
Abstract
Objective. To describe the impact of weight on length of stay (LOS) and oxygen requirement among hospitalized children with COVID-19. Methods. This is a retrospective review of 153 children admitted for COVID-19 from March 2020 to October 2021. Body mass index (BMI) percentile and weight-for-age (WFA) percentile were used to determine weight status for children ≥2 years and <2 years respectively. Results. We found 2 distinct patterns for patients <2 years and ≥2 years; The likelihood of needing oxygen and LOS ≥ 5 days was higher for children ≥2 years with BMI ≥ 85th percentile (P = .0415 and P = .0197). Among those <2 years, mean WFA percentile decreased with increasing oxygen need (P = .0325). There was a negative correlation between LOS and WFA percentile (r = −.31, P = .0123). Conclusion. It is important to stratify patients’ risk according to their age, BMI and WFA percentile during hospitalization for COVID 19.
Background
Coronavirus disease 2019 (COVID-19), is a respiratory disease caused by SARS-CoV-2 infection. It first emerged in December 2019 in China, then rapidly spread to many parts of the world, and was declared a pandemic 3 months after.1,2 Individuals of all ages can be infected with different outcomes, from asymptomatic, mild, moderate to severe disease and death, however, it appears that children generally present with less severity when compared to adults.3,4 In the United States, during March 1, 2020, to August 14, 2021, the cumulative incidence of COVID-19–associated hospitalizations in children was 49.7 per 100 000. 5 Previous studies on risk factors among hospitalized children with COVID-19 revealed that obesity is a highly prevalent comorbidity in severe cases of COVID-19 in children.6 -8 One retrospective cohort study in adults found that both underweight and obesity are associated with an increased risk of coronavirus disease 2019 (COVID-19) severity. 9 Another study on severe influenza viral infection in children showed that children who were underweight were prone to severe infection. 10 This study was done to understand how pediatric patients’ weight affects their hospitalization due to COVID-19.
Method
This was a retrospective study of pediatric patients (age ≤ 18 years old) who were admitted to our institution due to COVID-19 from March 2020 to October 2021. Asymptomatic patients who were found to have incidental positive results for COVID-19 or admission diagnosis not related to COVID-19 were excluded from this study. We also excluded patients whose anthropometric data were not available.
We divided patients into 2 groups: children aged less than2 years, and children aged 2 years and older. For patients 2 years and older, CDC growth charts were used according to the American Association of Pediatrics (AAP) recommendation. BMI percentiles were calculated. Categorization of underweight, normal, overweight, and obese were defined by CDC criteria for ≥2 years (below 5th, 5th to <85th, 85th to <95th, and ≥95th BMI percentiles respectively). 11
For patients aged less than 2 years, WHO growth charts were used according to the AAP recommendation. 11 Weight-for-age is a common parameter used among pediatricians to assess children’s growth, and in fact it is used as one of the criteria to diagnose failure to thrive. Weight-for-age also reflects body weight relative to age and is influenced by recent changes in health or nutritional status, thus, WHO growth chart for weight-for-age percentile was used to represent weight status.12,13 We also categorized weight-for-age percentile into 4 groups: below 5th, 5th to <85th, 85th to <95th, and ≥95th.
We assessed the duration of hospital admission in general as well as duration of intensive care admission specifically. We also assessed oxygen therapy requirements among the patients and divided them into 4 groups: (1) no oxygen therapy, (2) low flow oxygen, (3) high flow oxygen, and (4) noninvasive/invasive positive pressure ventilation.
Collected data was analyzed using JMP Pro 16.0.0. All numerical data was summarized using mean and standard deviation. All categorical data was summarized using percentages. Association between numerical variables was studied using Pearson’s correlation coefficient and association between categorical variables was studied using Fisher’s test or Chi square test depending on the number of categories involved. Mean outcomes for 2 groups were studied using a t test and for more than 2 groups using ANOVA. Variation in outcomes for different groups was studied using Levene’s test. Tukey’s HSD was used for Post hoc analysis.
Ethical Approval and Informed Consent
Written informed consent and assent forms were waived. The study was approved by the Institutional Review Borad, University of South Alabama according to Heath Insurance Portability and Accountability Act (HIPAA), Reference number 21-414.
