
Abstract
Background. Despite the significant public health impact of neonatal jaundice on neonatal survival, local epidemiologic data are scarce. Methods. A multi-centered, unmatched case-control study was conducted among 180 consecutively admitted neonates (60 cases and 120 controls). The independent determinants of newborn jaundice were determined using a multivariable binary logistic regression model, and a P-value of <0.05 was used to indicate statistical significance. Results. Maternal medical complications during the index pregnancy (AOR = 2.45; 95% CI 1.01-5.97), rural residence (AOR = 3.1; 95% CI 1.02-9.42), being a low birthweight neonate (AOR = 3.42; 95% CI 1.12-10.41), neonatal B blood group (AOR = 10.19; 95% CI 2.89-35.9), neonatal O blood group (AOR = 2.99; 95% CI 1.04-8.59), and a longer duration of hospital stay (AOR = 9.83; 95% CI 3.11-31.02) were the independent determinants of neonatal jaundice. Conclusions. Early assessment of high-risk neonates might reduce the long-term neurodevelopmental consequences.
• The buildup of unconjugated bilirubin levels in the blood is what causes neonatal jaundice.
• There is a dearth of representative local studies conducted in the Tigray region of northern Ethiopia that identify the independent determinants of neonatal jaundice.
• The epidemiologic distributions of neonatal jaundice are well documented in those developed countries.
• In neonates admitted to neonatal intensive care units, this study will determine the factors that contribute to neonatal jaundice.
• This study will assist medical professionals in overcoming the difficulties associated with the early diagnosis and treatment of newborn jaundice in a resource-poor setting.
Introduction
Neonatal jaundice is one of the most common clinical signs that indicate hyperbilirubinemia. Jaundice becomes evident when the total serum bilirubin level reaches 5 mg/dL (86 mmol/L). 1 The buildup of unconjugated bilirubin levels in the blood is what causes neonatal jaundice. Yellowish discoloration of the skin, eyes, palms, and soles of feet, dark urine, and pale faces are the clinical features of neonatal jaundice. 2 Neonatal jaundice is linked to both fatal and nonfatal health outcomes, as well as possible long-term effects (neurological impairment), including death. 3
Globally, neonatal jaundice affects 60% to 80% of newborn babies and is one of the leading causes of hospitalization in the first week of life. 3 In the early (0-6 days) and late (7-27 days) neonatal periods, deaths attributed to neonatal jaundice account for 1309.3 per 100 000 live births and 187.1 per 100 000 live births, respectively. 4 Jaundice, which occurs within the first 36 hours and lasts more than 2 weeks, accounts for 82.8% and 95.27%, respectively. 5 Neonatal sepsis (66.7%), prematurity (15.2%), lack of breastfeeding (9%), and ABO incompatibility (5.2%) were the leading causes of neonatal jaundice. 6
In Africa, the incidence of severe neonatal jaundice accounts for 667.8 per 100 000 live births, which is higher than the incidence in Southeast Asia, the Eastern Mediterranean, the Western Pacific, America, and the European regions. In sub-Saharan Africa, neonatal jaundice accounts for 1309 deaths per 100 000 live births, making it the eighth leading cause of death. 3 Neonatal mortality in Ethiopia accounts for 30 deaths per 100 000 live births, 7 in Mekelle, the capital city of the Tigray region, the magnitude of neonatal jaundice was 37.3%. 8 Late presentation to health facilities was common, which resulted in high rates of acute bilirubin encephalopathy and avoidable exchange transfusions. 9
Severe neonatal hyperbilirubinemia causes neonatal mortality and chronic bilirubin neurotoxicity that manifests as cerebral palsy (kernicterus) or auditory problems with and without hearing deficits. 4 Early identification of the determinants of neonatal jaundice could facilitate the timely care-seeking process and improve treatment outcomes. 10
Previous local studies assessed the magnitude and factors associated with neonatal jaundice. To the best of our knowledge, we did not get local representative studies conducted in the whole Tigray region of northern Ethiopia that determined the independent determinants of neonatal jaundice. Hence, the objective of this study was to identify the determinants of neonatal jaundice among neonates admitted to the neonatal intensive care units of Tigray Region General Hospitals, Northern Ethiopia, in 2020.
