
Abstract
Background: Severe neonatal jaundice (NNJ) remains a leading cause of preventable brain damage, mental handicap, physical disabilities, and early death among infants. Methods: Using a descriptive cross-sectional study design, information was gathered using a structured, pretested questionnaire from 518 pregnant women who attended the antenatal clinic at a tertiary Hospital in Southwest Nigeria. Results: Most (77%) of the respondents have heard about NNJ prior the survey. Most respondents (69.5%) demonstrated poor knowledge of the causes of NNJ. The majority, 98.4% had good attitude toward treatment of NNJ. Most respondents (72.1%) demonstrated poor knowledge of the correct treatment of NNJ. A quarter of the respondents knew no danger sign of NNJ. Conclusion: There is serious knowledge gap among the respondents about the causes, treatment, dangers signs and complications of NNJ. There is need for increased awareness campaign using every available means of reaching women of reproductive age group to reduce the consequences of this common neonatal problem.
What do we already know about this topic?
Neonatal Jaundice is a leading reason for neonatal admissions and re-admissions worldwide. Severe NNJ is a known cause of neonatal morbidity, mortality, and life-long disability for the survivors.
How does this research contribute to the field?
This study showed that mothers’ understanding of this common problem is still poor. It further showed that there is need for continued, intense public enlightenment campaign to prevent more children suffering from the complications of this common neonatal problem.
What are the research’s implications toward theory, practice, and policy?
There is need to review the education curriculum to ensure the public is aware of this common problem and the appropriate treatment options.
It is important to ensure that healthcare workers with the requisite knowledge handles health talks during antenatal clinic sessions.
There is also the need to use various media of communication to ensure that the right information is available to women of reproductive age groups. Neonatal healthcare professionals, either as individuals or in groups can make use of social media to give correct information to mothers.
Introduction
Neonatal jaundice (NNJ) is one of the leading reasons for admission into neonatal units worldwide. Jaundice is defined as yellowish discoloration of the white part of the sclera and skin due to excessive bilirubin accumulation. 1 It is seen in as much as 50-60% of term babies after delivery and in about 80% of preterm babies making it a very common condition in neonatal life.1-3 Though a common neonatal condition, NNJ is a known reason for hospital admission and re-admission in neonatal period. It is a known cause of both short-term and long-term complications in neonates who unfortunately develop the severe form of the condition. Jaundice can either be conjugated, unconjugated or a mixture of the two. 2 Complications can arise because of excessive accumulation of either unconjugated or conjugated bilirubin in newborns, however most of the complications follow unconjugated hyperbilirubinaemia. Severe neonatal jaundice remains a leading cause of preventable brain damage, mental handicap, physical disabilities, and early death among infants.2,4-9
Jaundice is seen more in the neonatal period due to higher rates of bilirubin production resulting from physiological factors like higher red cell mass at birth, shorter red blood cells life span, inadequate calorie intake which results in increased enterohepatic circulation, low albumin level and an underdeveloped bilirubin conjugating system.2,6,10
Risk factors for significant hyperbilirubinemia include ABO blood incompatibility, sepsis, glucose-6-phosphate dehydrogenase deficiency (G6PD deficiency), Rhesus iso-immunization, prematurity, cephalhematoma and positive Coombs test.2,11,12 Others include inadequate breastfeeding, breastmilk jaundice, maternal diabetes, oriental race, short gestation, male sex, and induction of labor with oxytocin.2,11,12
The precise blood level above which unconjugated bilirubin will be toxic for an individual infant is unpredictable. 3 However, high incidence of acute bilirubin encephalopathy (ABE) is associated with serum bilirubin levels in excess of 20 mg/dl in normal birth weight babies who are otherwise healthy. 13 Some studies have documented mild neurological damage from even moderate neonatal hyperbilirubinaemia. 14 Most times, these neurological sequelae manifest later in life. 14 There is no cure for the chronic findings associated with Kernicterus Spectrum Disorders (KSDs), 15 but they are preventable if NNJ is recognized early and effective therapy commenced promptly. 13
Aside from being a known cause of neonatal mortality, acute bilirubin encephalopathy (ABE) results in chronic handicapping conditions such as cerebral palsy, deafness, speech disorders, learning disabilities and mental retardation.2,4-6,8-10 Some studies have shown that severe neonatal jaundice with ABE contributed to about 50% of all cases of cerebral palsy.4,16,17
Studies conducted in Nigeria have shown neonatal jaundice to be one of the leading reasons for referral to tertiary health facilities for care.5,18-20 However a good proportion of the babies were brought in late with ABE, the most feared complication of severe NNJ. 21
The affected babies are brought late to the appropriate healthcare facilities probably because most mothers and caregivers have poor understanding of the causes of NNJ, its detection, management, and complications coupled with the mismanagement of this common neonatal problem by the general populace.1,20,22,23 Unfortunately, on some occasions when NNJ is noticed early by the mother or close relatives, ineffective medications and treatment options are offered the mothers sometimes by friends, other relatives, concerned neighbors and sometimes by “healthcare workers” with poor knowledge of neonatal jaundice and its management.
Previous studies on NNJ in Nigeria reported a poor knowledge about its causes, management and complications among pregnant women.3,24-26 For instance, about 80% of participants in a study conducted by Ezeaka et al. 25 in Lagos (an urban center city in Nigeria) did not know the causes of NNJ and only 9.5% of them identified phototherapy as a treatment option. Also, only 56.6% of pregnant women studied by Ogunfowora et al. 3 could correctly check for jaundice, just 50.3% of them knew at least a danger sign of severe NNJ and 14.8% would use extract of unripe papaya for its treatment. These studies showed great knowledge gap among expectant mothers in Nigeria. It is expected that the advent of the internet and social media should increase the knowledge of pregnant women about NNJ. It remains to be seen if this holds true among pregnant women in Nigeria. The high incidence of unwholesome practices like absence of skilled birth attendants at delivery, delivery outside healthcare facilities, early hospital discharge post-delivery and poor post-delivery follow-up 27 further emphasizes the need for mothers and other caregivers of newborn babies to possess basic knowledge about the causes, identification, treatment and complications attributable to neonatal jaundice. The multicenter study conducted by Wennberg et al. 28 revealed that providing information to mothers about NNJ was associated with a reduction in the incidence of bilirubin encephalopathy.
This study was conducted to determine the level of understanding of neonatal jaundice among expectant mothers attending antenatal care at a tertiary healthcare facility in Ekiti State, Southwest Nigeria. The study is also expected to identify knowledge gaps about NNJ among expectant mothers and how to address the identified gaps. The outcome of this study is expected to guide healthcare professionals and policy makers to decide on appropriate method of information dissemination and the need for increased awareness campaign about NNJ among women of reproductive age group in the State.
Methods
Study Setting
The study was conducted at the antenatal clinic of the Obstetrics and Gynaecology (O&G) Department of a tertiary hospital in South-West Nigeria. This tertiary level healthcare facility provides medical care including maternal and child health services to the people of Ekiti State and some border towns in the neighboring States of Ondo, Kogi and Kwara States. The Obstetrics and Gynaecology Department of the institution is well staffed with its components of interns, Registrars, Senior registrars, Consultants and Nursing staffs who run a twice weekly antenatal clinic where pregnant women are attended to.
Study Design
The study was a descriptive cross-sectional study conducted at a tertiary hospital in Southwest Nigeria between April and July 2019.
Study Population
The study population were pregnant women who attended the antenatal clinic of the institution during the study period. The women were first given information about the study and those who gave consent to participate were given the questionnaire to complete. Any participant who had filled the questionnaire once was prevented from filling the second time. This was done to prevent multiple/duplicate responses or entries from any participant.
Data Collection
This was done using a structured, pretested questionnaire administered by trained nurses in the antenatal clinic and medical interns. Qualitative information was sought on socio-demographic characteristics of the participants. Additionally, their knowledge, attitude, and practice with regards to detection, causes or risk factors, treatment options and complications of severe NNJ were obtained.
The first section of the questionnaire included biodata, sociodemographic data, highest level of formal education attained, and obstetric data of respondents.
The next section of the data collection tool assessed the knowledge of the mothers on the detection, possible causes, treatment modalities, and complications of neonatal jaundice using both closed- and open-ended multiple-choice questions.
Respondents’ answers to questions on their perceived causes of NNJ were graded as correct and incorrect and the total score of the correct answers were used to categorize respondents’ knowledge as follows: Poor Knowledge (0-3 correct answers), Good Knowledge (4-6 correct answers), and Very Good Knowledge (7-9 correct answers). There were 5 correct answers among the options listed when assessing the respondents’ knowledge of the management of NNJ and the correct responses were graded as follows: Poor knowledge (0-2 correct options), Good knowledge (3 correct options) and Very Good knowledge (4-5 correct options).
Participants were discouraged from communicating with one another while completing the questionnaire. The participants were however allowed to seek clarification from the personnel who administered the questionnaire.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Research and Ethics Committee of the Ekiti State University Teaching Hospital (EKSUTH) prior the commencement of the study with approval number EKSUTH/A67/2019/04/0011.
All the participants provided written informed consent prior to enrolment in the study.
Statistical Analysis
Data obtained were entered into a personal computer and was cleaned. Descriptive data analysis was done using SPSS version 25. Results were expressed as means, frequencies, and percentages. Chi-square statistical test and Fisher’s exact test were used to test association between the socio-demographic characteristics of the respondents and their knowledge and attitude toward NNJ. The level of significance was set at P < .05 and confidence level at 95%.
Result
Five hundred and eighteen (518) pregnant women participated in the study. The mean age of the respondents was 29.7 years, with about half of them (50.8%) within the age range 21 to 30 years. Eighty eight percent (88%) of the study participants had tertiary education. Twenty eight percent of them (28.4%) had been pregnant once before this study, while 25.7% were carrying their first pregnancy. The other sociodemographic characteristics of the participants are shown in Table 1.
The Socio-Demographic Characteristics of the Respondents.

