
Abstract
Introduction. Neonatal sepsis is the primary cause of increased newborn morbidity and mortality worldwide, particularly in developing countries. In Ethiopia, the factors of neonatal sepsis are not well understood. Therefore, the purpose of this study was to determine the factors associated with neonatal sepsis in the study area. Methods. A case-control study design was conducted among 60 cases and 120 controls. Variables with P ≤ .25 in the bivariate analysis were entered into multivariable logistic regression, and statistical significance was declared at P < .05. Result. Birth weight <2500-g (AOR = 4.05 [1.44, 11.36], number of ANC visits <3 (AOR = 4.49 [1.70, 11.86], duration of rupture of membrane ≥18 hours (AOR = 4.42; [2.02, 9.66], first minute APGAR score <7 (AOR = 3.09 [1.10, 8.70], birth at a health-center (AOR = 0.22 [0.08, 0.60]) and instrumental delivery (AOR = 0.30 [0.10, 0.88]
Introduction
Neonatal sepsis is a systemic inflammatory response to the presence of or as a result of suspected or proven infection in a neonate, and it may be bacterial, viral, fungal, or rickettsia in origin.1,2 In neonatal intensive care units (NICUs), maternal infections in medical settings continue to be a leading source of overestimated mortality and morbidity worldwide. 2
Neonatal sepsis (NS) accounts for 15% of neonate deaths worldwide, with 30% to 50% of cases occurring in low and middle-income countries (LMIC).3-6 About 6.9 million neonates are reported to have a possible serious sepsis every year in sub-Saharan Africa, south Asia, and Latin America.3,7 Around 5.94 million children under the age of 5 experienced sepsis in 2015; of these, 45% died, 8 from neonatal sepsis, the third leading cause of newborn death.7,9 Again, 2.6 million infants lost their lives in 2016 to mostly avoidable causes; over 2 million of these deaths happened in the first week of life, and 1 million happened on the day of birth in Africa. 10
Neonatal sepsis is a major newborn killer in Ethiopia and accounts for more than one-third of neonatal deaths. It causes 37% of neonatal deaths, with an incidence rate as high as 10 per 1000 live births.11,12 A recent population-based studies in a rural part of Ethiopia showed that sepsis is the first consequence of neonatal death. 13 According to the 2019 Mini Ethiopian Demographic Health Survey (EDHS) report, the neonatal mortality rate (NMR) in Ethiopia is 30/1000 live births, and this significant number of deaths is greatly attributed to neonatal sepsis. 14
Various factors contribute to this elevated mortality, including under-recognition of illness, delay in healthcare seeking at the household level, delay in initiation of treatment, and lack of access to both properly trained health workers and high-quality services to manage sepsis.15,16 Thus, identifying determinant factors prevailing in the different geographical contexts has become a crucial issue for optimizing neonatal care. 1 The World Health Organization (WHO) has set global objectives to reduce neonatal and under-five mortality to as low as 12/1000 and 25/1000, respectively, by 2030 in African nations to achieve the Sustainable Development Goals (SDGs). 17 In several developing countries, the identification of determinants for neonatal sepsis and the management of neonates with sepsis are unsatisfactory. 11
Although a large amount of research has been done in Africa and other developing countries on the factors associated with newborn sepsis,5,18,19 very few studies have been done in the Amhara region, particularly in the study area. Therefore, identifying determinant factors of neonatal sepsis will be crucial for reducing neonatal mortality and proposing appropriate interventions. Thus, this study aimed to identify determinants of neonatal sepsis among neonates admitted to the NICU ward in Injibara General Hospital in Awi Zone, Amhara Region, Amhara Regional State, Ethiopia.