Methods and Materials
Study Area and Period
The study was conducted at the Neonatal Intensive Care Units (NICU) of Tigray Region public general hospitals, in northern Ethiopia. In the Tigray region, there are 15 public general hospitals; from these, 5 hospitals were randomly selected: Lemlem Karl general hospital, Suhul general hospital, Mekelle general hospital, Adigrat general hospital, and St. Mary general hospital. The NICU is a specialized treatment center for neonates in need of intensive care, like those diagnosed with neonatal sepsis, birth asphyxia, neonatal jaundice, prematurity, and congenital anomalies. The study was conducted from February 1 to April 30, 2020.
Study Design
A multi-centered, unmatched case-control study was conducted among consecutively admitted neonates in the NICU of selected public general hospitals in the Tigray region.
Eligibility Criteria
Cases were newborn babies less than 28 days old with clinically evident manifestations of neonatal jaundice as clinically confirmed by the physician (pediatrician, general practitioner, neonatal nurse) with their index mothers were included in this study.
Controls were newborn babies less than 28 days old admitted to the NICU at least 6 hours after birth, who had no clinical evidence of neonatal jaundice and were admitted for other medical conditions as confirmed by the physician (pediatrician, general practitioner, neonatal nurse), and their index mothers were included in this study. Whereas, neonates with or without jaundice who had no mother, which could be due to death or any other reason, and neonates with major congenital malformations were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was determined using the double population proportion formula using Epi Info version 7.2.2.6 software, taking the sepsis status of the neonates as the main exposure variable, and with the assumptions of a 2-sided significance level (α = 5%), power (1−β) = 80%, a 95% confidence level, and a ratio of controls to cases (R) of 2:1. Accordingly, the sample size was calculated with the assumption that the percent of controls exposed = 51%, 8 to detect an odds ratio of 2.64, and an adjustment was made by taking a 10% non-response rate.
The final sample size required to get a statistically meaningful difference between cases and controls was 180 (60 cases and 120 controls). A consecutive sampling technique was used to select the number of cases and controls after the proportional allocation of the sample size to each selected general hospital by taking the last quarter’s report of the number of jaundice cases in the selected hospitals. For each selected case, 2 consecutively admitted controls were taken.
Operational Definitions
Neonatal sepsis is a systemic bacterial, viral, or fungal (yeast) infection of the baby from birth to 28 days. 11 Hypoglycemia was defined as a low blood glucose level, which is less than 40 mg/dL, 12 and hypothermia was defined as an axillary temperature of less than 36.5°C. 13 The average duration of labor for primiparous and multiparous mothers was defined as less than 24 and 12 hours, respectively. The prolonged duration of labor for primiparous and multiparous mothers was defined as above 24 and 12 hours, respectively. 14
Obstetric complications during the index pregnancy are any of the complications that occurred during the index pregnancy, like preeclampsia or eclampsia, intrauterine growth restriction, gestational diabetes mellitus, and hyperemesis gravidarum. 14
ABO incompatibility was defined as a neonate with blood group A or B born from O blood group mothers. 15 Rhesus (Rh) incompatibility was defined as a clinical condition that occurred when an Rh-negative mother gave birth to an Rh-positive baby. 15 Physiological jaundice was defined as jaundice attributable to the physiological immaturity of neonates to handle increased bilirubin production, usually appearing between 24 and 72 hours of age. 16 Pathologic jaundice was defined as visible jaundice that usually appears within 24 hours of age or >14 days of age. 16
Study Variables
The primary outcome measurement was the neonatal jaundice status of the neonates classified as neonates with and without neonatal jaundice.
Independent Variables
Socio-demographic characteristics of the mother include age, religion, residence, marital status, occupational status, educational status, and average monthly income.
Neonatal characteristics: age, gender, gestational age at delivery, birthweight, blood group, and Rh factor. Neonatal complications like birth asphyxia, neonatal sepsis, cephalohematomas, meconium or amniotic fluid aspiration, hypoglycemia, and hypothermia.
