
Abstract
Posterior reversible encephalopathy syndrome (PRES) is a clinico-radiological entity occurring during several conditions and more frequently in those associated with severe hypertension. The diagnostic approach is possible by considering the clinical context and MRI data, where white matter abnormalities are observed predominantly in the parietal and occipital territories secondary to the formation of a vasogenic edema. The evolution is characterized by a reversibility of the lesions in case of early diagnosis and management. The authors report a case of reversible posterior encephalopathy in a 12-year-old child who presented with a status epilepticus, revealing an acute renal failure.
Introduction
Posterior reversible encephalopathy syndrome (PRES) is a clinical-radiological entity first described in 1996. 1 In this entity, neurological manifestations associated with white matter abnormalities predominantly in parietal and occipital territories are found, the reversibility of which is a fundamental characteristic. Numerous cases have been reported, occurring in a variety of clinical conditions and with a wide range of clinical and imaging findings. We report a case of PRES revealing an acute renal failure in a child.
Medical Observation
A 12-year-old girl, with good psychomotor development, presented a convulsive state, which justified her hospitalization in intensive care. The family did not report any familial or medicosurgical history. The symptomatology was of sudden onset and made of several generalized tonic-clonic seizures, prolonged in time with an alteration of the consciousness during the inter-critical periods, in the absence of fever. In emergency, the cerebral CT scan did not find any abnormality, while the biological assessment revealed a renal insufficiency with a creatinine at 78 mg/l, that is to say a glomerular filtration rate at 6 ml/minute according to the Swartz formula, the urea at 1.18 g/l. The hypothesis of renal failure secondary to acute post-streptococcal glomerulonephritis (GNA) was retained in the face of the positivity of the anti-streptolysin antibody (ASLO) test. In addition, the monitoring of vital constants showed an increase in blood pressure, which averaged 160/115 mmHg. The lumbar puncture as well as the viral serologies were normal, which did not argue in favor of a viral encephalitis. The MRI performed as a delayed emergency showed white matter abnormalities hyperintenses in T2WI and FLAIR, without any DWI abnormally, thus suggesting a vasogenic edema whose distribution was bilateral, coarsely symmetrical with a predominance of the parietal and occipital territories, although the temporal and frontal lobes were also affected (Figure 1). The correlation of the lesions with the imaging, clinical and biological data allowed us to retain the diagnosis of PRES. The management consisted of control of blood pressure with calcium channel blockers associated with hemodialysis sessions and antiepileptic treatment. The evolution was favorable with a complete disappearance of the symptomatology as well as a clear regression of the lesions at the control MRI at 1 month interval (Figure 2).
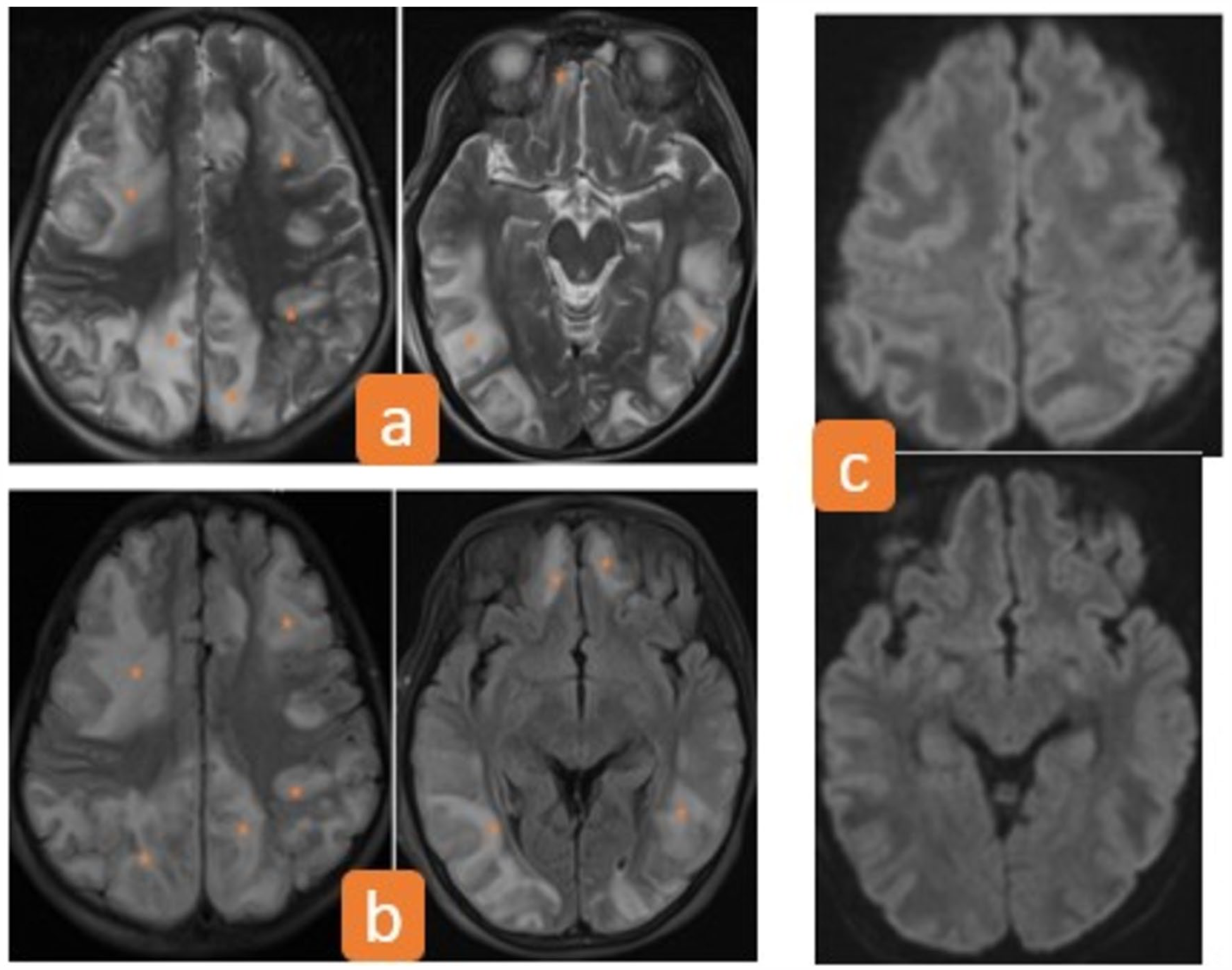
Brain MRI in a 12-year-old child presenting with status epilepticus revealing signal abnormalities of the subcortical white matter, hyperintense on T2WI (a) and FLAIR (b) axial sections, without any translation on DWI (c) related to vasogenic edema with bilateral, symmetrical distribution, predominantly in the parietal and occipital territories, with frontal and temporal lobes involved.

MRI check-up at 1 month interval showing a clear regression of the lesions on the T2WI (a), FLAIR (b), and DWI (c).
Discussion
