
Abstract
Objective. To reduce neonatal intensive care unit admission rate (NAR) and antibiotic utilization rate (AUR) in ≥36 weeks gestational age infants exposed to maternal chorioamnionitis (MC) through the application of early-onset sepsis calculator (EOSCAL). Study Design. This is a single-center cohort study. All infants born ≥36 weeks gestational age and exposed to MC were compared for NAR, AUR, and laboratory evaluation rate (LER) 2 years after and 1 year before the implementation of EOSCAL. Results. There is a significant decrease in NAR (P < .001), AUR (P < .04), and LER for blood culture, complete blood count, and C-reactive protein (P < .001) after implementation of EOSCAL. If infants received antibiotics, it was for significantly less number of doses (P < .01). There was no increase in the readmission rate. Conclusion. Use of EOSCAL significantly decreases the rate of NAR, AUR, and LER in infants exposed to MC, without affecting readmission rates and late antibiotic use.
Introduction
Early-onset sepsis (EOS), defined as an infection that manifests within 3 or 7 days after birth and proven by a positive culture in blood or cerebrospinal fluid, is a significant cause of neonatal morbidity and mortality. 1 A meta-analysis by Benitz et al reported chorioamnionitis (CAM) in most (88%) cases of EOS despite intrapartum maternal antibiotic therapy. 2 Current recommendations from the American Academy of Pediatrics and Centers for Disease Control and Prevention (CDC) state that all infants exposed to MC including well-appearing infants should undergo a limited diagnostic evaluation and receive empiric antimicrobial therapy. 3 Group B Streptococcus continues to be the most common organism implicated in EOS. 4 Prevention guidelines, as well as obstetrical and neonatal care, have reduced the incidence of both early-onset group B Streptococcus sepsis 5 and overall EOS.4,6 A clinically apparent CAM complicates approximately 2% to 5% of term deliveries. 7 The rate of EOS in term infants exposed to MC is also low at 2 to 4 per 1000 live births,8,9 and as per recent studies, there are fewer instances of failed intrapartum prophylaxis resulting in EOS associated with MC. 10 National Institute of Child Health–sponsored conference proposed management for asymptomatic infants 34 weeks with either maternal fever or suspected intra-amniotic infection to be just observation and evaluation. They also urged the use of alternative approaches like the use of EOSCAL (early-onset sepsis calculator). 11 The EOSCAL estimates a neonate’s probability of EOS and provides the recommendation for management based on several antepartum risk factors for sepsis and the infant’s clinical status after birth.12,13 The EOSCAL is increasingly used by neonatologists to limit laboratory evaluation (LE) and antibiotic use 15 in infants born ≥34weeks of gestational age (GA), but there are limited data to support its use in infants exposed to MC.
We implemented EOSCAL as part of antibiotic stewardship in infant born ≥34weeks of GA. In this article, we have compared the antibiotic utilization rate (AUR), neonatal intensive care unit (NICU) admission rate (NAR), LE rate (LER), and also the length of NICU stay in infants 36 weeks exposed to MC, 1 year before and 2 years after the implementation of EOSCAL.
Materials/Subjects and Methods
This study is a single-center cohort study. The Institutional Review Board at Hennepin County Medical Center approved the study. Data collection was performed by the review of the electronic medical charts of all infants ≥36 weeks GA and exposed to MC born during the study period. The study period was divided into 2 phases. The first phase was before the implementation of EOSCAL from January 2015 to December 2015, when all infants exposed to MC were admitted to NICU for continuous clinical monitoring and periodic LE (Figure 1). Antibiotics were considered only in infants with clinical signs of sepsis and/or if there was abnormal LE. Our NICU joined an Internet collaborative with Vermont Oxford Network “Using Antibiotics Wisely” starting February 2016. There was an increased awareness of antibiotic stewardship, and EOSCAL implementation during the period from January 2016 to March 2016. The data from this washout period were conscientiously excluded from this study. The second phase was after the implementation of EOSCAL from April 2016 to March 2018, where all infants born ≥34 weeks of GA were managed using EOSCAL recommendations. EOSCAL was performed at birth and with the change in clinical status within 24 hours after birth. In addition to recommendations from EOSCAL, additional laboratory tests (complete blood count [CBC] and C-reactive protein [CRP]) were checked with any change in clinical status (Figure 2). Infants who were born at 34 and 35 weeks of GA were routinely admitted to NICU for monitoring and were excluded from this study.