Obstetric characteristics: antenatal care visit, place of antenatal care visit, detection of obstetric complications during the index pregnancy, gravidity, parity, previous induced abortion, mode of delivery, duration of labor, the timing of delivery, maternal blood group, Rh factor, ABO incompatibility, and Rh incompatibility.
Data Collection Tool and Procedure
The data were gathered using an interviewer-administered, pre-tested, structured questionnaire. The questionnaire was derived from many literary works8,13,14,19,20 and comprises significant factors that were arranged following the study’s goal. The interviewer-administered questionnaire was written in English, translated into the local language (Tigrigna), and then retranslated back into English to ensure uniformity. Additional information on the clinical status of cases and controls with their index mothers was retrieved by reviewing their medical records using a structured data abstraction checklist.
Following the delivery of the appropriate care to the neonates, the index mothers of the neonates were interviewed at the NICU of the chosen hospitals. Five nurses with bachelor’s degrees worked as data collectors under the supervision of 5 master’s-trained nurses who worked in the NICUs of the hospitals. Two days before the data collection period, the primary investigator trained the data collectors on the questionnaire’s contents and how to interact with respondents. The questionnaire has 3 parts: socio-demographic characteristics of the mother, neonatal characteristics, and obstetric characteristics (See Supplemental File).
Data Processing and Analysis
The collected data were coded and checked for their clarity, consistency, and completeness up to the end of each data collection period, and Epi-Data version 4.4.2.1 software was used for data entry. The entered data were exported to SPSS version 25.0 for Windows. Descriptive statistics of skewed numeric variables were presented with medians and interquartile range (IQR) and categorical variables were presented using frequency and percentages.
The bivariate analysis was done to check the existence of crude association and to select candidate variables, those variables which are clinically important and have (P < .25) were included in the final model. Confounding was checked and a percentage change in the regression coefficients (β) less than 20% reveals an absence of confounder. Interaction for the main effect model was also checked and partial likelihood ratio test result with P-value > .05 and variance inflation factor less than 10 indicated the non-existence of multi-collinearity among the independent variables.
The multivariable binary logistic regression model was used to identify the independent determinants of neonatal jaundice. The summary measures of estimated crude (COR) and adjusted odds ratios (AOR) with a 95% confidence interval were presented and a P-value less than .05 was used to declare statistical significance and the goodness of fit of the model was assessed by using Hosmer and Lemeshow goodness of fit test.
Ethics Approval and Informed Consent
The Health Research Ethics Review Committee of the College of Health Sciences, Mekelle University granted ethical approval with reference number (ERC 1551/2020). Each mother provided written, informed consent, and all information gathered from them was treated with strict confidentiality. Neither the case files nor the data were used for any other reason. The study was carried out following the 1964 Declaration of Helsinki, and all patient data were held anonymously.
Results
Sociodemographic Details of Mothers
This study included 180 neonates in all, giving a response rate of 100%. Of these, 60 infants had neonatal jaundice with their index mothers, and 120 neonates did not. The overall median (IQR) age of the mothers was 27 (23-30) years, among mothers who had neonates with and without neonatal jaundice it was 26 (22-29), and 27 (23.5-30) years, respectively. Thirty-eight (63.3%) mothers had neonates with jaundice and 99 (82.5%) mothers with neonates without jaundice lived in urban areas. Concerning the educational status of the mothers, 10 (16.7%) and 12 (10%) mothers who had neonates with and without neonatal jaundice were unable to read and write respectively. Concerning the marital and occupational status of the mothers, 168 (93.4%) of them were married and 43 (23.9%) of the mothers were government employees (Table 1).
Socio-demographic Characteristics of Mothers Whose Neonates Were Admitted to the Neonatal Intensive Care Units of Tigray Region Public General Hospitals, Northern Ethiopia, 2020 (n = 180).

Abbreviations: IQR, interquartile range.
Implies that mothers were not comparable based on their place of residence and occupational status using the Pearson Chi-square test.