Seventy seven percent of the respondents have heard about neonatal jaundice prior the survey, 2.5% were not sure if they have heard about it before, 15.6% of the respondents claimed not to have heard about neonatal jaundice before the survey while 4.1% did not respond to the question.
Few of the study participants (10.4%) have had babies with neonatal jaundice in the past, 83.4% of the respondents have not had any baby with noticeable jaundice prior this study while 6.2% did not respond to this question.
About 7% of the respondents have had only 1 baby with jaundice prior this study, 1.5% have had 2 babies with jaundice prior this study while 0.6% of the respondents have had 3 babies with jaundice previously.
Seventy nine percent (79%) of the respondents will check the eyes of the newborn for jaundice, 40.9% the baby’s skin, 17.8% will check for jaundice inside the baby’s mouth while 21.2% of them will check for jaundice on the baby’s abdomen.
Regarding the knowledge of the causes of neonatal jaundice, 54.2% of the respondents attributed NNJ to yellow fever, 52.9% attributed it to malaria in pregnancy, 26.4% believe that wearing yellow clothes for the baby could cause NNJ while 42.5%, 33.0%, and 31.7% correctly attributed it to infection in the baby, use of icterogenic agents and blood group disparity between the mother and the baby respectively. Other causes mentioned by the participants are shown in Table 2.
Causes of Jaundice.