Flow depicting the management of infants before the implementation of EOSCAL.

Flow depicting the management of infants after the implementation of EOSCAL
The primary outcome measure was to determine the difference in the AUR in the first 48 hours after birth, and the NAR in ≥36 weeks GA infants exposed to MC before and after implementation of EOSCAL. NAR was calculated per 100 live-born infants. AUR was calculated as the number of calendar days infant was on antibiotics per 100 live-born infants. Overall AUR (OAUR) was defined as antibiotic use among all NICU admissions and was calculated as the number of calendar days per 100 patient days. Secondary outcome measures were to compare LER, which was defined as the number of laboratory tests such as CBC, CRP, and blood culture performed in the first 48 hours of life per 100 live-born infants, the number of doses of antibiotics received within 48 hours after birth, and readmission rate within 28 days after discharge. The rate of readmission and the use of antibiotics within the first 28 days after discharge from the NICU was tracked by using the electronic medical chart for all the study subjects.
Nominal variables were presented as percentages and continuous data as means and SDs or median and 25th to 75th percentiles, depending on distribution normality. Categorical variables were compared between groups with the χ2 test. Differences in continuous variables were compared by 2-tailed Student’s t tests or Mann-Whitney U test where appropriate.
Ethical Approval and Informed Consent
The Institutional Review Board at Hennepin County Medical Center approved the study with ID HSR#17-4405. Informed consent was waived under the category 45 CFR 46.116.
Results
A total of 5346 infants ≥36 weeks GA were born during the study period, 289 (5.4%) infants were exposed to MC, and the incidence of EOS was 0.35%. Baseline maternal and neonatal characteristics for these 2 periods were comparable (Table 1). Overall, more mothers received antibiotics before EOSCAL (P < .006), but the number of mothers receiving antibiotics >4 hours prior to delivery was similar in both the groups (P = .688) After implementation of EOSCAL, the number of infants receiving antibiotic treatment was significantly reduced including those not needing respiratory support (Table 1). After implementation of EOSCAL, OAUR decreased from 16.4 to 10.9 per 100 patient days (P < .001). Figure 3a shows the trend of OAUR over the study period. AUR among the infants born ≥36 weeks and exposed to MC decreased from 2.2 to 1.1 per 100 live births after the implementation of EOSCAL (P < .04), as shown in Figure 3b. Among the infants who received antibiotics, the median number of antibiotic doses were 4 (interquartile range = 4-8) after EOSCAL implementation as compared with 8 (interquartile range = 5-14) before intervention (P < .01). NAR among the infants exposed to MC decreased from 5.7 to 2.5 per 100 live births after implementation of EOSCAL (P < .001), trends are presented in Figure 4. Overall, 90/111 (81%) of asymptomatic infants stayed with their mother and required no evaluation or antibiotic treatment.
Maternal and Infant Characteristics.
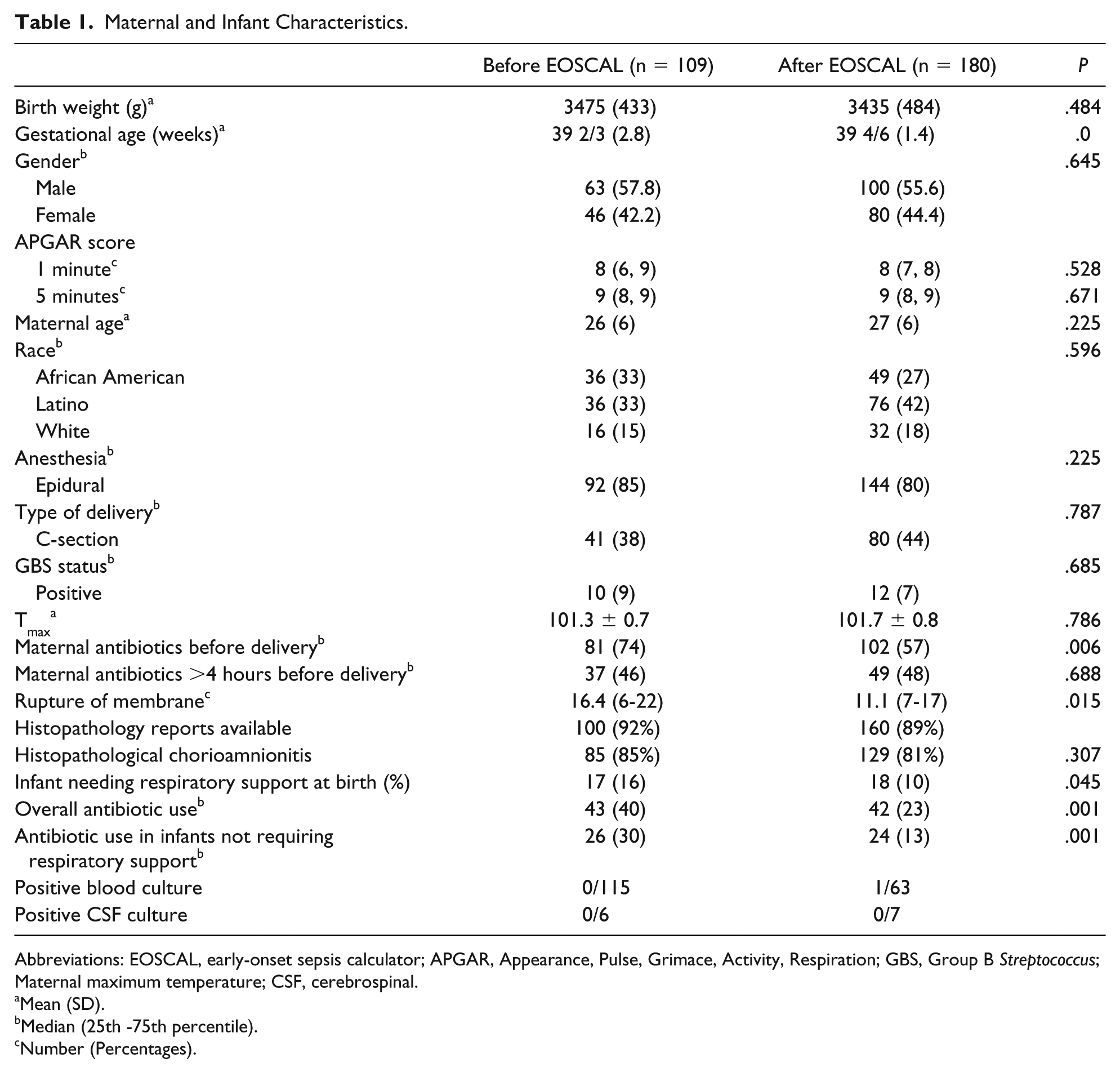
Abbreviations: EOSCAL, early-onset sepsis calculator; APGAR, Appearance, Pulse, Grimace, Activity, Respiration; GBS, Group B Streptococcus; Maternal maximum temperature; CSF, cerebrospinal.
Mean (SD).
Median (25th -75th percentile).
Number (Percentages).

(a) The trend of Overall Antimicrobial Usage Rate (OAUR) before and after EOSCAL. A significant decrease in OAUR from 16.4 to 10.9 per 100 patient days after implementation of EOSCAL (p<0.001). (b)Trend Antimicrobial Usage Rate in infants exposed to MC before and after EOSCAL. A significant decrease in AUR amongst infant exposed to MC from 2.2 to 1.1 per 100 live births after implementation of AUR (p<0.04). (c) Block and Whisker comparing doses of antibiotics used before and after EOSCAL in infants exposed to MC, who received antibiotics. The median doses of antibiotic were 4 (IQR 4-8) after EOSCAL implementation comparing to 8 (IQR 5-14) before intervention (p<0.01).