Methods
Study Area and Period
The study was conducted in the Injibara General Hospital, Awi Zone, Amhara Region, Ethiopia, from March 16, 2020, to April 16, 2020, and a case-control study design was employed. The Injibara General Hospital is located in Injibara, in the town of Awi Administrative Zone. Injibara town is also located in both the Northwestern area of Ethiopia and the Southwest part of the Amhara region. The town is about 447 km away from Addis Ababa, the capital city of Ethiopia, and 118 km from Bahir Dar, the capital city of the Amhara Regional State. It is located at 10°57′N, 36°56′E, at an elevation of 2560 m above sea level. Injibara is situated in a predominantly mountainous location. 20 The hospital was established in February 2015 by the government and provides services in emergency, outpatient, inpatient, and operation room theater departments. The Injibara General Hospital serves more than 1.32 million people in the Awi Zone community. On average, 6 neonates were admitted to the NICU per day, and there were 4 physicians, 12 nurses, and 15 beds in the NICU.
Population
Source population
All neonates who were admitted to Injibara General Hospital were the source population.
Study population
The study population was all neonates admitted to the NICU wards of Injibara General Hospital during the study period.
The cases were all neonates admitted to Injibara General Hospital with their mothers, and peripheral vein blood culture was obtained from them within the first 28 days of life and validated the clinical suspicion of sepsis. 21
The controls in this study were neonates admitted to the NICU of Injibara General Hospital in the Awi zone of Amhara, Ethiopia, during the study period, but without sepsis. Neonates without mothers, with incomplete charts, and who weren’t given a sepsis diagnosis weren’t included in the case. Similarly, newborns admitted without their mothers and those with inadequate charts were not included in the study’s control group.
Sample size determination
The sample size for the study was determined using a double population proportion exposure difference formula by using major determinant variables. 22

Based on the above calculation, the place of delivery had the largest size, 163, which determined the final sample size
Sample Size Calculation to Identify Determinants of Neonatal Sepsis Among Neonates Admitted in a Neonatal Intensive Care Unit IGH, Awi Zone Amhara Regional State, Ethiopia, 2020.

By considering 10% non-response the final sample size was 180. Then the estimated sample size for cases and controls was 60 and 120 respectively, using 1:2 ratios.
Sampling Procedure
Using the log books as the sample frame and a physician’s diagnosis as the basis for selection, a simple random sampling was employed to choose research participants. Through record review, cases and controls were identified following diagnosis by NICU physicians. Cases were chosen from among newborns hospitalized in Injibara General Hospital’s NICUs sequentially. Similarly, the next 2 corresponding controls were selected among newborns hospitalized at Injibara General Hospital’s NICUs on the same day.
Data Collection and Data Quality Control
Neonatal sepsis was a dependent variable, and socio-demographic variables, maternal/obstetric variables, and neonatal variables were independent variables. Neonatal sepsis diagnosed as septic was considered a case, 21 and neonates diagnosed with other problems except sepsis were controlled. A prolonged rupture of the membrane is characterized as a labor that lasts more than 18 hours after the membrane ruptures. 23 Neonates were babies with 28 days of life, and babies weighing less than 2.5 kg were deemed to have low birth weights. 24 Those mothers who could not read and write the Amharic language were considered unable to read and write. Those who live in areas accessed by infrastructure and connectivity health facilities were considered urban residents. In contrast, those who live in rural areas usually don’t have access to infrastructure and connectivity.
The quality of the data was assured with 5 trained data collectors and 2 supervisors. The data were collected through face-to-face interviews by BSc nurses after 2-day data collection training was given to them together with 2 MSc holder supervisors. The questionnaire was structured and pre-tested; it was first prepared in English, translated to the local (Amharic) language, and then again translated back to English. A pretest was conducted on 12 respondents of the sample size in Debre Markos Specialized Hospital, and the necessary corrections were made when necessary, but the results of the pretest were not included in the final analysis.
