
Abstract
Background. Jaundice is a common problem in the neonatal period, and it is one of multiple factors found in children who die. Despite the majority of pathological jaundice public health consequences, there is no evidence on risk factors of pathological jaundice among neonates in Southwest Ethiopia. Therefore, this study aimed to identify factors associated with jaundice requiring phototherapy management in neonates admitted to the neonatal unit of a university teaching hospital in Southwest Ethiopia (Mizan-Tepi). Methods. Facility-based, unmatched case-control study was conducted among 240 (80 cases and 160 controls) in the Neonatal Intensive Care Unit of Mizan-Tepi University Teaching Hospital. Neonates with pathological jaundice and neonates without pathological jaundice were considered as cases and controls, respectively. Data were collected using a structured questionnaire, and extraction checklist, including information on maternal demographics, obstetrics, and neonatal factors. Simple random sampling techniques were used to select respondents. Bivariate and multivariable analyses were used to examine the association. Finally, statistical significance was declared at a P-value < .05. Results. In this study, 237 mothers with their neonates were included, making a response rate of 98.7%. The mean birth weight of cases and controls was 2330.3 ± 698.9 and 2699.3 ± 686.7 g, respectively. Hypothermia (AOR = 4.28; 95% CI: [1.72-10.67], cesarean delivery (AOR = 4.09; 95% CI: [1.69-9.93]), breast milk feeding (AOR = 2.97; 95% CI: [1.04-8.47]) and being male (AOR = 2.67; 95% CI: [1.17-6.13]) were significantly associated with jaundice. Conclusion. Most of the risk factors of neonatal jaundice were found to be modifiable. Therefore, early prevention and recognition of identified factors are recommended.
Keywords
Introduction
Neonatal jaundice (NJ) is a yellow discoloration of the skin, sclera, and mucosa that results from an excessive accumulation of bilirubin in the neonatal body.1,2 It is one of the most common medical conditions that occurs in up to 60% of term and 80% of preterm newborns. 3 NJ is a preventable and treatable clinical complication, but if left untreated, it can result in neonatal mortality.4,5
Worldwide, NJ affects 1.1 million neonates every year. 6 The burden was highest in low-and middle-income countries in Sub-Saharan Africa and South Asia. 7 Based on the findings of a study in Nigeria, NJ accounted for 35.0% of all NICU admissions. 8 Ethiopia is one of the top 10 countries in jaundice-related neonatal mortality. 9 Studies conducted at the University of Gonder, and Addis Abeba, Ethiopia, showed a prevalence of NJ of 24.6% and 13.3%, respectively.10,11
Maternal risk factors for NJ include diabetes mellitus, ABO, and Rh incompatibilities are the main risk factors of NJ. 12 Low birth weight, sepsis, birth injury, prematurity, glucose-6-phosphate dehydrogenase deficiency (G6PD), polycythemia, male sex, breastfeeding, and family history of jaundice are recognized as independent factors for NJ.12,13
Severe NJ leads to acute bilirubin encephalopathy or kernicterus with a significant risk of neonatal mortality. If an infant survives, they may suffer long-term neurodevelopmental damage, including cerebral palsy, sensory neural hearing loss, intellectual disabilities, seizures, and significant developmental delays.14 -17 In addition, NJ is a risk factor for attention deficit hyperactivity disorder, autism spectrum disorders, asthma, and epilepsy in childhood and later life.18 -20 Moreover, it increases the economic and social burden on families. 7 NJ is also a major cause of hospital readmissions in the Neonatal Intensive Care Unit (NICU) in the first month of life. 21
The Ethiopian Federal Minister of Health (FMOH) has implemented different strategies to improve maternal and neonatal health, including expanding healthcare facilities, increasing skilled health professionals, and increasing the availability of supplies. Even though those actions are taken, the neonatal mortality rate is still 29/1000 live births. 22 Despite the above burden and efforts, there is no research on the determinants of NJ in our study area. In addition, the Ethiopian government targets decreasing the neonatal mortality rate below 11/1000 live births by 2035. 23 To succeed in this plan, data related to the factors associated with NJ is crucial. Therefore, this study aimed to identify factors associated with jaundice requiring phototherapy management in neonates admitted to the neonatal unit of a university teaching hospital in southwest Ethiopia (Mizan-Tepi).
