
Abstract
Objective
To investigate the relationships between body mass index (BMI) and sex, and asthma-like disease and current wheeze in Han children in Nanjing, China.
Methods
Han children aged 3–14 years were recruited. Height and weight were measured; individuals were classified into obesity, thinness and normal-weight groups on the basis of the calculated BMI. Questionnaires were used to measure prevalence of asthma-like disease and current wheeze. Results were evaluated using the χ2-test, odds ratios with 95% confidence intervals and multivariate logistic regression analyses.
Results
In total 12 092 children (6 331 boys and 5 761 girls) were included. Rates of normal weight, obesity and thinness were 8915/12 092 (73.73%), 1479/12 092 (12.23%) and 1698/12 092 (14.04%), respectively. Asthma-like disease and current wheeze were reported in 2051/12 092 (16.96%) and 400/12 092 (3.31%), respectively. An increased BMI was associated with a greater risk of asthma-like disease; this relationship was strongest in girls. Current wheeze was associated positively with obesity and negatively with thinness, but only among boys. Boys had a greater risk of asthma-like disease and current wheeze than girls.
Conclusions
BMI and sex were associated independently with the prevalence of asthma-like disease and current wheeze in Han Chinese children.
Introduction
Asthma is a major cause of chronic morbidity and mortality throughout the world and its prevalence has increased considerably over the past 20 years, especially in children. 1 In recent decades there has also been a substantial increase in the prevalence of obesity among children. 2 A number of studies have shown that obesity is an important risk factor for asthma and wheeze. A study carried out in the USA found that the risk of obese children having asthma was two times higher than for children with normal body weight. 3 An Asian study by the Prediction of Allergies in Taiwanese Children (PATCH) group, involving 5 476 children showed that an elevated body mass index (BMI), was associated with a greater prevalence of wheezing and eczema. 4 In many studies, especially those based in the USA, the term ‘overweight/obese’ has usually been defined as the 95th centile of the US Center for Disease Control reference curves for BMI, with children at or above the 85th (but below the 95th) centile classified as being at risk. 5 The prevalence of asthma in the USA has been reported to be higher than in many other countries. 6 Furthermore, in a US study in children from racial minority subgroups with different genetic backgrounds, obesity prevalence ranged from 4.4% in Asian Indian children up to 13.0% in American Indian/Alaska Native children. 7 Therefore, it is important for such surveys to take ethnicity into account. A number of studies investigating the relationship between the incidence of asthma or asthma-like symptoms and increasing BMI have included information on individuals’ sex.3,4,6–8 Nevertheless, there is still a need for further studies that include these key factors and involve large numbers of individuals.
The present large population study aimed to investigate whether BMI and sex are associated with the prevalence of asthma-like disease and current wheeze, in children from the Han ethnic group in Nanjing, China.
Subjects and methods
Every child belonging to the Han ethnic group from 16 kindergartens and 12 elementary schools, covering the age range 3–14 years old, in the northern part of Nanjing City, China, was selected to participate in the study. Data collection took place between August 2010 and January 2011. Children with major systemic diseases or syndromes were excluded.
The children’s parents completed a set of questions derived from the International Study of Asthma and Allergies in Childhood (ISAAC) core questionnaire. 9 The ISAAC is a well-validated standard tool for epidemiological investigation of the prevalence and severity of atopic disorders, such as wheezing and rhinitis, for use in children living in different countries.10,11 In the present study, the presence of asthma-like disease was based on a positive response to the question, ‘Has your child ever been diagnosed with asthma, asthmatic bronchitis, chronic bronchitis or asthmatic pneumonia?’. The presence of current wheeze was based on a positive response to the question on asthma-like disease, plus a positive response to the question, ‘In the last 12 months, has your child had wheezing in the chest?’. The questionnaire also gathered information on birth date, sex, height, weight, home address, and a history of asthma or other allergic disorders in the parents and grandparents. The date on which the questionnaire was completed was recorded for each individual.
All the parents provided verbal informed consent and anonymity was preserved in the data analysis. The study was approved by the Committee on Human Experimentation, Nanjing Children’s Hospital, Nanjing Medical University, Nanjing, China, and was conducted in accordance with the Helsinki Declaration of 1964, as revised in 2013. 12
The weight and height of each participant were measured according to a standard protocol. All children were weighed while wearing light clothes and without shoes. Measurements were conducted using a calibrated weighing scale and stadiometer. Weight (in kg) was measured to the nearest 1 kg and height (in cm) was measured to the nearest 1 cm. The BMI for each study participant (defined as weight in kg divided by height in m2), was calculated from these measurements.