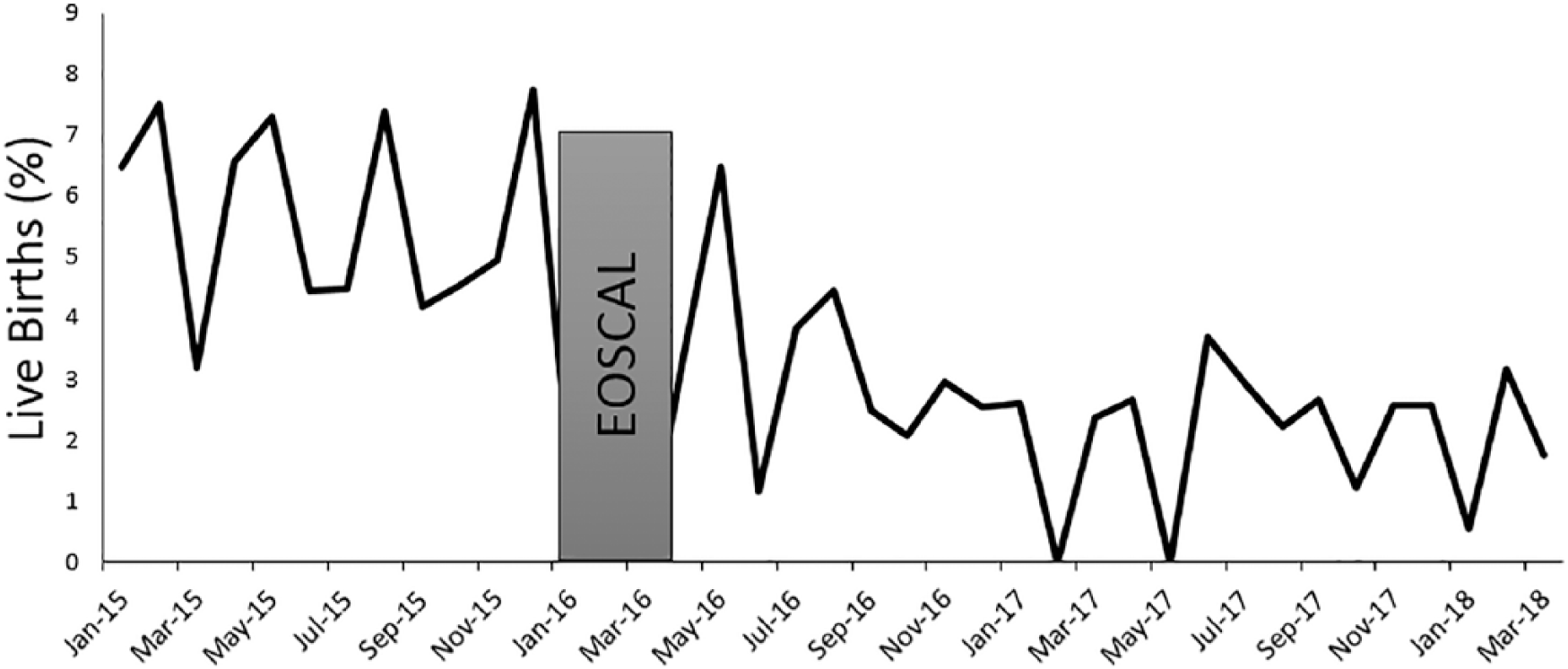
The trend of NICU admission rate amongst ≥36 weeks GA infants exposed to MC. NICU admission rate amongst the infants exposed to MC decreased from 5.7 to 2.5 per 100 live births after implementation of EOSCAL (p<0.001).
There was a significant reduction in LER after implementation of EOSCAL: blood culture (1.5 vs 6.1), CBC (1.9 vs 16.9), and CRP (1.9 vs 11.9) with P < .001 (Figure 5). Readmission rate within 28 days after birth was similar before and after initiation of EOSCAL (P = .45; Table 1). None of the study subjects required antibiotic treatment on readmission in the first 28 days after birth.