Materials and Methods
Study Design, Setting, and Period
A facility-based, unmatched case-control study was conducted at Mizan-Tepi University Teaching Hospital (MTUTH) from July 2021 to September 2021. It is located in the south-western part of Ethiopia, in a town called Mizan Teferi. Mizan Teferi is located about 565 km from Addis Ababa, the capital city of Ethiopia. The hospital serves around 2.7 million people. The hospital provides emergency obstetric care and has a full maternal and neonatal health infrastructure and skilled health professionals, including neonatologists, obstetricians, anesthesiologists, radiologists, nurses, and midwives. One of the current services offered by this hospital is the NICU. The unit admits about 90 neonates per month on average, and it has 50 beds (30 neonatal beds and 20 kangaroo mother care (KMC) beds). A total of 240 (80 cases and 160 controls) mothers and their newborns participated in the study. To get an adequate number of study participants, both cases and controls were selected using a consecutive sampling technique. For one case, 2 controls were recruited until the allocated sample was achieved in the NICU.
Participants
All mothers with their neonates admitted to the NICU in MTUTH were the source of population, and all mothers with their neonates admitted to the NICU in MTUTH during the study period were the study of population. Cases and controls were neonates with pathological jaundice and without pathological jaundice admitted to the NICU, respectively. Neonates with congenital anomalies and readmitted neonates with the same medical problem during the study period were excluded from the study. Mothers who had an incomplete chart and those mothers who were too critically ill were also excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was calculated by using a double population proportion formula in the EPI Info version 7 statistical software packages by considering a 95% confidence interval (CI), power of 80%, and case-control ratio of 1:2. The previous Ethiopian studies conducted in Addis Ababa, Amhara region, and Mekelle city reported that sepsis, duration of labor, birth weight, and birth asphyxia are significantly associated with NJ. To calculate the sample size, all the above exposure variables were considered. From those variables, birth asphyxia with an adjusted odd ratio (AOR = 2.88), 11% of controls exposed, and 26.3% of cases exposed give the maximum sample size as compared to other exposure variables. 24
The formula for sample size is

where n1 = the sample size required in each group, Zα/2 represented the desired level of statistical significance (1.96) for a 0.05 significance level, r was the ratio of cases to control (1:2), Zβ was the desired study power (typically .84 for 80% power), P was the average proportion in the reference study (18.5%), p1 was the proportion of exposure in the control group in the reference study (11%%), and p2 was the proportion of exposed in the case group in the reference study (26.3%). Accordingly, after adding a 10% non-response rate, the total sample size becomes 240 (160 control and 80 cases).
Operational Definitions
Data Sources and Measurement
Data were collected by interviewing the mother and reviewing medical records of the mother and their neonate using the Amharic version, which is the local language. The structured questionnaire and extraction checklist were adapted from previous literature.11,24,26 -29
An interviewer-administered questionnaire was used to collect information on the mother’s age, religion, marital status, parity, occupation, educational level, place of residence, antenatal (ANC) follow-up, method of feeding the neonate, and its frequency. A checklist was used to extract data from the maternal and neonatal records regarding the sex of the neonate, their age, types of delivery, duration of labor, blood type and Rh status, Rh-, and ABO-incompatibility, birth weight, sepsis, birth trauma, hypothermia, hypoglycemia, meconium aspiration syndrome (MAS), and premature rupture of the membranes (PROM). Additionally, information on gestational age at birth was collected using the checklist from the antenatal follow-up record. When information was not known, evidence of first- or second-trimester ultrasounds was used.
Data Quality Control
Data were collected using questionnaires and checklists that were written in English and translated into the local language, Amharic. Four B.Sc. midwives were trained on the techniques of data collection. The principal researchers were also involved in data collection. A pre-test was done outside the study area among 5% of the total sample size to check the consistency of the tool.
Data Processing and Analysis
The data were cleaned, coded, and entered into EpiData version 3.2 and transferred to SPSS version 25.0 for analysis. The data were expressed in terms of frequency, percentages, and mean. Chi-square (
Results
Socio-Demographic Characteristics
A total of 237 mothers and their neonates (79 cases and 158 controls) were included in the study, making a response rate of 98.7%. The mean birth weight of cases and controls was 2330.3 ± 698.9 g and 2699.3 ± 686.7 g, respectively.