The study population was divided according to age (<7 years versus ≥7 years) and sex. Participants were also divided into three groups according to BMI, based on age- and sex-specific criteria for normal weight, obesity 13 and thinness, 14 using well-validated standards developed on the basis of worldwide surveys.15,16
Statistical analyses
The prevalence of asthma-like disease and current wheeze in the different BMI and sex groups were compared using the χ2-test. Odds ratio (OR) and 95% confidence intervals (CI) were derived in the different BMI, sex and age groups. Multivariate logistic regression analysis was performed to estimate the effects of BMI, sex and age independently; the confounding factor of BMI was treated as ranked data, whereas sex and age were treated as dichotomous data. A P-value <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 13.0 (SPSS Inc., Chicago, IL, USA).
Results
Prevalence of obesity, thinness, asthma-like disease and current wheeze in Han Chinese children.

Data presented as n (%) of children.
BMI
Of the 2 051 children with asthma-like disease, 292 (14%) were in the obesity group. In contrast, of the 10 041 children who did not have asthma-like disease, only 1 187 (12%) were obese. This difference was statistically significant (P = 0.002). A similar difference was observed when comparing obesity rates in those with and without current wheeze. Of the 400 children with current wheeze, 63 (16%) were in the obesity group, whereas only 1 416 (12%) of the 11 692 children who did not have current wheeze were obese (P = 0.029).
Odds ratio analysis of the prevalence of asthma-like disease and current wheeze in the obesity and thinness groups compared with the normal-weight group in Han Chinese children.
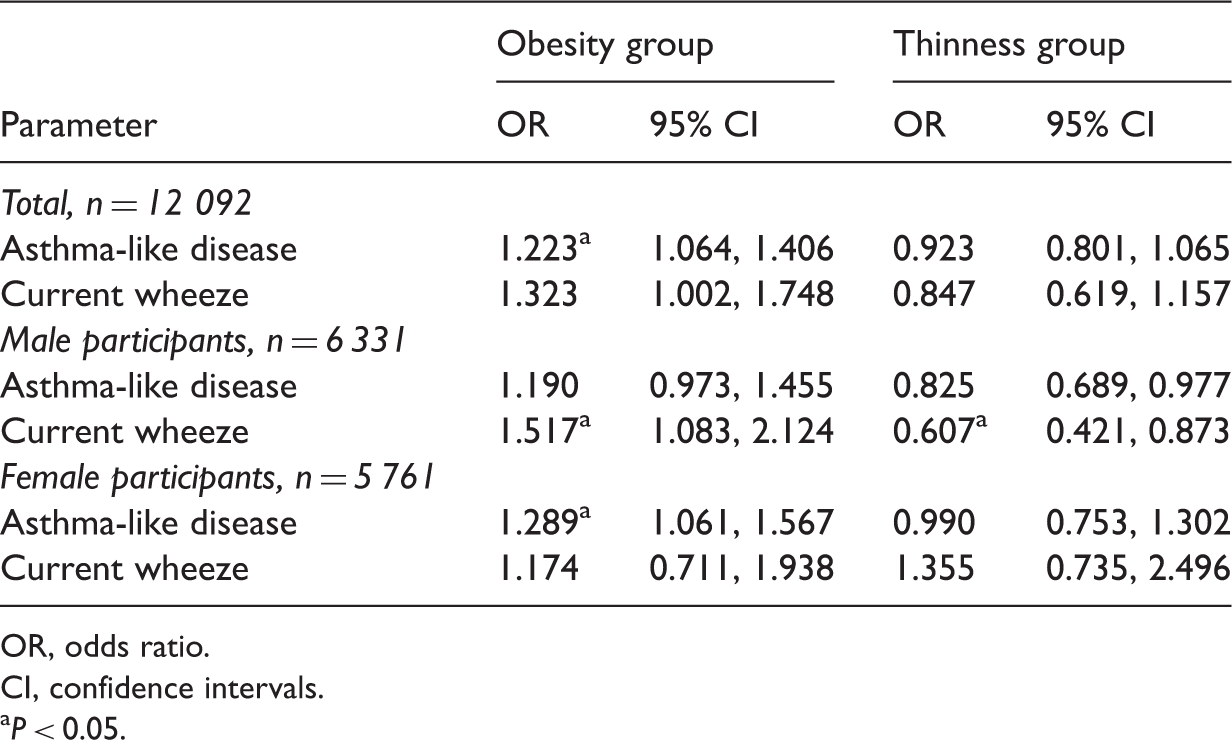
OR, odds ratio.