Neonatal Characteristics
The overall median (IQR) age in days of the neonates at admission was 1 (1-2) days, similarly, among neonates with and without jaundice, their median (IQR) age in days at admission was 1 (1-4) and 1 (1-1.5) days, respectively. The median (IQR) gestational age at birth in weeks for all newborns was 39 (37-40) weeks, and for neonates with and without jaundice, it was 38 (36.5-40) and 39 (38-40) weeks, respectively. Concerning the gender of the neonate, 42 (70%) neonates with jaundice and 66 (55%) neonates without jaundice were male babies. Twenty-six (43.3%) neonates with jaundice and 22 (18.3%) neonates without jaundice were low birthweight neonates (Table 2). Nine (15%) neonates with neonatal jaundice and 6 (5%) neonates without neonatal jaundice developed birth asphyxia, similarly, 11 (18.3%) neonates with neonatal jaundice and 10 (8.3%) without neonatal jaundice developed neonatal sepsis (Figure 1).
Neonatal Characteristics of Neonates Admitted to the Neonatal Intensive Care Units of Tigray Region Public General Hospitals, Northern Ethiopia, 2020 (n = 180).
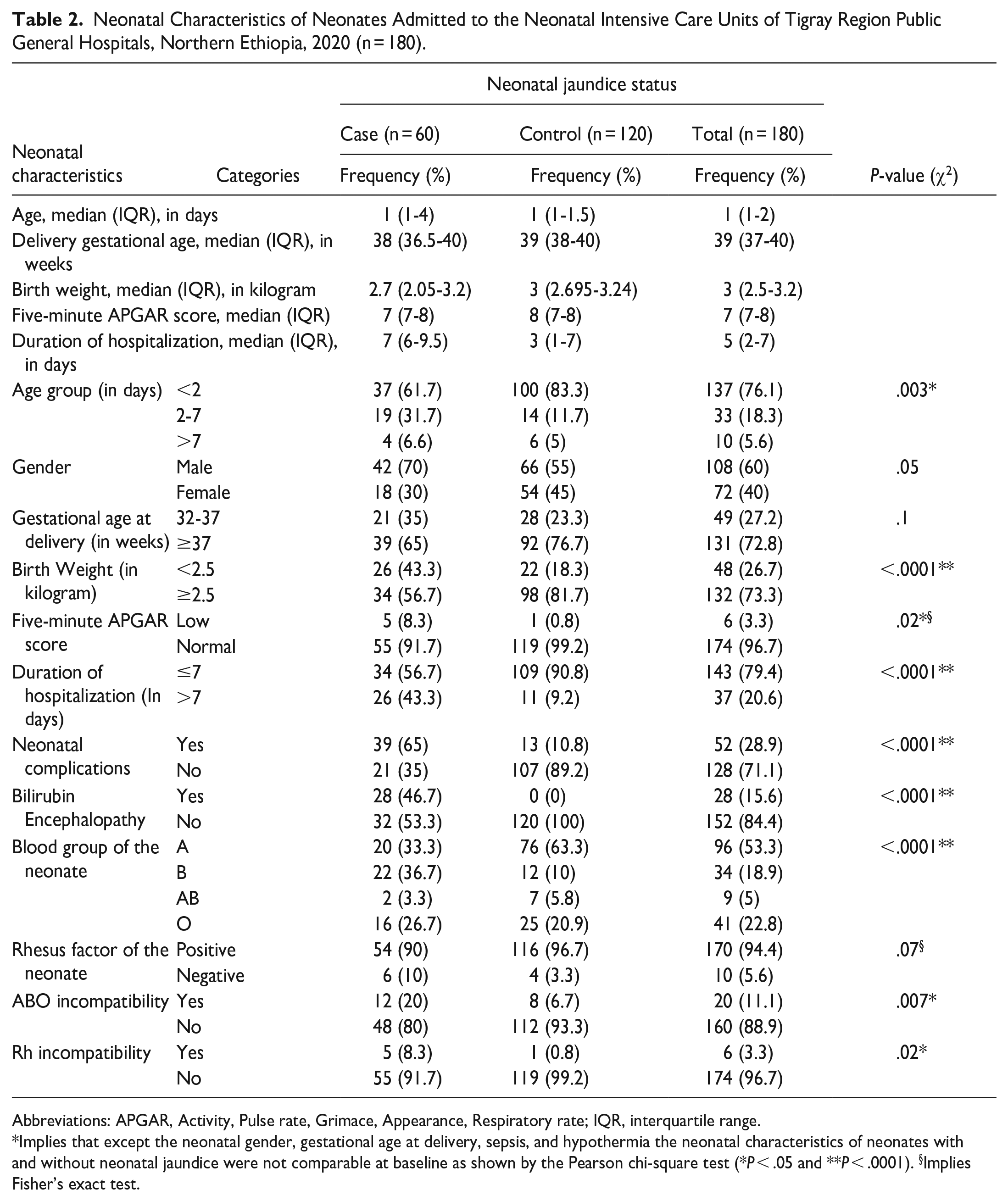
Abbreviations: APGAR, Activity, Pulse rate, Grimace, Appearance, Respiratory rate; IQR, interquartile range.