Data Processing and Analysis
Data were entered, cleaned, and coded using Epi Data version 3.1 and exported to STATA software version 14 for analysis.25,26 Descriptive statistics are presented as frequency and percentages. A Pearson Chi-square test was used to assess the relationship between each independent variable and the outcome variable (neonatal sepsis). Then variables in the bivariate model with a P-value ≤ .25 were entered and analyzed by a multivariable logistic regression model to identify the independent effects of different factors on the occurrence of sepsis. Then, the 95% confidence interval of the adjusted odds ratio (AOR) was computed, and a variable having a P-value less than .05 in the multivariable logistic regression analysis was considered statistically significant.
Ethical approval and informed consent
Ethical clearance for the study was obtained from the Institutional Research Ethics Review Committee of the Debre Markos University (HSC/R/C/Ser/PG/Co/418/11/12). Written and verbal informed consent was obtained from participants’ mothers to confirm their willingness. Participants were interviewed in a separate room, and anonymity and confidentiality of the data providers were strictly maintained.
Results
Socio-Demographic Characteristics of the Respondents
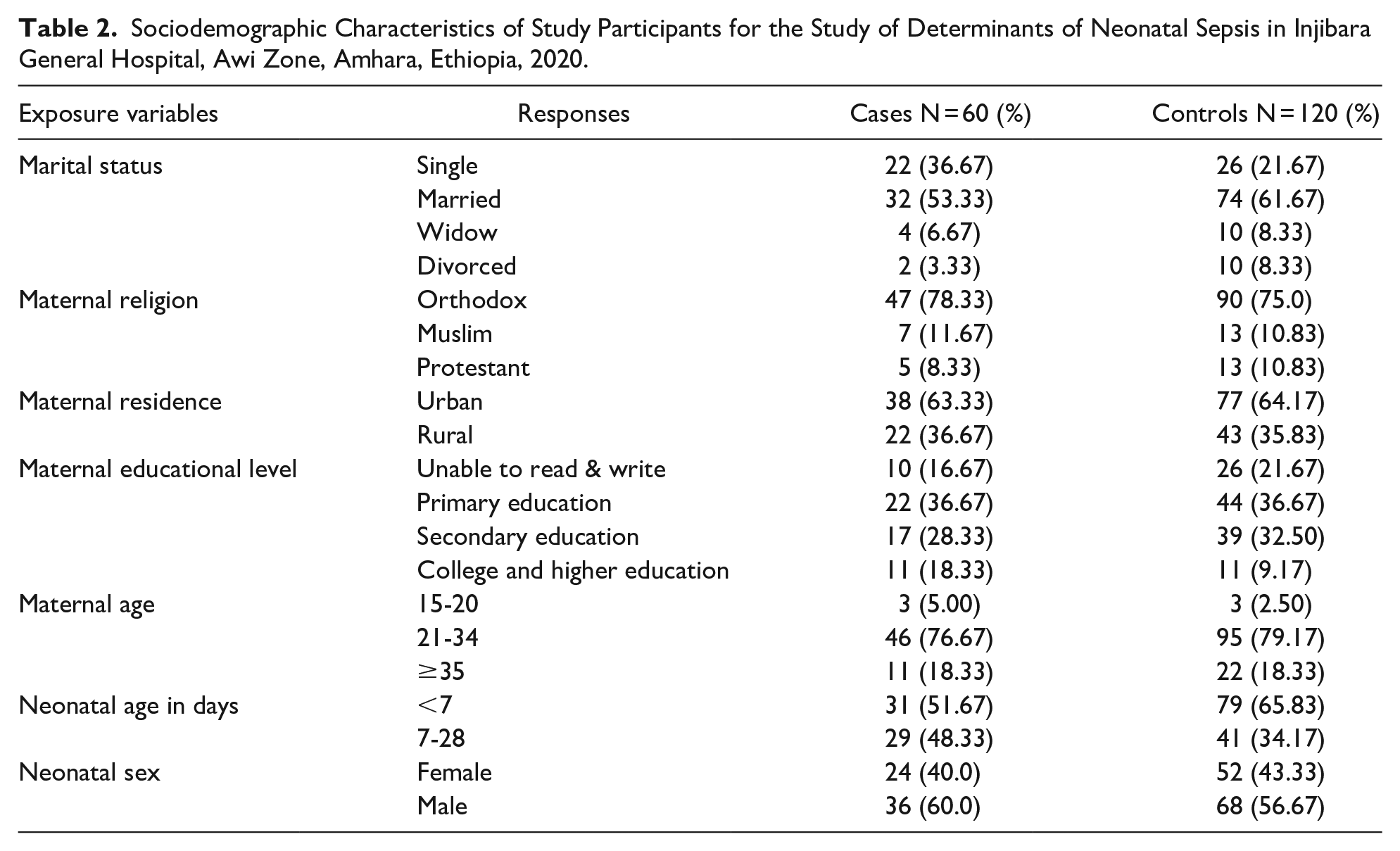
