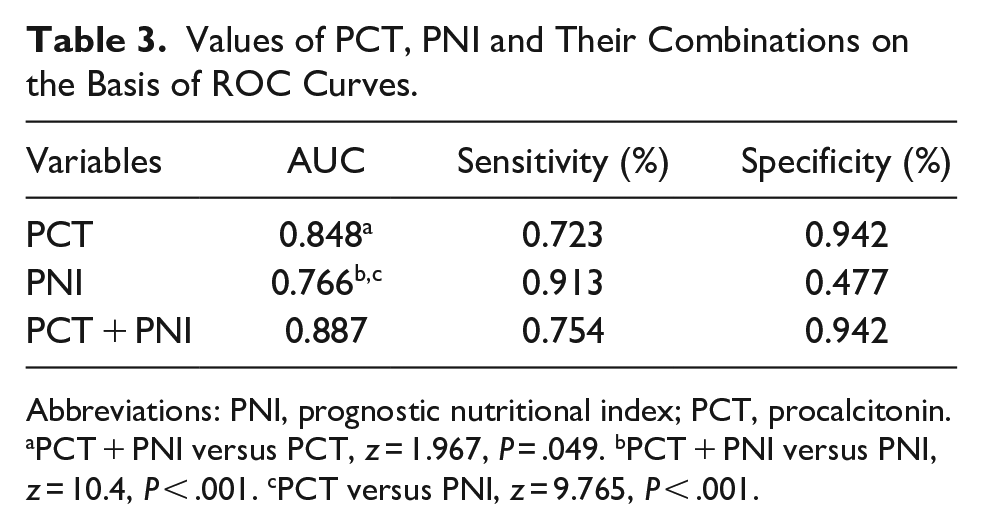
Abbreviations: PNI, prognostic nutritional index; PCT, procalcitonin.
PCT + PNI versus PCT, z = 1.967, P = .049. bPCT + PNI versus PNI, z = 10.4, P < .001. cPCT versus PNI, z = 9.765, P < .001.
Predictive Value of Constructed Model
Based on the results of multivariate logistic analysis, we selected PCT and PNI for establishing a nomogram to predict sepsis probability (Figure 2). The ROC for nomogram model was developed. The AUC of the nomogram was 0.887, which was significantly higher than that of the PCT-alone (z = 1.967, P = .049) and PNI-alone (z = 9.765, P < .001), respectively (Table 3 and Figure 3A). Meanwhile, calibration plot of nomogram model showed a good calibration for predicting sepsis (Figure 3B). Next, to further compare the power of nomogram model with PCT and PNI alone, DCA and NRI were performed. In DCA, nomogram model indicated a better benefit compared to PCT and PNI alone (Figure 3C). Additionally, nomogram model improved the predictive ability of sepsis by 15.1% (P < .05) and 60.4% (P < .05) of NRI compared with PCT and PNI alone, respectively.

Nomogram for predicting the presence of sepsis.

Evaluation for the nomogram model. (A) Receiver operating characteristics curve (ROC) comparison of PCT, PNI and nomogram model; (B) Calibration plot for nomogram model; (C) Decision curve analysis of PCT, PNI and nomogram model.
Discussion
The main finding of this study was that NLR, CAR and PNI were associated with pediatric sepsis, while only PNI was independently associated with pediatric sepsis. Moreover, PNI was useful in discriminating pediatric sepsis, which added to diagnostic potential of PCT for differentiating pediatric sepsis.