Mothers aged 35 and older had the highest proportion of cases (71.4%) compared with controls (28.6%) (P = .001). However, there were no significant differences between cases and controls in terms of maternal educational status (P = .913), religious affiliation (P = .698), marital status (P = .276), residence (P = .167), and occupation (P = .843) (Table 1).
Comparison of Socio-demographic Characteristics in Cases and Controls.

Obstetrics and Social-Related Characteristics
The proportion of ANC follow-up was lower among cases (29.3%) compared with controls (70.7%) (P = .001). In addition, the proportion of cesarean delivery was higher among cases (54.0%) compared with controls (46.0%) (P = .000). The proportion of term neonates was much lower among cases (13.6%) than in controls (86.4%) (P = .000). However, parity (P = .699), history of abortion (P = .312), time of delivery (P = .373), history of PROM (P = .470), history of multiple pregnancies (P = .335), history of using traditional medicine (P = .582), and cigarette smoking during pregnancy (P = .321) were comparable in the cases and controls group (Table 2).
Comparison of Obstetrics and Social-related Characteristics in Cases and Controls.

Neonatal Characteristics
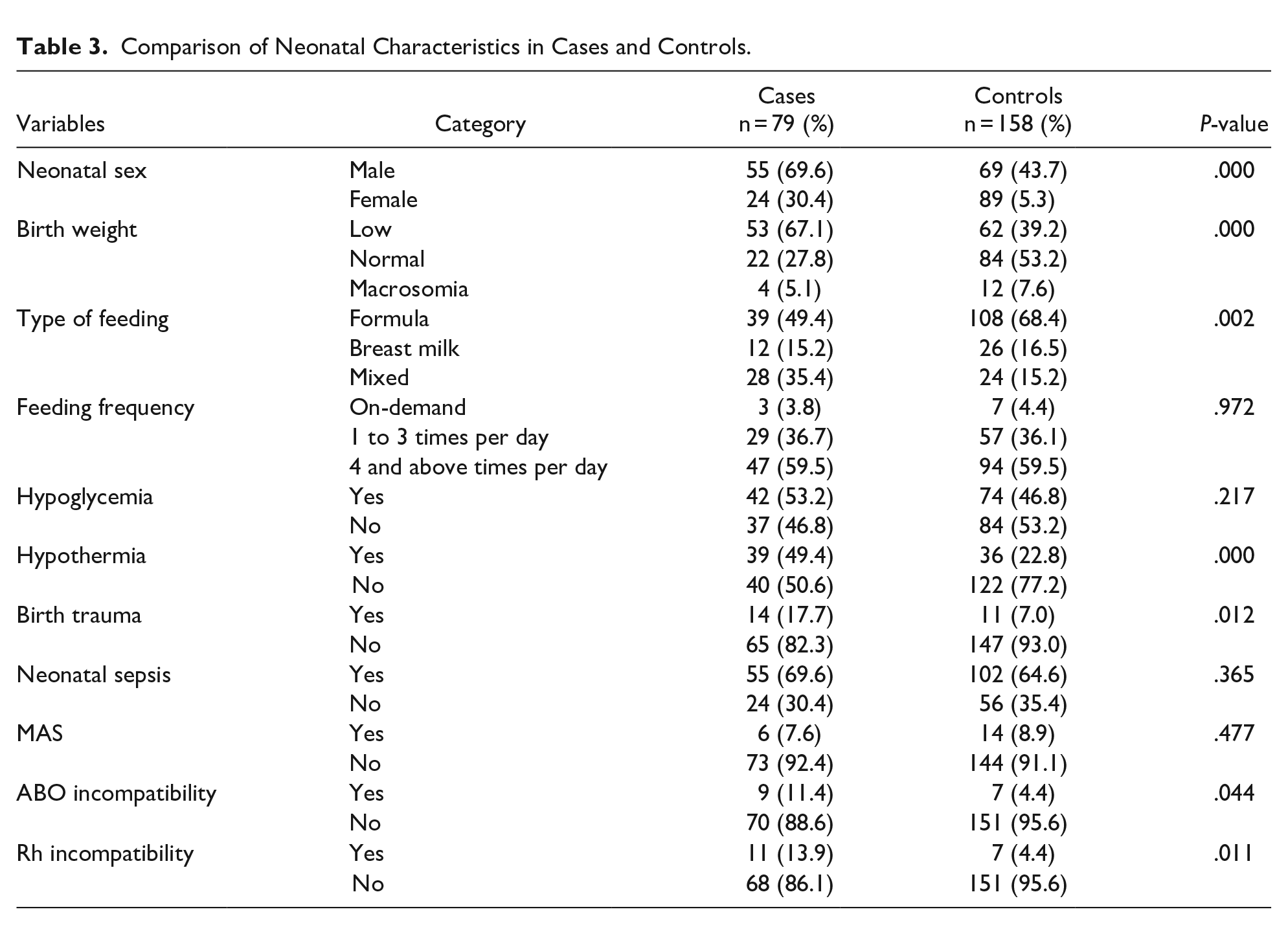
The female sex was much higher for controls (78.8%) than for cases (21.2%) (P = .000). The proportion of hypothermia neonates was much lower among cases (24.7%) compared with controls (75.3%) (P = .000). The proportion of neonates who had breastfed was much lower among cases (26.5%) compared with controls (73.5%) (P = .002). The proportion of neonates who had ABO incompatibility with their mother was also higher for cases (56.3%) than for controls (43.8%) (P = .044). The proportion of neonates who had Rh incompatibility with their mother was also higher for cases (61.1%) than for controls (38.9%) (P = .011). The proportion of normal birth weight was higher among controls (79.2%) compared with cases (20.8%) (P = .000). The proportion of birth injuries was much lower among cases (30.7%) than in controls (69.3%) (P = .012). However, there were no significant differences between cases and control groups in sepsis (P = .365) and meconium aspiration syndrome (P = .477) (Table 3).
Comparison of Neonatal Characteristics in Cases and Controls.
Factors Associated With NJ