Multiple responses were allowed.
As high as 98.3% of the respondents agreed that a baby with jaundice should be taken to the hospital for treatment, 1 respondent (0.2%) suggested a church while 1.5% of the participants did not respond to the question.
When asked about the time of presentation in the hospital for treatment, 65.2% of the respondents agreed that the baby should be taken to the hospital within 24 hours of noticing the jaundice, 3.9% would wait till 7 days or more before presenting at the hospital while 28.8% of the respondents do not know when to take a baby with jaundice to the hospital (Figure 1).
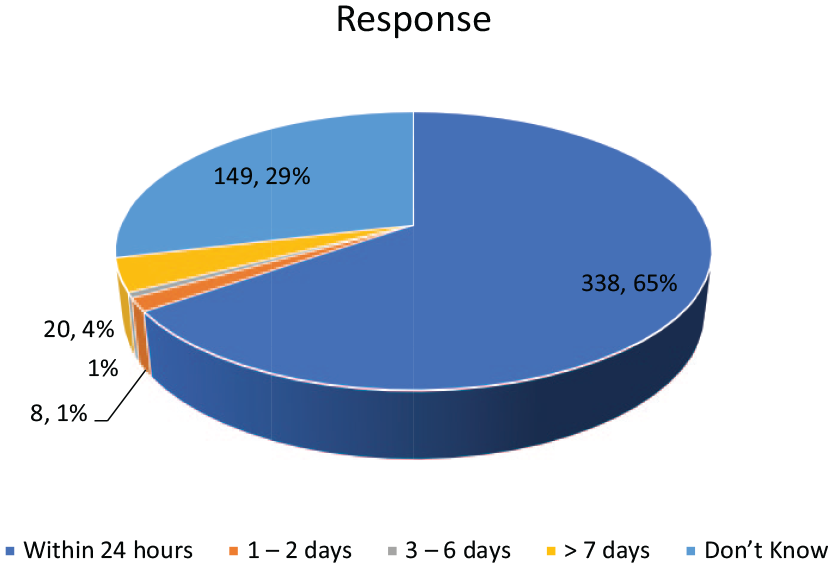
Likely time of presentation in hospital for NNJ.
On the treatment of a baby with jaundice, 36.5% of the respondents chose breastfeeding, 34.9% will expose the baby to sunlight, 27.8% of the respondents will give glucose water to the baby, 15.7% will give Ampiclox syrup, 29.2% will use phototherapy, 0.2% chose surgery. Other treatment options suggested by the respondents are shown in Figure 2.