Implies that except the neonatal gender, gestational age at delivery, sepsis, and hypothermia the neonatal characteristics of neonates with and without neonatal jaundice were not comparable at baseline as shown by the Pearson chi-square test (*P < .05 and **P < .0001). §Implies Fisher’s exact test.
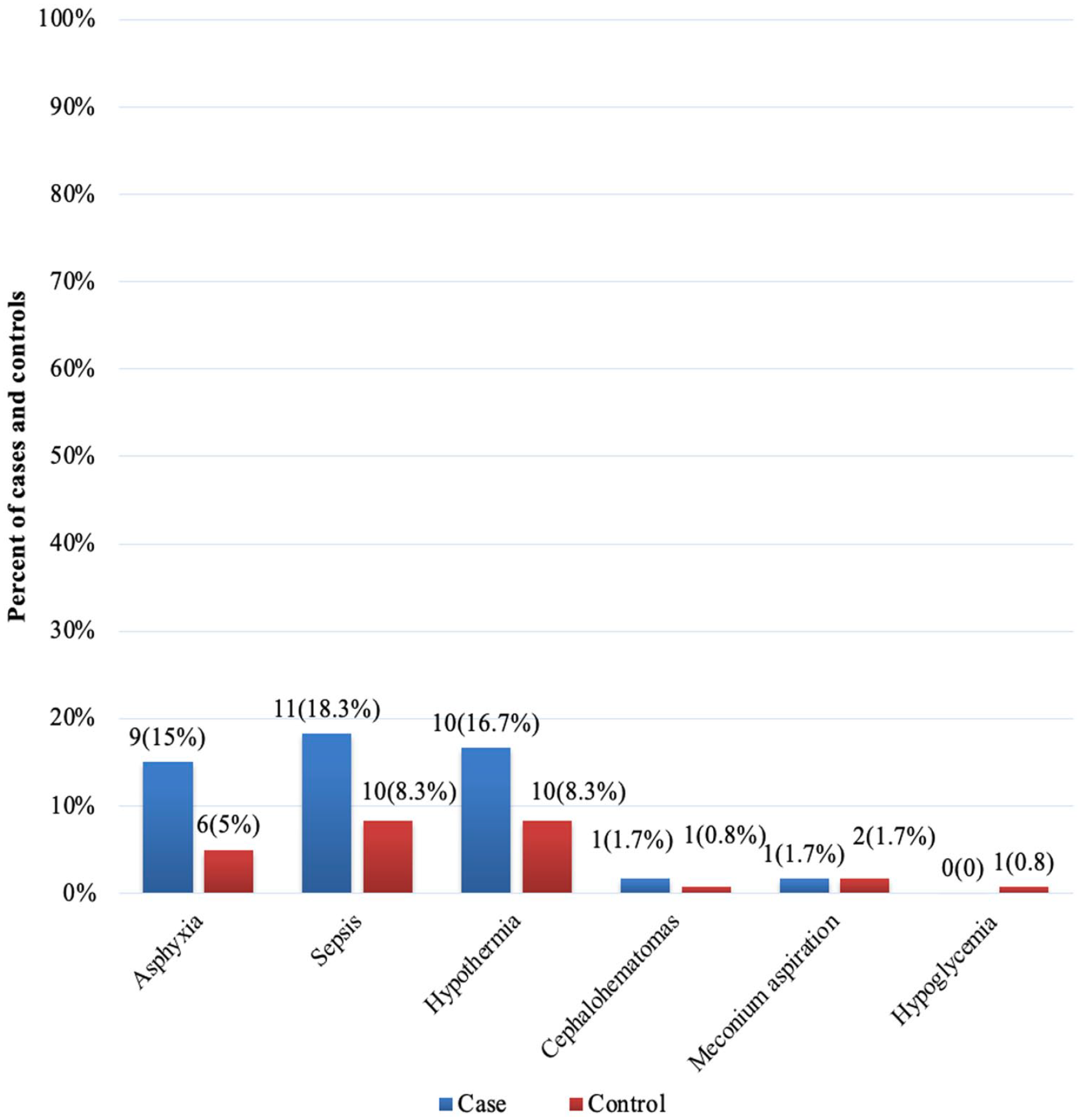
Common neonatal complications among neonates admitted to the neonatal intensive care units of Tigray region public general hospitals, Northern Ethiopia, 2020 (n = 180).