In the bivariable logistic regression model, maternal age, ANC follow-up, gestational age, duration of labor, types of delivery, hypothermia, type of feeding, Rh-incompatibility, ABO-incompatibility, birth weight, and sex of the neonate were the risk factors of NJ. After adjusting confounding variables in the multivariable logistic regression model, types of delivery, hypothermia, type of feeding, and sex of the neonate were independent risk factors of NJ.
The odds of NJ were 4.28 times higher among neonates with hypothermia than neonates without hypothermia (AOR = 4.28; 95% CI: [1.72-10.67]. Neonates born from mothers who had a cesarean section during the current pregnancy were 4 times more likely to develop NJ than their counterparts (AOR = 4.09; 95% CI: [1.69-9.93]). The odds of NJ were 2.97 times more likely among breastfeeding neonates than formula-feeding neonates (AOR = 2.97; 95% CI: [1.04-8.47]). The odds of experiencing NJ were higher among male neonates as compared to female neonates (AOR = 2.67; 95% CI: [1.17-6.13]) (Table 4).
Bivariable and Multivariable Analysis of the Risk Factors of NJ.

Abbreviations: COR, crude odd ratio; AOR, adjusted odd ratio; 1, Reference.
Significant at ≤5% level of significant.
Discussions
The commitment to neonatal health issues is necessary for Ethiopia to achieve the Sustainable Development Goals (SDGs). One of the factors contributing to neonatal morbidity and mortality is NJ and its consequences. Our study identified the risk factors of NJ among neonates admitted to the NICU of MTUTH, Southwest Ethiopia.
The most important factor associated with NJ found in our study was hypothermia. In this regard, neonates with hypothermia were 4.2 times more likely to develop NJ than neonates without hypothermia. This was in agreement with a study done in Amhara, Ethiopia. 24 This might be because the cold injury is associated with edema and hemorrhage, which leads to the accumulation of serum bilirubin. In addition, cold injury can lead to increases in pre-glomerular vasoconstriction, thereby causing glomerular filtration rate derangement, which leads to the accumulation of serum bilirubin in the body. 30 Warming the delivery room (25°C and 28°C) before delivery, drying and skin-to-skin contact, and timely initiation of breastfeeding are important to minimize hypothermia. Radiant warmers, incubators, and Kangaroo Mother Care (KMC) are also essential measures to keep the neonate warm. In addition to regulating body temperature, KMC has even more significant advantages, including reducing mortality, increasing weight gain, encouraging breastfeeding, reducing hospital stays, and improving sleep.