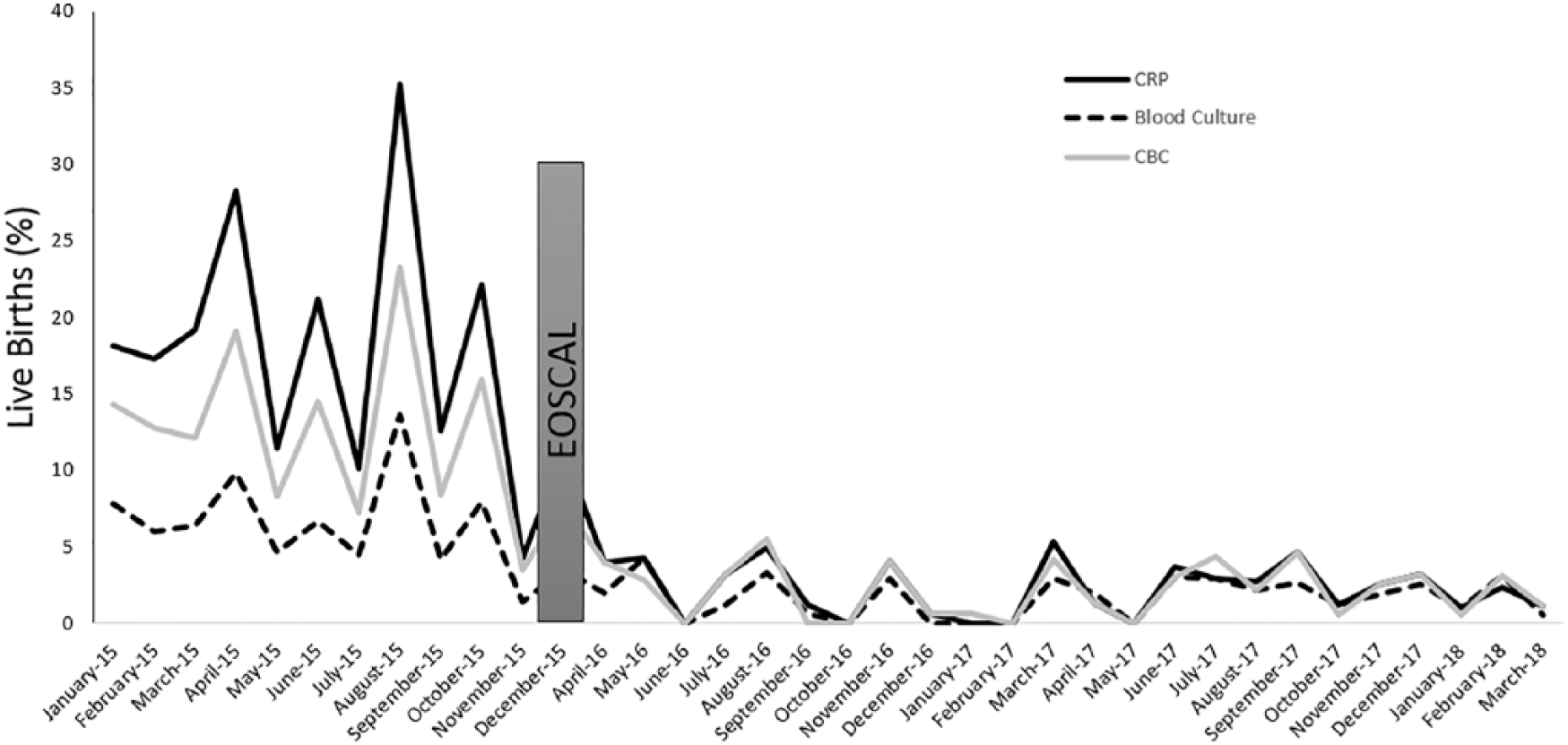
The trend of LER rate amongst ≥36 weeks GA infants exposed to MC. LER for CRP (Solid black line), Blood Culture ( dotted black line) and CBC ( Gray line), all have shown a significant decrease after implementation of EOSCAL (p<0.01).
Discussion
This study aimed to evaluate the effect of implementation of EOSCAL on the management of infants born at ≥ 36 weeks GA and exposed to MC in a single level III nursery care and NICU. Eighty-one percent of asymptomatic infants were managed with their mothers without any LE or antibiotic use after the implementation of EOSCAL in our unit. This study further substantiates the claim to reconsider the CDC approach of treating all infants exposed to MC with antibiotic therapy.