Results
Patient Characteristics
One hundred eighty-two hospitalized children with COVID-19 were identified. Twenty-two patients were excluded due to incidental positive results for COVID-19. Seven patients were excluded due to anthropometric data not available.
A total of 153 patients were included in this study with 91 patients aged ≥2 years, and 62 patients aged <2 years. From our review, none of our patients had concomitant bacterial pneumonia, and we had one patient with pyelonephritis and renal abscess, and one patient with sepsis. There were 4 patients ≥2 years and 2 patients <2 years who had multisystem inflammatory syndrome (MIS-C) and received intravenous immunoglobulin (IVIG), their mean LOS was similar to the mean LOS of the rest of the participants, so we decided to include them in the study.
Patients Aged ≥2 Years
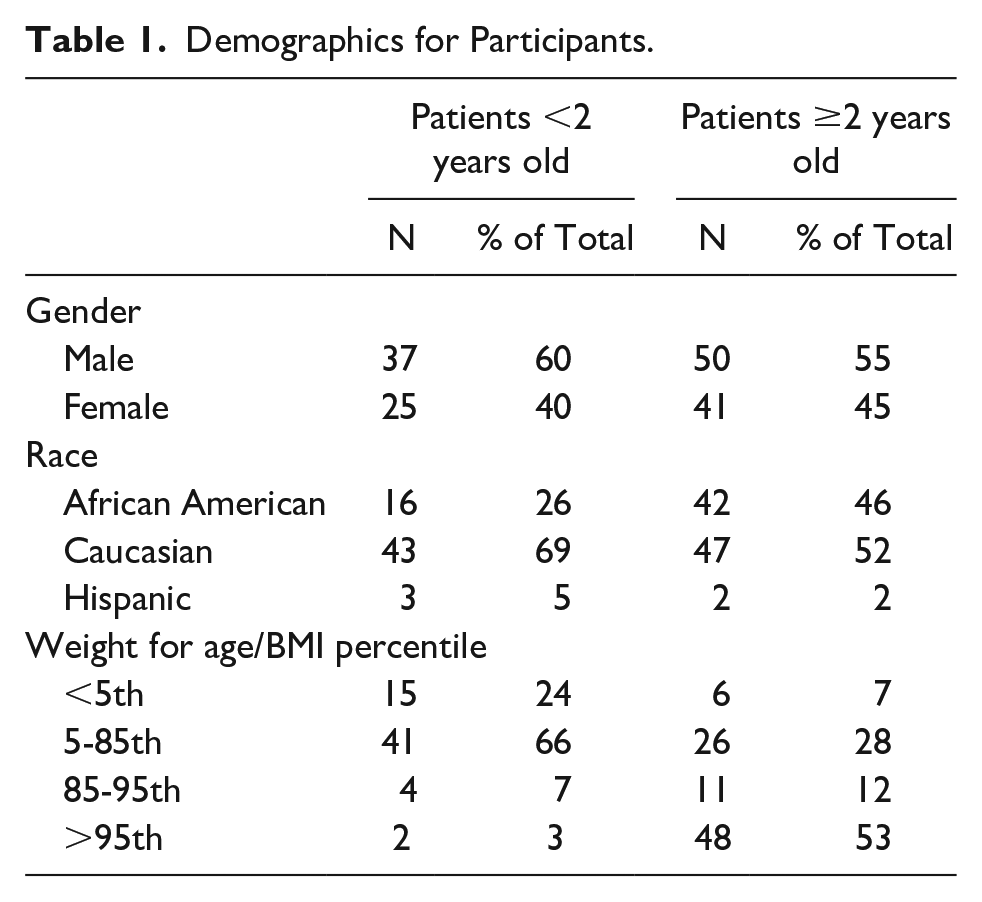
Ninety-one patients were included. There were 50 (55%) males and 41 (45%) females. Mean age was 11.4 years old. Mean age of patients with BMI ≥ 85th percentile was higher compared to those with BMI < 85th percentile, 12 years old versus 8 years old, (P = .0005). More than half of the patients, 48 participants (53%) had BMI ≥ 95th percentile (Table 1). In this cohort, 15% had glucose derangements, there were 7 patients with type 1 diabetes mellitus, 3 patients with type 2 diabetes mellitus, and 4 patients with prediabetes. We also had 6 patients with asthma, 5 patients with sickle cell disease, 2 patients with congenital heart defects, 1 patient with prematurity and bronchopulmonary dysplasia.
