
Abstract
This study explored the relationship between BMI trajectories and the duration of obesity in Thai children diagnosed with hypertension. Demographic and blood pressure data from 536 children (270 boys, 50.3%) from a school in Bangkok, Thailand were collected. Hypertension was defined as blood pressure above the cutoff values specified in the 2017 American Academy of Pediatrics guidelines on 3 occasions. Records of BMI over the previous 3 years were reviewed. The prevalence of hypertension was 2.61% (14/536). Complete data on BMI trajectories were available in 421 non-hypertensive and 12 hypertensive children. The increase in BMI z-score over the previous 3 years was significantly greater in the hypertensive group than the non-hypertensive group, 1.45 (95% CI 0.42 to 1.88) versus 0.09 (95% CI: −0.35, 0.65), P = .008. In conclusion, children with a confirmed diagnosis of hypertension had a greater increase in BMI over the past 3 years than non-hypertensive children.
Introduction
The prevalence of hypertension (HT) in children has been increasing over recent decades. According to data from the U.S. National Health and Nutrition Examination Survey (NHANES), the percentages of children with elevated blood pressure (BP) increased from 8.2% in girls and 15.8% in boys during 1999 to 2008 to 12.6% in girls and 19.2% in boys during 1988 to 1994. 1 A 2015 study in Thai school-age children found that 21.4% of girls and 24.3% of boys had elevated BP. 2 Another study found that rates of obesity were 12.8% in girls and 30.6% in boys and that obesity increased the risk of elevated BP over 10-fold. 3 Studies from other Asian countries also found increases over time in the prevalence of children with obesity and HT.4-7
Given that obesity is strongly associated with HT, a long duration of obesity may contribute to the development of HT. Tanamas et al 8 reported results of a 15-year-longitudinal study, the Framingham Heart Study, in almost 3000 adults aged 30 to 62 years without baseline HT, and found a positive correlation between the duration of obesity and the incidence of HT in women. In contrast, a study by Hekimzoy and Oktem 9 found no significant relationship between the duration of obesity and HT in 200 adults. Aris et al 10 studied a cohort of 1170 children and found that rapid body mass index (BMI) z-score increase during the first 2 years of life predicted obesity status, but failed to predict pre-hypertensive status at 5 years of age. East et al 11 however, found that a BMI > 25 kg/m2 at 13 years of age was associated with adult HT.
This study explored the impact of BMI trajectories and duration of obesity on the development of HT in Thai school-aged children. Most previous studies reported the association of BMI z-score and HT using BP measurement at only a single visit. It is therefore possible that some participants had elevated BP in their doctor’s offices (a phenomenon known as “white-coat HT”) but did not actually have HT. In contrast to these studies, we defined HT as elevated BP over 3 consecutive visits, 4 to 6 months apart.
Subjects and Methods
We conducted a cross-sectional study with a retrospective review of records between August 2017 and September 2018 in a primary school in central Bangkok, Thailand. The study was performed in conjunction with the annual school health check-up provided to every school-age child in Bangkok, and it was approved by the Ramathibodi Hospital Ethics Committee for Human Research (ID 03-60-32 and MURA 2020/1363). Given previous research showing that the prevalence of HT in Thai children is approximately 4%, 3 we estimated that the sample size should be at least 456, which provided a power of 95% at alpha = .05.
Students in fourth to sixth grades were included in the study. Demographic and health data including weight, height, waist circumference (WC), WC-to-height ratio (WHR) and BP were collected. We also performed a retrospective review of annual records containing the weight and height of each child during the current year and over the past 3 years. Weight was measured in kilograms (kg) with 1 decimal point. Height was measured in centimeters (cm) with 1 decimal point. Waist circumference was measured at the midpoint between the lower rib and the top of the iliac crest in cm with 1 decimal point. BP was measured by trained research and school nurses using the Dynamap V100 (GE Healthcare, USA) on the right arm of each child in a sitting position after resting for 5 minutes. A cuff size with a width of at least 40% and the length of at least 80% of the mid-arm circumference was used, as recommended by the American Academy of Pediatrics (AAP). 12 Each child had 3 BP measurements, with 5-minute intervals between measurements. The average of the last 2 measurements was used for analysis. At the first visit, children with either systolic BP (SBP) or diastolic BP (DBP) ≥ the 95th percentile based on age, gender, and height (according to the 2017 AAP guidelines) 13 had a second visit for BP measurement within 4 to 6 months. Children whose BP remained high underwent a third visit for BP measurement within 4 to 6 months of the second visit. Children with persistently elevated BP, ≥ the 95th percentile, at the 3 visits were diagnosed as having HT. The methods of this study and preliminary results after the first 2 visits of BP measurements have been published previously. 14
BMI was calculated as follows: weight (kg)/height (m)2. Z-scores of BMI were calculated using the World Health Organization 15 growth reference for age and gender. Obesity was defined as a BMI z-score ≥2. The waist circumference to height ratio (WHR) was calculated using the formula: waist circumference (cm)/height (cm). BP z-scores were calculated using the normative BP table published in the 2017 AAP guideline. 13 The 95th percentile (P95th) was considered a +1.65 z-score.