CDC guidelines of administrating antibiotics to asymptomatic infants exposed to MC provide maximum reduction of EOS with acceptance of significant overtreatment. Antibiotic treatment of infants in the neonatal period has been shown to alter the microbiome, increase the risk of late-onset sepsis, and could also be an independent risk factor for the development of chronic diseases like asthma, obesity, and other autoimmune disorders later in life.15,16
The sensitivity of detecting sepsis in an infant can be greatly enhanced by combining physical examination findings with laboratory tests. 17 A large prospective multicenter surveillance study showed that 9% of infants with culture-positive sepsis work asymptomatic within the first 72 hours of life and hence would not be labeled as abnormal by just following serial physical examinations in these infants. 18 Several studies have shown the lack of sensitivity and specificity along with a poor predictive value of white blood cell count, differential count, platelet count, and CRP in the evaluation of an infant at risk for development of EOS.19,20 In fact, abnormal values of laboratory tests have led to unnecessary NICU admissions and antibiotic exposures in asymptomatic and culture-negative infants at risk for development of EOS. 21
EOSCAL has emerged as a powerful screening tool in the management of infants at risk of developing EOS. 14 A retrospective study by Shakib et al showed that 88% of well-appearing infants exposed to MC could be managed with mothers and without any LE, and only 6% to 12% would qualify for antibiotics if managed with EOSCAL. 22 Another recently published study has shown that using EOSCAL for the evaluation of term infants exposed to MC could significantly reduce antibiotic treatment (99.7% vs 2.5%). 23 In our study, we managed 67% of infants without the use of antibiotics by using EOSCAL to evaluate the risk of development of EOS in infants born at ≥36 weeks GA and exposed to MC. The NAR of infants born ≥36 weeks of GA and exposed to MC dropped from 5.7 to 2.4 per 100 live births infants. AUR decreased from 2.2 to 1.1 per 100 live births. Our finding of a reduction in the number of doses of antibiotics during the study period was similar to that reported by Money et al. 23
The incidence of EOS in the infant exposed to MC during the study period was very low (0.35%) but comparable with the published data (0.2% to 0.4%).8,22 The only infant with a positive blood culture in the study population was sick with respiratory distress requiring continuous positive airway pressure with sepsis risk at the birth of 36/1000. The infant was started on antibiotics per EOSCAL recommendations. This infant would qualify for antibiotic therapy even without EOSCAL considering his clinical presentation. We also had 2 blood culture–positive EOS in ≥36 weeks of GA infants who were not exposed to MC. The first infant was born before EOSCAL implementation and was started on empiric antibiotics for a clinical illness, and the EOSCAL recommendations would have been to consider antibiotics. The second infant was born after implementation of EOSCAL, and a term infant was transferred to the NICU at around 12 hours for equivocal signs of sepsis. He qualified for antibiotic therapy on NICU admission per EOSCAL and was later diagnosed with Escherichia coli sepsis and meningitis. To us, he was picked up early with equivocal signs, which necessitated prompt initiation of antibiotics even before he was clinically sick.
All infants exposed to MC need a LE that includes blood culture, CBC, and CRP as a part of the laboratory surveillance of EOS. 24 Blood culture though is the gold standard for the diagnosis of EOS, but its yield depends on various other factors. 25 Clinicians still follow other surrogate markers (CBC and CRP) of sepsis to make decisions concerning initiating or to decide the duration of antibiotic therapy in culture-negative high-risk or clinically sick infants. 17 Abnormal LE in asymptomatic infants can lead to NICU admission and antibiotic exposure in 76% of culture-negative infants who were exposed to MC. 17 In a study by Kiser et al, 20% of infants who were blood culture–negative were treated with prolonged antibiotics solely based on abnormal laboratory values. 21 We still were concerned regarding missing a case of sepsis and were selectively performing CBC/CRP if there was a change in the clinical status of infants. Despite those additional LEs, there was still a significant reduction in LER after the implementation of EOSCAL. We have not noted any missed case of sepsis in the form of readmission to our institution with the diagnosis of sepsis or need of antibiotics within 28 days after birth.
Our study has some limitations including a small sample size in the setting of a single level III tertiary care NICU. The incidence of EOS in the infant exposed to MC during the study period was low (0.35%) but comparable with the published data (0.2% to 0.4%).8,22 Using blood culture as the only criterion for the diagnosis of EOS may underestimate the actual prevalence of EOS. 26 At the time of EOSCAL implementation, few other patients care changes were enacted as a part of antibiotic stewardship. Those changes might also have affected the antibiotic utilization rate. Future large randomized research trials are warranted to evaluate the validity and efficacy of EOSCAL use in the evaluation of EOS in infants exposed to MC.
Conclusion
Use of EOSCAL significantly decreases the rate of NICU admission, AUR, and LER in ≥36 weeks gestation infants exposed to MC.
Footnotes
Author Contributions
VS: substantially contributed to conception or design, contributed to acquisition, analysis, or interpretation of data, drafted the manuscript and critically revised the manuscript for important intellectual content.
CA: critically revised the manuscript for important intellectual content.
KG: contributed to acquisition of data and critically revised the manuscript for important intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.