Demographics for Participants.
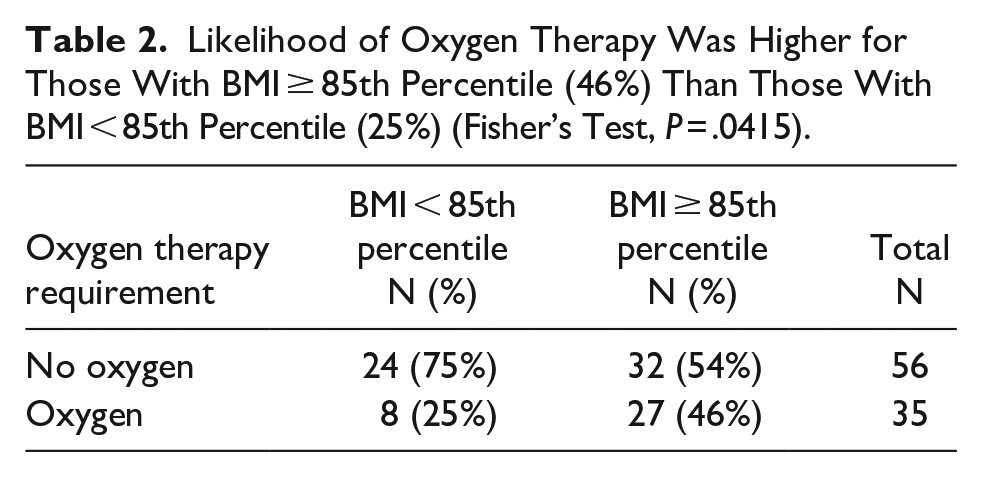
Mean BMI percentile was significantly higher in those who required oxygen therapy (86) as compared to those who were not (73), (P = .0323) (Figure 1). Eighty-eight percent of patients who required positive pressure ventilation were obese and 77% of patients who required low flow oxygen were obese as compared to only 39% of patients who did not need oxygen were obese, (P = .028). We also found that the likelihood for oxygen therapy was higher for those with BMI ≥ 85th percentile (46%) than those with BMI < 85th percentile (25%) (P = .0415) (Table 2).

Mean BMI percentile was higher in those who required oxygen therapy compared to those who did not (86vs 73; t-test, P = .0323).
Likelihood of Oxygen Therapy Was Higher for Those With BMI ≥ 85th Percentile (46%) Than Those With BMI < 85th Percentile (25%) (Fisher’s Test, P = .0415).
There was no significant difference or association between length of stay and BMI percentile, (P = .1181) and (r = .079, P = .4550) respectively. We also did not find any significant difference and association between duration of pediatric intensive care unit (PICU) admission and BMI percentile, (P = .6305) and (r = .26, P = .1671) respectively.
Since the median of length of stay was 5 days, we divided the length of stay to <5 days and ≥5 days. The likelihood of length of stay ≥ 5 days was greater for BMI ≥ 85th percentile than <85th percentile (P = .0197) (Supplemental Table 1).
Patients Aged <2 Years
Sixty-two patients were included. Mean age was 7.2 months old. There were 37 (60%) males and 25 (40%) females. Most of the patients (66%) had normal weight for age (WFA) percentile (Table 1). Out of the 62 patients, 5 patients’ gestational age was unknown, 38 patients were born term, and 19 patients were born preterm. We had 1 patient with bronchopulmonary dysplasia, 1 patient with hypogammaglobulinemia, 1 patient with sickle cell disease, and 2 patients with congenital heart defects. There was no patient with diabetes in this cohort.