Institutionally licensed SPSS software was used for statistical analysis. Demographic data were presented as frequency or median and interquartile range (IQR), as appropriate. Mann-Whitney U test was used to test the difference in continuous data between 2 groups, as appropriate. The Wilcoxon Signed Rank test was used to test the difference of 2 paired-parameters. Chi-square tests were used to test the difference of categorical data between 2 or more groups, as appropriate. Bivariate logistic regression models of the factors associated with HT were created. The current BMI z-score, age, gender, and height were included in the multivariate analysis. A P of ≤.05 was considered statistically significant.
Results
A total of 536 participants, including 270 boys (50.3%) and 266 girls (49.6%), were included in the study with a mean age of 10.2 ± 0.9 years. The overall prevalence of HT, based on those with persistent elevated BP measurements across 3 visits, was 2.61% (14 of the 536 students). At the first visit for BP measurement, 160 (29.8%) children had either SBP or DBP ≥ the 95th percentile. A total of 58 of these 160 children (10.8% of the sample) continued to have elevated BP at the second visit. At the third visit, BP was assessed in 53 of 58 children, and 14 of these had confirmed HT.
The previous 3-year records of BMI z-score were available for 433 children (12 children with HT and 421 children without HT). Demographic and health data did not differ significantly between the 103 children who did not have the complete 3-year records of BMI z-score and the 433 children who had complete records (see Supplemental Table S1). A comparison of demographic data and BMI in children with and without HT is shown in Table 1. A box plot of the BMI z-score over the past 3 years, stratified by HT status, is shown in Figure 1. Within groups, the median increase in BMI z-score over the previous 3 years was significantly different both in the hypertensive group (1.7 to 4.12, P = .015) and the non-hypertensive group (0.1 to 0.24, P = .001). Moreover, the absolute increase in BMI z-score over the past 3 years was significantly greater in the hypertensive group than in the non-hypertensive group, 1.45 (0.42, 1.88) versus 0.09 (−0.35, 0.65), P = 008.
Demographic and Health Data of Study Participants.

Bold font indicates statistical significance.

BMI trajectories over the 4-year-period between normotensive (N = 421) and hypertensive groups (N = 12).
The rate of HT differed significantly by the duration of obesity, P = .009. Rates of HT in children with obesity were 5/54 (9.3%), 2/26 (7.7%), and 0/16 (0%) among those who were obese over 3 years, 2 years, and 1 year, respectively. Among the non-obese children, 4/306 (1.3%) had hypertension, and 1/31 (3.2%) of children who were obese during the most recent year had HT. The group of children who were obese for at least 2 years had a significantly greater likelihood of HT than the non-obese group or the group of children who were obese for less than 1 year, p = .002. Change in BMI also differed significantly by the duration of obesity, P < .001. The median (IQR) of the current BMI z-scores were 4.1 (3.6, 5.1), 3.2 (2.5, 4.8), and 2.6 (2.0, 3.2) among children with obesity for 3 years, 2 years, and 1 year, respectively. In contrast, the median (IQR) of the current BMI z-scores were 2.1 (1.5, 2.7) among children with obesity in the current year and −0.2 (−0.7, 0.4) among non-obese children. Regarding the group of 102 children with obesity in the current year, there were 8 children had HT and the other 93 children without HT. Demographic and health data between the 2 groups were compared in Table 2. There was a significantly higher WHR in the group with HT compared to that of the group without HT, P = .008.
Demographic and Health Data of 101 Study Participants with Recent Obesity.

Bold font indicates statistical significance.