CI, confidence intervals.
P < 0.05.
Sex
The overall prevalence of asthma-like disease and current wheeze were compared between the sexes, using OR. The risk of asthma-like disease was significantly higher in male subjects than in female subjects (OR 1.284, 95% CI 1.167, 1.414, P < 0.001). Likewise, a significantly higher risk of current wheeze was observed in male, compared with female, subjects (OR 2.202, 95% CI 1.772, 2.737, P < 0.001).
Multivariate logistic regression analysis
Multivariate logistic regression analyses of risk factors for asthma-like disease and current wheeze in Han Chinese children.

OR, odds ratio.
CI, confidence intervals.
NS, not statistically significant (P ≥ 0.05).
Discussion
The present study revealed a significant relationship between asthma-like disease and obesity among children from the Han ethnic group in Nanjing, China.
Both χ2-test and multivariate logistic regression analyses showed that an increasing BMI was significantly and independently associated with a higher prevalence of asthma-like disease in children. While a number of studies have shown that asthma or asthma-like symptoms were significantly more frequent among obese children,4,17–19 the associated OR have varied. Interaction analysis of BMI and sex suggested that the effect of BMI on asthma-like disease does not differ between the sexes. This is in line with some reports, 20 but some studies have revealed a stronger association between BMI and asthma-like disease in boys than in girls3,8 or conversely a stronger association in girls than in boyssubjects.18,21,22 Reported differences between the sexes in the effect of body size on asthma suggest it is important to specify the age at which an effect is observed, as some associations may only be seen during certain periods of development. 23 The present study also demonstrated a significant association between BMI and current wheeze, but only in boys.
While the epidemiological evidence linking asthma or asthma-like symptoms and obesity is impressive, the mechanism of the link between these diseases is far from clear. Since variations in this association are seen in results from different areas and ethnic groups,3,4,10,21 it has been proposed that asthma and obesity may be linked via specific regions of the human genome, such as chromosomes 5q and 6p21. 24 It is thought that interactions between genetic and environmental factors may be important. 24 In addition, it has been suggested that mechanical factors such as the functional residual capacity of the lung (which is lower in obese subjects), breathing patterns (obese subjects have a higher breathing rate and a lower tidal volume) and alterations in smooth-muscle structure and function may also play a role. 18
Adipose tissue is not a passive energy storage depot; 25 it has been shown that obesity affects the immune system and promotes inflammation, which could potentially promote the development of a variety of chronic conditions and diseases. 26 Furthermore, it has been reported that the cellular and signalling networks linked to the immune system undergo changes in lean individuals, and activated macrophages and eosinophils have been found in adipose tissues. 27 Changes in macrophage function have been reported in organs other than adipose tissue, which could contribute to the development of steatohepatitis. 27 In addition, studies have suggested that alveolar macrophage function may be altered in obesity. 25
The results of the present study indicated that boys were more likely than girls to suffer from current wheeze, which is consistent with the results of previous studies. 8 This may be due to a higher degree of physical activity among boys, leading to a greater likelihood of discovering their symptoms. 28 The hormone oestrogen may also play a role in the sex difference. 24
In conclusion, the present study, which had a high participation rate and used the well-validated ISAAC criteria, showed that an increase in BMI was associated with an increased risk of asthma-like disease in Han children from Nanjing, China. In addition, sex may also play a role in the presence of current wheeze. Knowledge of this association may help inform public health decisions concerning asthma diagnosis, management and prevention. However, because of the cross-sectional design of the study, and since only sex and age were used as confounding factors, a causal association cannot be assumed on the basis of the present study. Additional investigations are needed to gain further insight into the underlying mechanisms.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was financially supported by the Nanjing City Scientific and Technological Foundation (200901064) and funds for training were received from the Department of Disease Control of Ministry of Health, Beijing, China.
Acknowledgements
The authors thank the Department of Disease Control of Ministry of Health for granting training funds to this programme and the Capital Institute of Paediatrics and Chinese Centre for Disease Control and Prevention for providing technical support.