In this cohort of 62 patients, 11 patients did not have respiratory viral panel or rapid Respiratory Syncytial Virus (RSV) test done. The other 51 patients who were tested with respiratory viral panel or rapid RSV test, 17 patients tested positive for other viruses (6 patients with rhinovirus, 5 patients with RSV, 3 patients with adenovirus, 2 patients with RSV and rhinovirus, and 1 patient with adenovirus and rhinovirus). We did not find any significant difference between length of stay between patients who were tested positive for other viruses and patients who tested positive for Covid 19 only (P = .1243). There was also no difference in terms of oxygen requirement in the 2 groups (P = .2971).
Mean WFA percentile decreased with increasing need of oxygen therapy (P = .0325) (Supplemental Figure 1). However, post hoc comparison failed to identify which groups were significantly different. One sided hypothesis test was performed, and it showed the mean WFA percentile in the oxygen therapy group was significantly lower than that in no oxygen group (P = .0293) (Figure 2).

Mean WFA percentile was significantly lower in those who required oxygen compared to those who did not (23vs 38; t-test, P = .0293).
A significant negative correlation was observed between length of stay and WFA percentile, (r = −.31, P = .0123). Patients with higher WFA percentile needed shorter length of stay (Figure 3). Mean length of stay also differed significantly for at least 2 WFA percentile groups (P = .0117). Post hoc analysis showed that mean duration for WFA < 5th percentile (8 days) was significantly higher than that for WFA 5th-85th percentile group (3 days) (Supplemental Figure 2).

Significant negative correlation was observed between length of stay and WFA percentile (r = −.31, P = .0123) in patients <2 years old.
Since the median of length of stay was 3 days, we divided the length of stay to <3 days and ≥3 days. The mean WFA percentile was significantly higher for length of stay <3 days (43) compared to ≥3 days (26), (P = .0357) (Supplemental Figure 3).
Discussion
Obesity has been reported to be an independent risk factor for critical illness and longer duration of hospital admissions in a large cohort of hospitalized children with COVID-19. 7 One study also showed that obesity was the most important risk factor for respiratory support use among 50 pediatric cases admitted due to COVID-19. 14 In our study, we found similar results in children aged 2 years and older. The mean BMI percentile was significantly higher in those who required oxygen therapy and the likelihood of oxygen therapy was higher for children with overweight and obesity (BMI ≥ 85th percentile). BMI has significant effects on all lung volumes, functional residual capacity (FRC) and expiratory reserve volume (ERV) decreased exponentially with increasing BMI. 15 Children with obesity breathe at lower lung volumes at rest when compared with children without obesity. This could explain increases in the work of breathing and dyspnea in children with obesity during hyperpnea related to respiratory illnesses. 16 The exact mechanisms linking obesity to severe COVID-19 are likely multifactorial—which stem from obesity-related changes in pulmonary physiology and the genetics to alterations in immune response and inflammatory profiles, endothelial dysfunction, and metabolic dysfunction. 17
In contrast to the fact that obesity was found to be a significant risk factor for severe COVID-19, defined as requiring ICU admission, invasive mechanical ventilation, or in-hospital death, in patients aged 2 years and older, it was not associated with severe COVID-19 in patients aged less than 2 years. 18 In our study, we reported 29% of our patients aged less than 2 years required oxygen therapy and interestingly the mean weight-for-age percentile was significantly lower in those who required oxygen therapy. Prematurity is associated with severe COVID-19 in patients < 2 years old, 18 we do not have information on all our patients’ gestational age, but it is possible low weight is related to prematurity. Previous studies also reported underweight was significantly associated with increased severity of respiratory tract infection due to immunosuppression and malnutrition.10,19 -22
Our study showed that patients aged 2 years and younger with lower weight-for-age percentile had longer length of stay, while patients aged 2 years and older, patients with BMI ≥ 85th percentile had higher likelihood of staying in the hospital for ≥5 days. This was broadly in line with the study done by Tripathi et al which reported increased hospital length of stay for both underweight and obese children when admitted due to COVID-19. 7 Sharma et al also reported pediatric intensive care units and hospital lengths of stays were higher in underweight children, and underweight children were younger when compared to normal or obese children. 23 On the other hand, a study done in hospitalized pediatric patients aged 2 to 18 years showed obese patients had 15% longer hospital stays and 19% higher hospital costs than normal weight patients, when controlled for age, sex, ethnicity, insurance type, calendar year, and primary diagnosis. 24 This U-shaped curve was also reported in mortality rate in pediatric intensive care units with respect to weight centile, and the lowest mortality rate was around 75th weight-for-age centile.25,26
Limitations
We acknowledged a few limitations in our study. This was a small and single center study, which may limit the generalizability of the study’s findings to other settings or populations. Since our study was a retrospective study, there is also possibility of incomplete or inaccurate data, as well as the potential for selection bias in the inclusion of patients. Since it was a retrospective study, we were also not able to assess how weight affects the long term morbidity or mortality of our patients.