A total of 60 cases and 120 controls admitted to the NICU with their indexed mothers took part in the study. The neonates that were included in the study had ages ranging from 1 up to the 28th day of life, with a mean age of 7.31 (SD ± 5.91) days. Their moms ranged in age from 15 to 45, with a mean age of 28.74 (SD ± 5.48) years. Over half of the participants (60.0%) were male and 56.67% were female, with the majority coming from urban areas (63.33% cases and 64.17% controls). Of the participants, 78.33% of the cases and 75.83% of the control moms identified as Orthodox Christians. Most cases (71.67%) and controls (65.0%) had married couples (Table 2).
Sociodemographic Characteristics of Study Participants for the Study of Determinants of Neonatal Sepsis in Injibara General Hospital, Awi Zone, Amhara, Ethiopia, 2020.
Maternal obstetrics and gynecologic characteristics
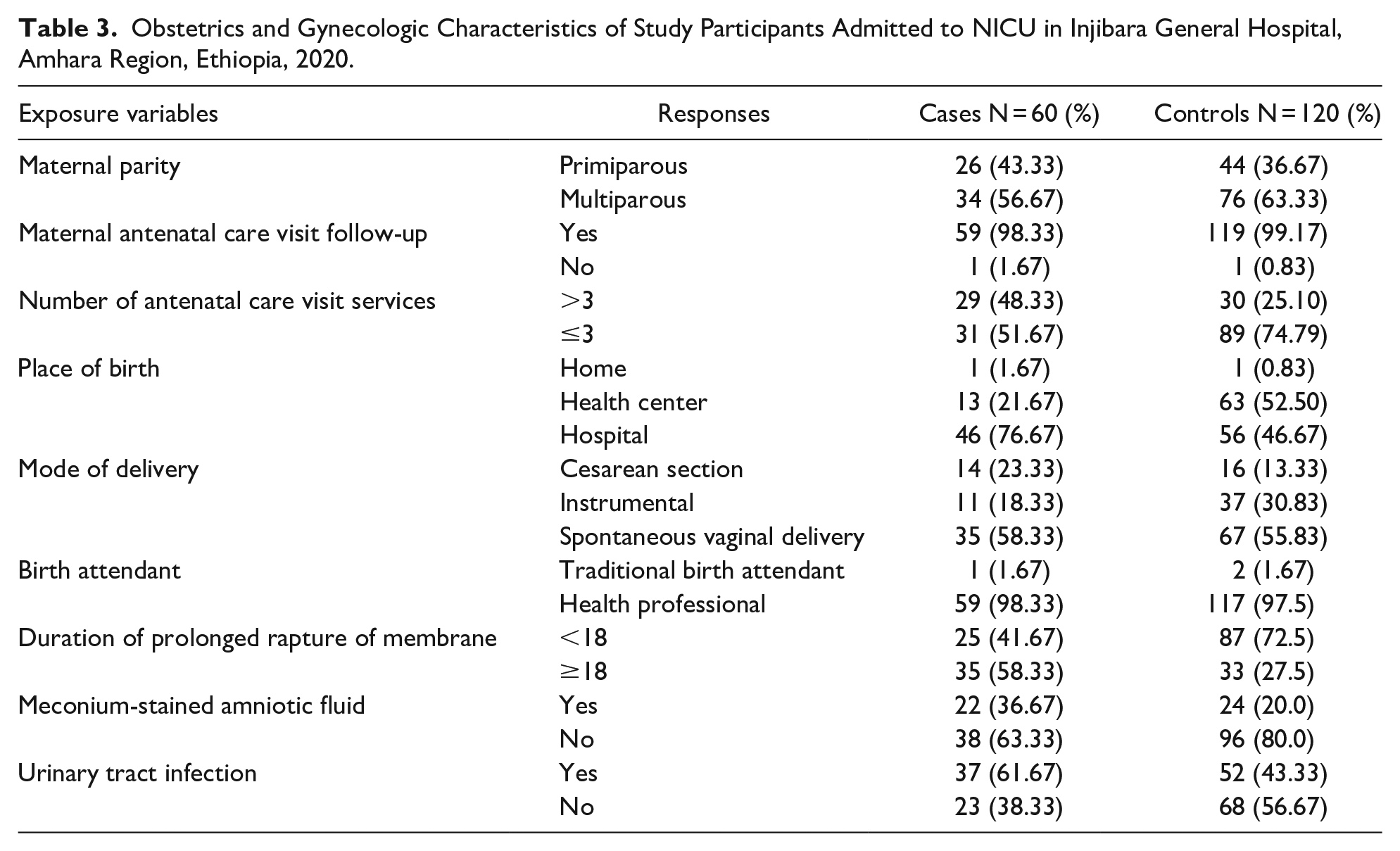
According to this study, the majority of cases (98.33%) and control women (99.17%) received antenatal care (ANC) services while they were pregnant with the present neonate. The proportion of women who attended ANC service ≤ 3 times was higher in controls (68.07%) than cases (51.67%) respectively. More than half of the women (46 (76.67%) of cases and 56 (46.67%) of controls) had given birth at the hospital (Table 3).
Obstetrics and Gynecologic Characteristics of Study Participants Admitted to NICU in Injibara General Hospital, Amhara Region, Ethiopia, 2020.