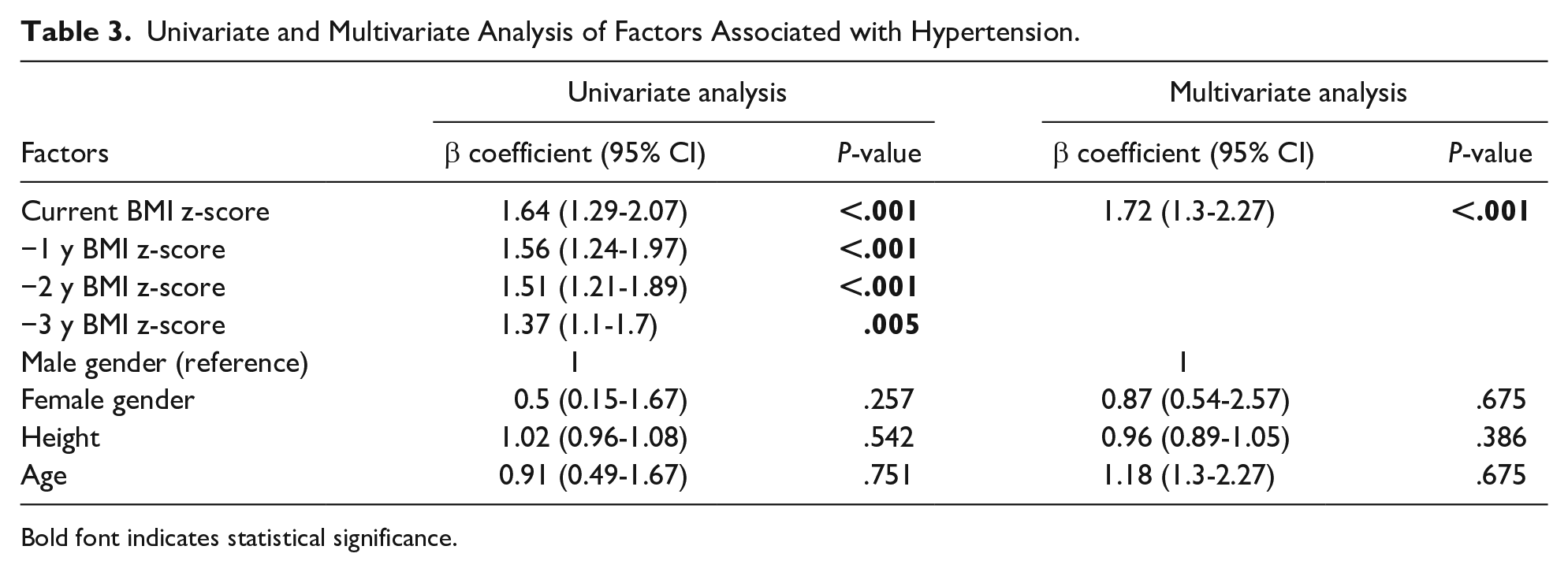
In univariate analysis, the BMI z-score during the current year had a stronger association with the diagnosis of HT than the BMI z-score of past years. Age, gender, and height were not significantly associated with HT. In the multivariate model, the current year BMI z-score was independently associated with HT after adjusting for age, gender, and height (see Table 3).
Univariate and Multivariate Analysis of Factors Associated with Hypertension.
Bold font indicates statistical significance.
Discussion
The present study showed the overall rate of HT was 2.61%. The increase in BMI z-score over the past 3 years was significantly greater in the group of children with HT than in the group without HT. Moreover, the proportion of HT among children with obesity for at least 2 years was greater than that of the group with obesity for 1 year or less.
The overall rate of HT in the present study at 2.61% was much lower than those reported from the previous studies in Thailand. The most likely explanation for this was that the diagnosis of HT in the present study was made by BP measurements over the 3 consecutive visits while the previous studies reported the rate of HT by only 1 visit of BP measurement. Therefore, some children who expressed anxiety and had elevated BP on the first few BP measurements had been excluded and the remaining children were the group with sustained HT.