There is also a lack of standardization of classification of weight status for patients less than2 years old, and we used weight for age in our study, as gold-standard measurement of length requires a calibrated length board with 2 trained individuals. 27 Two studies in children younger than 2 years old found that the current clinic practice of length measurement is often inaccurate.28,29 Another limitation was that oxygen therapy was usually given due to hypoxemia measured via pulse oximeter; however, regardless of oxygen level, oxygen therapy was also given when patients had symptoms of hypoxia, for example, shortness of breath. 30 There were no definite clinical indications for oxygen therapy, 31 therefore the decision to initiate or discontinue oxygen therapy can be varied based on provider assessment and might not be an objective assessment of severity of disease. This study was conducted from March 2020 to October 2021, so any developments or new insights related to Covid-19 after that time frame would not be considered in this analysis.
Conclusions
Both extremes of weight centiles - underweight and overweight were related to longer length of stay and higher oxygen requirement. Patients aged 2 years and older with BMI ≥ 85th percentile were more likely to require oxygen therapy during hospitalization as well as longer length of stay of ≥5 days. Paradoxically, for patients <2 years old, those with lower weight for age percentile needed longer hospital stay and had higher need for oxygen therapy. Thus, it is important to stratify patients’ risk according to their age, BMI percentile, and weight for age percentile during hospitalization due to COVID-19. Our results may also help to identify children at potentially higher risk of severe COVID-19 who may benefit from vaccination.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X231220873 – Supplemental material for Impact of Weight on Severity of Hospital Course in Children Admitted With COVID-19
Supplemental material, sj-docx-1-gph-10.1177_2333794X231220873 for Impact of Weight on Severity of Hospital Course in Children Admitted With COVID-19 by Nessa Tantivit, Madhuri Mulekar, Anne-Marie Kaulfers and Whei Ying Lim in Global Pediatric Health
Supplemental Material
sj-docx-2-gph-10.1177_2333794X231220873 – Supplemental material for Impact of Weight on Severity of Hospital Course in Children Admitted With COVID-19
Supplemental material, sj-docx-2-gph-10.1177_2333794X231220873 for Impact of Weight on Severity of Hospital Course in Children Admitted With COVID-19 by Nessa Tantivit, Madhuri Mulekar, Anne-Marie Kaulfers and Whei Ying Lim in Global Pediatric Health
Footnotes
Abbreviations
COVID-19 Disease caused by the SARS-CoV2 virus
BMI Body mass index
WFA Weight-for-age
LOS Length of Stay
p P-value
r Pearson correlation coefficient
MISC Multisystem inflammatory syndrome in children
PICU Pediatric intensive care unit
Author Contributions
Dr. Tantivit designed the study, established criteria for inclusion and exclusion studies, submitted documents for IRB approval, collected data from electronic medical record and organized the data, drafted the initial manuscript and approved the final manuscript as submitted. Dr. Mulekar conducted statistical analysis, reviewed the manuscript, and approved the final manuscript as submitted. Dr. Kaulfers reviewed and revised the manuscript, and approved the final manuscript as submitted. Dr. Lim determined the research question, designed the study, established criteria for inclusion and exclusion studies, drafted the initial manuscript, reviewed, revised the manuscript, and approved the final manuscript as submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Written informed consent and assent forms were waived. The study was approved by the Institutional Review Borad, University of South Alabama according to Heath Insurance Portability and Accountability Act (HIPAA), Reference number 21-414.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.