Neonatal characteristics
This study showed that, nearly two
Neonatal Characteristics of Study Participants Admitted to NICU in Injibara General Hospital, Amhara Region, Ethiopia, 2020.

Determinants of Neonatal Sepsis
After controlling the effect of other variables with binary logistic regression, the number of antenatal care visits, place of birth, mode of delivery, birth weight, duration of the premature rupture of the membrane, urinary tract infection, first-minute apgar score, fifth-minute apgar score, meconium aspiration syndrome, intra-natal fever, immediate cry at birth, resuscitation at birth, oxygen requirement, neonatal age, and gestational age continued to be significantly associated with neonatal sepsis. Finally, after controlling the effect of other variables with multivariable logistic regression analysis, premature rupture of membrane (AOR = 4.42; [2.02, 9.66]), number of maternal ANC visits (OR = 4.49; [1.70-11.86]), AGAR score < 7 (AOR = 3.09 [1.10, 8.70]), place of delivery (AOR = 0.22; [0.08, 0.60]), instrumental delivery [AOR = 0.30; [0.10, 0.88]), and birth weight (AOR = 4.05 [1.44, 11.36]) were the significant factors for neonatal sepsis (Table 5).
Bivariate and Multivariable Logistic Regression Analysis Result for Determinants of Neonatal Sepsis in Injibara General Hospital, Awi Zone, Amhara, Ethiopia, 2020.