Sepsis is considered as a life-threatening disease with organ dysfunction caused by a dysregulated host response to infection. Remarkable inflammatory cytokines are up-regulated because of excessive inflammation in the early stage of sepsis, leading to the development of organ damage and dysfunction, ultimately resulting in death. 20 Early prediction of pediatric sepsis would be essential to decreasing organ system injury and mortality. Although several screening tools available or biomarkers have been used to discriminate sepsis, imperfect sensitivity and specificity for them can influence the clinician’s diagnosis. 21
PNI is calculated based on serum Alb level and total lymphocyte count in peripheral blood, which is widely used to assess the nutritional status and inflammation. In the present study, PNI was decreased in sepsis group, and was negatively associated with pediatric sepsis, having the capacity for discriminating pediatric sepsis. Similarly, PNI also was found to be a potential predictor for neonatal sepsis. 14 Sepsis could easily cause liver dysfunction, leading to dysfunction of synthesis and metabolism, finally affecting the nutritional status of patients. On the one hand, studies have confirmed that close association between serum Alb level and inflammation has been found, and serum Alb level was negatively correlated to severity of inflammation in adult patient.22,23 In addition, decreased serum Alb level were widely found in sepsis in adult.5,24 On the other hand, lymphocytes also play vital role in the regulation of inflammation, and decreased lymphocytes due to apoptosis induced by continuous sepsis may lead to loss of anti-inflammatory cytokines, and then enhance inflammatory response. Thus, lower PNI could be a potential predictor for pediatric sepsis. Additionally, our data also observed that PNI was inversely associated with traditional biomarker of sepsis and inflammation such as CRP and PCT. These data further support our hypothesis that PNI was a potential biomarker for discriminating pediatric sepsis. Previous studies showed that NLR 7 and CAR8,25 were the predictors for neonatal sepsis, and according to the meta-analysis of 14 studies, Huang et al 26 found that NLR had the ability for predicting sepsis in adult, while similar results was not found in this study. The discrepancy may attribute to different age, subject, sample size.
Accumulating evidence confirm that multiple biomarkers or model could improve the predictive power compared with single index.3,6,27 In current study, the predictive capacity of PCT was superior to PNI, implying that as a traditional diagnostic marker for sepsis, PCT has excellent predictive ability. The predictive significance of combination of PNI and PCT was further assessed. The constructed predictive model of PCT + PNI showed a better predictive capacity than that of PCT and PNI alone, as demonstrated by multiple statistical methods such as AUC, DCA and NRI. As there is little or no emphasis on the model based on PNI and PCT to predict sepsis in children, the current results firstly indicated that the addition of PNI could improve the capacity of PCT to predict pediatric sepsis. PNI is easily available and inexpensive, and can be accurately calculated through routine testing, which would help to improve the accuracy of pediatric sepsis diagnosis in clinical practice.
However, a few limitations should be considered. Firstly, this study was retrospective design conducted in a single center. Thus, the predictive ability of PNI might not be applicable to other regions. Secondly, our sample size was small and unidentified confounders might not have been detected. Thus, there is potential confounding factors. Thirdly, we ignored patients who received human albumin infusion therapy. Finally, we only measured the parameters within 24 hours of admission, and did not further collect the dynamic changes of these parameters. In addition, the sample size calculation was ignored, which might affect the present results. We would address these issues through multiple-center, large-sample and prospective studies in future research.
Conclusion
PNI was independently associated with pediatric sepsis. Moreover, addition of PNI could improve the capacity of PCT to predict pediatric sepsis. The findings highlight the potential ability of PNI as a convenient, inexpensive and easily available index in routine testing to predict the risk of pediatric sepsis.
Footnotes
Author Contributions
Deng Hongya: acquisition, drafted the manuscript and interpretation of data; Deng Linfan: acquisition and critically revised manuscript; He Chunyuan, Jiang Jun and Liu Bin: analysis; Zhao Jian: conception, design, and final approval; Li Gang: conception, design, final approval and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Data Availability Statement
The data presented in this study can be obtained from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Sichuan Science and Technology Program (NO. 2022YFS0627) and Luzhou Municipal People’s Government-Southwest Medical University Science and Tech-nology strategic cooperation (NO. 2023LZXNYDJ042).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the ethics committee of Affiliated Hospital of Southwest Medical University.