Posterior reversible encephalopathy syndrome or PRES is a clinico-radiological entity of diverse etiology, sharing similarities in its clinical and radiological manifestations. It is observed both in adults and in the pediatric population. The pathophysiology of PRES is not yet fully understood, however, it is thought to be due to a disturbance of the autoregulation of cerebral vascular pressures and/or lesions of the endothelium leading to the formation of vasogenic cerebral edema. 2 Therefore, this entity occurs only in certain specific conditions (Table 1), and more frequently in cases of arterial hypertension with a diastolic blood pressure greater than 120 mmHg. In this condition, PRES represents one of the complications of hypertensive encephalopathy. In children with renal disease, the incidence of PRES is estimated at between 4% and 9%. 3 In this population, PRES occurs more frequently in cases of acute or chronic renal failure, but it can also occur in cases where renal function is preserved. Uncontrolled arterial hypertension remains the main risk factor, but other factors such as hypoproteinemia and hypocalcemia also contribute to the development of cerebral edema. 4 Drug risk factors, including some used in the treatment of renal disease, may also be involved, in particular calcium channel blockers, corticoids, cyclosporines, and other immunosuppressants. . .The clinical manifestations during PRES are variable. Classically, there are visual disturbances of variable magnitude, ranging from visual blurring to cortical blindness, psychomotor slowing, confusion or agitation, partial convulsions which tend to be generalized, or even a status epilepticus as in our patient. Nausea and vomiting are frequently associated, while headaches are rare. Imaging holds an important place in the diagnosis. The CT scan is poorly sensitive and in rare cases, hypodensity in the white matter of the posterior territories is observed. MRI is the gold standard and allows a diagnostic approach thanks to the characteristics of the lesions and their distribution. Vasogenic edema is found in the white matter which appears as hyperintense on T2 and FLAIR weighted image, without translation on DWI. The presence of restriction on DWI is in favor of cytotoxic edema and is one of the atypical features found in some cases of PRES. On the other hand, diffusion restriction does not seem to be an argument in favor of the irreversibility of the lesions. 5 In PRES the white matter involvement is bilateral, symmetrical, and predominantly in the parietal and occipital territories. However, as in our case, other parts of the brain may be involved. Thus, the frontal and temporal lobes may be affected, and more rarely the cerebellum and brainstem. 6 The calcarine scissure and the paramedian occipital regions are most often spared. PRES is characterized by the reversibility of the lesions. Thus, the evolution is marked by a regression of the clinical manifestations and the abnormalities on imaging, in case of optimal management. The latter consists of an early diagnosis of the condition followed by the correction of the triggering factors, to which are added various symptomatic treatments such as anticonvulsants. A lack of or delay in management can result in the death of the patient in extreme cases, or in the occurrence of sequelae such as epilepsy or neurological deficits.
Main Circumstances Associated With Posterior Reversible Encephalopathy Syndrome.

Abbreviation: HELLP, hemolysis, elevated liver enzymes, low patelets.
Conclusion
PRES can occur in children. Its diagnosis must be evoked in front of a pattern of acute encephalitis in case of a favorable clinical context. The characteristics of the lesions as well as their distribution are better studied on MRI, which makes it the imaging modality of reference for the diagnosis. The evolution is most often favorable in case of early diagnosis and management.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.