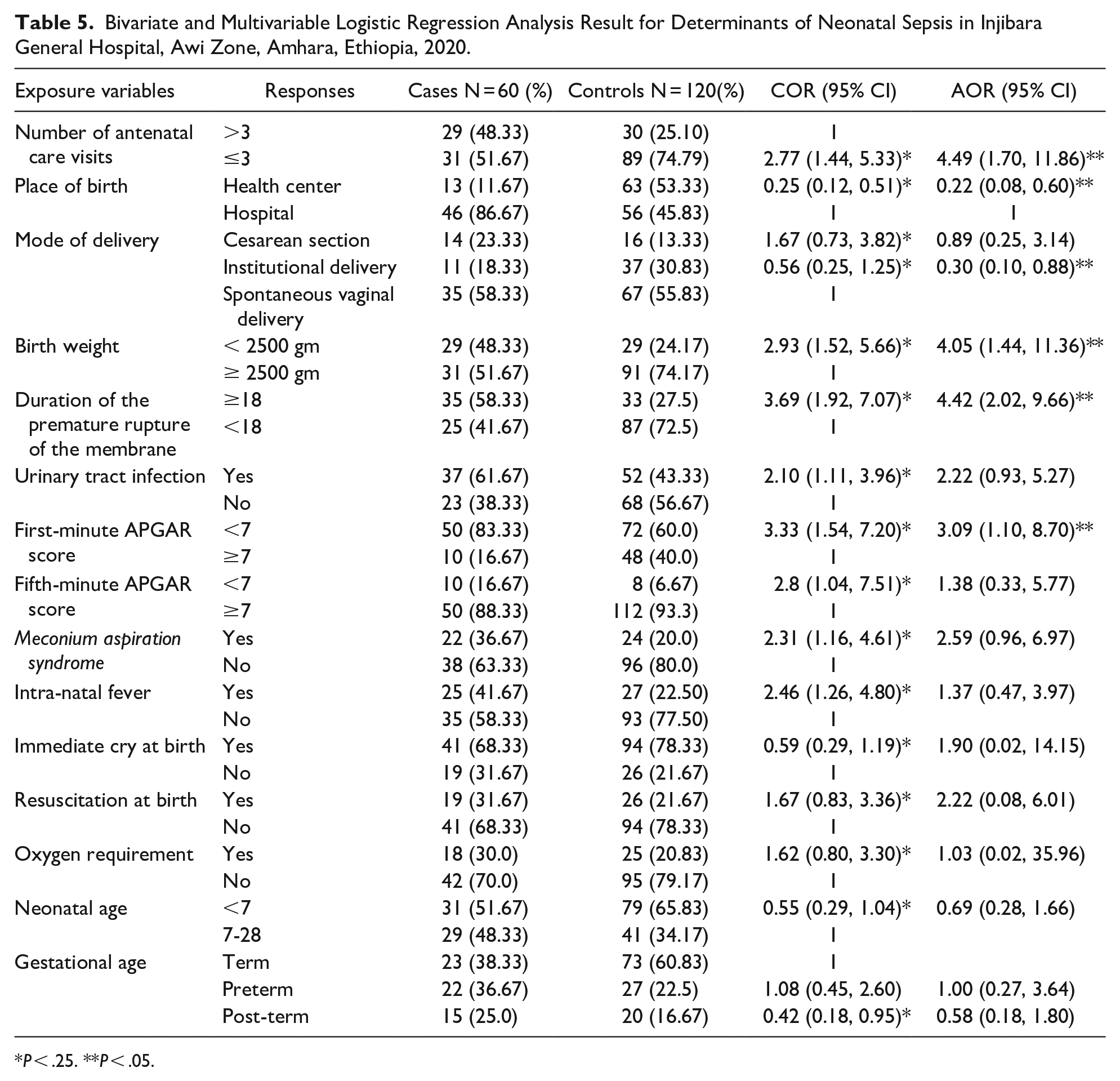
P < .25. **P < .05.