Maternal Characteristics
One hundred seventy-seven (98.3%) mothers had antenatal care visits during their index pregnancy, 59 (98.3%) and 118 (98.3%) mothers whose neonates diagnosed with and without jaundice had antenatal care visits during their index pregnancy, respectively. Eighty-nine (49.4%) mothers had developed at least one obstetric complication during their index pregnancy, similarly, among mothers whose neonates were diagnosed with jaundice 34 (56.7%) of them developed obstetric complication during their index pregnancy. Concerning the reproductive history of the mothers, 26 (43.3%) and 48 (40%) mothers who had neonates diagnosed with and without neonatal jaundice were primigravidas, respectively (Table 3).
Obstetric Characteristics of Last Pregnancy Among Mothers Whose Neonates Were Admitted to the Neonatal Intensive Care Units of Tigray Region Public General Hospitals, Northern Ethiopia, 2020 (n = 180).

Abbreviations: BMI, Body Mass Index; IQR, interquartile range.
Implies Fisher’s exact test.
Determinants of Neonatal Jaundice
The multi-variable logistic regression model shows that after adjusting for the impact of additional covariates, mothers who had at least one obstetric complication during their index pregnancy were twice as likely to possess a neonate with neonatal jaundice than their counterparts who had no medical complications during their index pregnancy (AOR = 2.45; 95% CI 1.01-5.97). Similarly, low birthweight neonates were 3 times more likely to have neonatal jaundice than their counterparts who had normal birthweight (AOR = 3.42; 95% CI 1.12-10.41).
The odds of having neonatal jaundice diagnosed neonate among mothers residing in rural areas were 3 times more likely than their counterparts residing in urban areas (AOR = 3.1; 95% CI 1.02-9.42), similarly, the odds of developing neonatal jaundice among neonates who had B blood group was 10 times more likely than their counterparts who had A blood group (AOR = 10.19; 95% CI 2.89-35.9).
The odds of having neonatal jaundice among neonates who had the O blood group was 3 times higher than neonates who had the A blood group (AOR = 2.99; 95% CI 1.04-8.59), similarly, the odds of developing neonatal jaundice among neonates admitted for more than 7 days in the hospital, was almost 10 times higher than their counterparts who stayed in the hospital of not more than 1 week (AOR = 9.83; 95% CI 3.11-31.02) (Table 4).
Determinants of Neonatal Jaundice Among Neonates Admitted to the Neonatal Intensive Care Units of Tigray Region Public General Hospitals, Northern Ethiopia, 2020 (n = 180).

Abbreviations: AOR, adjusted odds ratio; APGAR: Activity, Pulse rate, Grimace, Appearance, Respiratory rate; BMI, Body Mass Index; CI, confidence interval; COR, crude odds ratio.
Shows a significant difference at P < .05, and ** shows a significant difference at **P < .0001. ꜧ implies P-value of Hosmer and Lemeshow goodness of fit test for assessing the goodness of fit test after fitting logistic regression, accordingly, our model fits with the data we have.