The pathophysiology of obesity-induced HT is not well understood, but various mechanisms have been proposed. Hyperleptinemia caused by an increased production of adipose tissue to counteract obesity activates the sympathetic nervous system and leads to increased BP. 16 Moreover, increased visceral fat mass that leads to compression of the kidneys activates the renin-angiotensin-aldosterone system and leads to increased sodium absorption. 16 Therefore, a longer duration of obesity might lead to a greater risk of HT. A prolonged duration of obesity in adults not only increases the risk of HT, but also increases the risk of metabolic syndrome and diabetes. Fisher et al 17 studied 7532 adults without metabolic syndrome and followed them for 2 years. Among participants with a 2-point gain in BMI, the mean number of criteria for metabolic syndrome increased from 1.07 to 1.52, whereas among participants with a 2-point loss in BMI, the mean number of criteria decreased from 1.64 to 1.16. Another study in 837 adults found that the duration of obesity had a moderate effect on the frequency of diabetes. 18 In contrast, Hekimzoy and Oktem 9 did a cross-sectional study in 200 women and did not find a relationship between HT and duration of obesity. The reasons for these inconsistent findings remain unclear.
In children, a greater risk of HT and a prolonged duration of obesity were found to be associated with metabolic syndrome. Zamrazilova et al 19 found that children with obesity and metabolic syndrome had a longer duration of obesity than children without metabolic syndrome. The study also found that there was a significantly greater BMI z-score in children with metabolic syndrome than in those without metabolic syndrome at the age of 3 to 7 years, whereas the BMI z-scores at the age of 13 years were comparable. This finding suggests that there is a critical time period during which children with obesity are susceptible to the development of metabolic syndrome. The present study found that the group of children who were obese for at least 2 years had a significantly greater likelihood of HT than the non-obese group or those who were obese for less than 1 year. The most likely explanation for this finding is the greater BMI z-score found in the group with a longer duration of obesity.
Among 12 children with HT, 8 children were obese in the current year and there were 4 children that were not obese. This raised the concern that these 4 children might have underlying causes of HT or familial HT. On the other hand, these 4 children might have white-coat HT as the diagnosis of HT had not been confirmed by ambulatory blood pressure monitoring. In comparison of demographic and health data between obese children in the current year who had HT (8 children) and without HT (93 children), the present study revealed that WHR was significantly greater in the group with HT than in the group without HT. The other BMI parameters also were slightly greater in the group with HT than in the group without HT. However, the number of obese children with HT was very small and it limited a meaningful statistical significance.
A strength of this study is that the diagnosis of HT was based on 3 BP measurements conducted on 3 occasions, as recommended by AAP guidelines. Moreover, only 5 children did not complete the third BP assessment. Nonetheless, this study also has limitations including that it was retrospective, and the available records of weight and height over the previous 3 years were only 80% complete. The overall number of children with HT was small. Additionally, BP measurements were obtained by the oscillometric method, not the auscultatory method that is recommended by the AAP guideline, which could over-inflate BP values.
Conclusions
Children with a confirmed diagnosis of HT had a greater increase in BMI z-score over the past 3 years than did non-hypertensive children. The most recent BMI z-score was the only significant risk factor associated with HT.
Supplemental Material
sj-pdf-1-gph-10.1177_2333794X211012998 – Supplemental material for Body Mass Index Trajectories and Duration of Obesity in Thai Children Diagnosed with Hypertension
Supplemental material, sj-pdf-1-gph-10.1177_2333794X211012998 for Body Mass Index Trajectories and Duration of Obesity in Thai Children Diagnosed with Hypertension by Witchuri Paksi, Suthatip Sirijunpen, Pracha Nuntnarumit and Kwanchai Pirojsakul in Global Pediatric Health
Footnotes
Acknowledgements
The authors wish to thank the director and the nurses of the school participated in this study. The authors also would like to acknowledge financial support for this study from a Ramathibodi Hospital Research grant. We thank Diane Civic, PhD, from Edanz Group (![]() ) for editing a draft of this manuscript.
) for editing a draft of this manuscript.
List of Abbreviations
BP, blood pressure; AAP, American Academy of Pediatrics; HT, hypertension; WC, waist circumference; kg, kilograms; cm, centimeter; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; m, meter; WHR, waist circumference to height ratio; IQR, interquartile range; ROC, receiver operating characteristic curve; SD, standard deviation.
Authors’ Contributions
W.P., S.S., P.N., and K.P. made substantial contributions to the acquisition of data and interpretation of data. K.P. made substantial contributions to the conception and design of the study and drafting the manuscript. All authors reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a Ramathibodi Hospital Research grant.
Ethics Approval
This study has been approved by the Human Research Ethics Committee, Faculty of Medicine Ramathibodi Hospital Mahidol University (ID 03-60-32 and MURA 2020/1363).
Availability of the Dataset
The dataset used during the current study is available from the corresponding author by reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.