It was also found that the types of delivery had a significant effect on the development of NJ. The odds of developing neonatal jaundice among neonates whose mothers had cesarean delivery were 4 times higher compared with those neonates whose mothers had a vaginal delivery. This finding was supported by studies conducted in Malaysia and India.31,32 However, this study was inconsistent with the study done in South Africa found that vaginal delivery was associated with NJ. 33 This might be due to methodological differences, which was a cross-sectional study. A possible reason for the association between NJ and cesarean delivery is the anesthetic effect during the procedure that induced a substantial rise in the total bilirubin levels of neonates. 34 The other possible reason could be a delay in the initiation of breastfeeding after cesarean birth. Even though the WHO recommended that breastfeeding should be started within 1 hour of birth for all newborns, cesarean birth may not be initiated timely because of restricted mobility, the distressful condition of the newborn and mother after cesarean birth, and the physical separation of the newborn from mother during recovery time. When a baby is not getting enough breast milk on time, it leads to increased bilirubin levels.35,36
Another factor that affects NJ is the type of feeding. In this regard, neonates who feed breast milk were 2.9 times more likely to develop NJ as compared to those who use formula feeding. This was in agreement with studies done in Nepal, India, and Nigeria.37 -39 Another study conducted in Tigray, Ethiopia, showed that breast milk increases the risk of NJ. 40 This association is due to the fact that breastfeeding leads to a substantial elevation of bilirubin levels by inhibiting conjugation of bilirubin due to the existence of non-esterified free fatty acids. 41
Last, but not least, the determinant of NJ was the sex of the neonates. In this context, male neonates experienced a high risk of NJ as compared with female neonates. This finding was supported by studies conducted in Iran and Mekelle, Ethiopia.2,42 Although the cause of the sex-related variation in neonatal jaundice is unknown, a study suggested that sex hormones may play a role in regulating bilirubin conjugation. In contrast to males, females have a higher rate of bilirubin elimination and hepatic conjugation.43,44 Additionally, the growth and development of males were lower than those of females. It might therefore be possible that male neonates have a relatively immature liver, which may not be able to process all the bilirubin formed from red blood cells in normal conditions. 45
Limitations of the Study
The study found relevant findings that are crucial for NJ reduction programs. However, we would like to assure our readers that a few limitations need to be taken into account. The research might be subjected to recall bias, since participants might not remember past events. Additionally, some significant variables, such as glucose-6-phosphatase dehydrogenase (G6PD) and thyroid stimulating hormone (TSH), were not assessed due to a lack of resources.
Conclusion
NJ was affected by different factors in the current study. Cesarean delivery, hypothermia, and breast milk feeding were the modifiable risk factors for NJ. But, the sex of the neonate was a non-modifiable factor for NJ. Thus, prevention, early recognition, and treatment of identified modifiable risk factors should be considered to reduce NJ and its subsequent consequences.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X231218193 – Supplemental material for Determinants of Jaundice Among Neonates Admitted to Neonatal Intensive Care Unit of Mizan Tepi University Teaching Hospital, Southwest Ethiopia, 2021: Unmatched Case Control Study
Supplemental material, sj-docx-1-gph-10.1177_2333794X231218193 for Determinants of Jaundice Among Neonates Admitted to Neonatal Intensive Care Unit of Mizan Tepi University Teaching Hospital, Southwest Ethiopia, 2021: Unmatched Case Control Study by Amanuel Adugna and Demekech Ado in Global Pediatric Health
Footnotes
Acknowledgements
The authors are particularly grateful to the staff of the NICU and the medical records department of the hospital for their cooperation during the study. We would like to thank hospital manager, study participants, data collectors, and supervisors for the support of the overall process of the research procedure.
Abbreviations
ANC: Antenatal Care, AOR: Adjusted Odds Ratio, CI: Confidence Interval, COR: Crude Odds Ratio, OR: Odds Ratio, MAS: Meconium Aspiration Syndrome, MTUTH: Mizan-Tepi University Teaching Hospital, NICU: Neonatal Intensive Care Unit, NJ: Neonatal Jaundice, PROM: Premature Rupture of Membranes, Rh: Rhesus, SPSS: Statistical Package for Social Science, WHO: World Health Organization.
Author Contributions
AA; developed the conception of the idea, wrote the proposal, participated in the data collection, analysis writing, and prepared the manuscript. DA; participated in data analysis, and report and participated in manuscript development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Before data collection, ethical clearance was obtained from Mizan-Tepi University, College of Medicine and Health Science, with reference number 051/2021. The participants provided their written consent to participate in this study. Legally authorized representatives of illiterate participants provided informed consent for the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.