Discussions
Among newborns admitted to the neonatal intensive care units of the public general hospitals in the Tigray region of Northern Ethiopia, this region-based case-control study attempted to identify the factors that contribute to neonatal jaundice. The odds of neonatal jaundice were 3 times more likely among low birthweight neonates than neonates with normal birthweight. This finding was in line with the study conducted in Japan, 17 Ghana, 18 and India.14,19 Similarly, this finding was consistent with the studies conducted in Amhara 13 and Tigray regions. 20 This could be caused by a newborn having low birthweight and premature organs, particularly the liver, as well as failing to conjugate bilirubin created by the destruction of red blood cells. 13
Low birthweight infants may also feed less and have fewer bowel movements, which results in less bilirubin being removed through the stools and an increase in bilirubin circulation in the liver. 21 As a result, supplementation should be used in clinical settings for newborns who are at risk of having insufficient calorific intake. 22 According to this, low birthweight infants should be evaluated for their feeding status and require particular treatment to detect neonatal jaundice early.
Compared to neonates whose mothers resided in urban areas, neonates whose mothers resided in rural areas had a twofold increased risk of developing newborn jaundice, this finding was comparable with the study done in Egypt. 23 This can be explained by, women who lived in cities having much greater knowledge of the risk factors, complications, and management for neonatal jaundice than mothers who lived in rural areas. This could also be explained by the result of limited access to the healthcare institution that can treat newborns with jaundice-related issues beginning during pregnancy and continuing into the early postnatal period. Health services are widely accessible in metropolitan areas but may be challenging to access in rural areas due to the distance between health institutions and residents’ homes in Ethiopia. 24
Strengths and Limitations of the Study
It is the local multi-center study; bilirubin values were not collected because they were not regularly assessed or documented in medical records. Due to the lack of laboratory results on bilirubin level in the study area, physician-documented evidence was used. So different physicians may have different experiences and there could be misclassification bias. There was a lack of some information in the medical records of both neonates and mothers (eg, hematology results of mothers and neonates were not registered in their medical records). The findings of this study have an implication; regular collection of the serum bilirubin level and proper documentation of the client’s medical data should be given priority.
Conclusions
Maternal medical complications during the index pregnancy, being a low birthweight neonate, maternal rural residence, having a B blood group of the neonate, having an O blood group of the neonate, and longer duration of hospital stay were the independent determinants of neonatal jaundice. Early assessment of neonates with a higher chance of developing jaundice after delivery might reduce the long-term neuro-developmental consequences.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X231190518 – Supplemental material for Neonatal Jaundice: Its Determinants Among Neonates Admitted to Neonatal Intensive Care Units of Tigray Region General Hospitals, Northern Ethiopia
Supplemental material, sj-docx-1-gph-10.1177_2333794X231190518 for Neonatal Jaundice: Its Determinants Among Neonates Admitted to Neonatal Intensive Care Units of Tigray Region General Hospitals, Northern Ethiopia by Berhe Mengesha Kiros, Girmatsion Fisseha, Assefa Ayalew Gebreslassie, Zenawi Hagos Gufue, Haftamu Ebuy, Molla Teferi Belew, Getachew Zinabu Reda and Hayat Maeruf Mohammed in Global Pediatric Health
Footnotes
Acknowledgements
The study’s authors express gratitude to all the mothers who took the time to participate.
Author Contributions
Conceptualization: BMK; Data curation: BMK, GF, and AAG; Formal analysis: BMK, HMM, and ZHG; Investigation: BMK, GF, MTB, and AAG; Methods: BMK, HE, and GZR; Software: ZHG, and GZR; Supervision: BMK, and ZHG; Writing—original draft: BMK, ZHG, and GZR; Writing—review & editing: BMK, GF, AAG, ZHG, GZR, HE, MTB, and HMM.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
The Health Research Ethics Review Committee of the College of Health Sciences, Mekelle University granted ethical approval with reference number (ERC 1551/2020). Each mother provided written, informed consent, and all information gathered from them was treated with strict confidentiality. Neither the case files nor the data were used for any other reason. The study was carried out following the 1964 Declaration of Helsinki, and all patient data were held anonymously.
Patient and Public Involvement
In the planning, execution, reporting, or distribution of this study, patients and/or the general public were not included.
Consent for Publication
Not applicable.
Data Availability Statement
The corresponding author will provide the datasets created and used in the current work upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.