Discussion
This study was done to identify determinants of neonatal sepsis in Injibara General Hospital, Awi Zone, Amhara, Ethiopia. Compared to mothers whose fetal membrane rupture was less than 18 hours, those mothers whose ruptured fetal membrane was more than 18 hours were 4.42 times more likely to give birth to neonates who had sepsis. Studies were carried out in several regions of Ethiopia,22,27-30 Sudan, 18 Mexico, 31 Pakistan, 32 and Nepal 33 which supported the current study result. The possible reason might be the early fetal membrane rupture, which increases the risk of germs from the birth canal rising into the amniotic sac and causing fetal compromise, hypoxia, and chorioamnionitis or placentitis, which frequently result in infection of the fetus in utero. 34
Additionally, the number of ANC visits was found to be significantly associated with the incidence of neonatal sepsis; neonates born to mothers who had ANC visits ≤ 3 times were approximately 5 times more likely to develop sepsis than neonates born to mothers who had ANC visits >3 times. These findings were supported by earlier research conducted in Uganda 35 and India. 36 The possible reason might be that women who had completed ANC services may have had better medical attention and knowledge of risk factors than women who received partial ANC services. Individuals with higher ANC follow-up rates may be eligible for an early danger sign diagnosis.
Similarly, neonates with an APGAR score of less than 7 in the first minute had a threefold increased risk of developing neonatal sepsis in comparison to those with a score of 7 or higher. Studies from Ghana, 34 Indonesia, 37 and Nepal 33 that found a first-minute APGAR score of less than 7 to be a risk factor for newborn sepsis supported the above finding. Resuscitation and an immune insult occur when the Apgar score is low. Neonates exposed to resuscitation techniques after birth asphyxia are at risk for microorganisms that cause sepsis. This could be the consequence of using non-sterile assistance tools, which exposes the neonates to sepsis. Furthermore, sepsis may arise from neonates acquiring the pathogen vertically in utero before delivery.
The risk of neonatal sepsis had a significant association with the place of delivery. Compared to women who gave birth in hospitals, there was a 78% lower chance of neonates with neonatal sepsis in health center-born neonates. Studies carried out in Mekele, Ethiopia, supported the finding. 22 This could be because newborns delivered at health centers may receive treatment there or be sent to other medical facilities for diagnosis or treatment.
Neonates delivered via assisted vaginal delivery had a 70% reduced the risk of developing sepsis compared to those delivered spontaneously. This result was consistent with research from Debrezeit, Ethiopia. 38 The primary reason might be that women who used vacuum delivery techniques correctly were able to lessen the duration of labor, which can decrease hypoxia and ascending infection.
Compared to neonates weighing at least 2500 grams, those weighing less than 2500 grams had a 4-fold increased risk of developing sepsis. Research from Arsi, Jinka, Nigeria, Ghana, and India supported the current result.34,39-42 The possible explanation might be their innate sensitivity to infection and the invasive treatments they undergo. Neonates with low birth weights are more likely to require mechanical ventilation, intravenous access for medicines, parenteral nourishment via cannula, and longer hospital stays. Compared to neonates of average weight, this may put them at a higher risk of sepsis. 43 This may also be because the newborn’s susceptibility to infection is determined by immunological maturity. However, this finding was contrary to the findings of studies conducted in Mekele, 22 Bishoftu, 38 and Bangladesh. 44 The contradiction may be due to socio-economic and health service-related differences.
Conclusion
This study has found that both maternal and neonatal factors contributed to neonatal sepsis. Prolonged rupture of membrane, birth weight, number of ANC visits, place of birth at a health center, instrumental delivery, and first-minute Apgar score were determinants of neonatal sepsis. The government should augment the political priority given to sepsis by improving awareness of the growing medical and economic burden of neonatal sepsis. Health professionals should provide counseling for mothers who don’t have complete ANC services. Primary care organizations should also increase their support for maternal education and include routine neonatal sepsis screening in the care of neonates and mothers.
Footnotes
Acknowledgements
We would like to thank Debre Markos and Injibara Hospital for their permission to do this research and we gratefully acknowledge all study individuals for their participation in the study.
Author Contributions
All authors contributed equally.
Availability of Data and Materials
Data supporting this study can be obtained on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for Publication
All authors have a copy of this manuscript. The authors would like to confirm that this article has not been submitted to any other journal and we fully agree to be published by this journal.