Treatment of neonatal jaundice (NNJ).
Regarding danger signs in a newborn baby with jaundice, 38.4% and 37.3% of the respondents correctly chose either or both poor suck and high pitched cry respectively as danger signs, however 25.1% of the respondents do not know any danger sign of NNJ (Figure 3).

Respondents’ perceived danger signs of NNJ.
About the complications of NNJ, 39.2% agreed that jaundice could cause brain damage, 26.4% agreed that physical handicap could complicate NNJ, 25.3% chose deafness while 29.3% of the respondents do not know the complications that can result from NNJ (Table 3).
Complications of Jaundice.

Seventy three percent of the respondents believe that NNJ is preventable, 3.3% claim it cannot be prevented while 23.7% do not know if NNJ is preventable.
Seventy seven percent (77%) of the respondents claim that bringing the baby to the hospital for regular checkup is a way to prevent NNJ, 69.5% chose checking the eyes of the baby every day after delivery while 22.4% believe that giving the baby ampiclox syrup® can prevent NNJ (Table 4).
Prevention of NNJ.

Respondents were asked about their sources of information on NNJ, 52.1% of them got their information from the hospital, 23.1% got their information from fellow pregnant women while 11.8% got their information from relatives especially the grandmothers (Figure 4).

Sources of information.
A cross-tabulation of the respondents’ sources of information and a few socio-demographic characteristics and their knowledge of the causes of NNJ was done (Table 5); it was observed that there was a statistically significant association between the knowledge of the causes of NNJ and those who got their information from the hospital (P = 0.000), the respondents age and level of education had no effect on their knowledge of the causes of NNJ, also having a baby with NNJ previously had no effect on their knowledge of the causes of NNJ.
Sources of Information and Socio-Demographic Characteristics of Respondents and Knowledge of the Cause of NNJ.

The significant p-value is in bold font..
The highest level of formal education of the participants was compared with their knowledge of the danger signs of severe neonatal jaundice. It was observed that formal education did not have significant effect on the participants’ knowledge of the danger signs of NNJ as none of the findings was statistically significant (Table 6).
Knowledge of Danger Signs Compared with Highest Level of Formal Education.

Abbreviations: PRY, Primary level; SEC, Secondary level; TERT, Tertiary level; PG, Postgraduate; n, N, number of participants; Abn, Abnormal.
Another cross-tabulation of the socio-demographic characteristics and sources of information of the respondents and their knowledge of various modes of treatment of NNJ was evaluated; there was a statistically significant association between the knowledge of the treatment of NNJ and those who got their information from books/literature (P = 0.000), hospitals (P = 0.000) and the media (P = 0.003); the respondents age and level of education had no effect on their knowledge of the treatment of NNJ, also having a baby with NNJ previously had no effect on their knowledge of the treatment of NNJ(Table 7).
Sources of Information and Socio-Demographic Characteristics of Respondents and Knowledge of the Treatment of Neonatal Jaundice.

The significant p-values are in bold font.
Discussion
A large percentage (77.8%) of the respondents in this study have heard about neonatal jaundice (NNJ) prior their participation in this study. The level of awareness about NNJ is however slightly lower compared to 85.9% reported by Egube et al. 24 in Benin City, 88.2% by Eneh and Ugwu 29 in Port Harcourt and 100% reported by Ogunfowora et al. 3 sixteen years ago in another Southwestern State in Nigeria.
The study however showed that a lot of health education about NNJ still needs to be done even though 88.4% of the respondents had tertiary education.
Despite the seemingly high level of awareness about NNJ, most of the respondents demonstrated poor knowledge of the causes, treatment, danger signs and complications of NNJ. A small proportion (10.4%) of the respondents in this study have had a child with NNJ in the past which is comparable to 12.4% reported by Egube et al. 24 in their study among expectant mothers in Benin City. The knowledge of the respondents on where to check for jaundice is adequate as 70.8% of the respondents agreed to look at the eyes of the baby. This finding is comparable with the 77.4% reported by Egube et al. 24 in Benin City. The knowledge seems good, but the concern is whether it translates to practice among mothers.
The respondents’ knowledge about the causes of NNJ was however poor as more than half of the respondents wrongly chose yellow fever as a cause of NNJ. This observation is far higher than 0.8% reported by Ezeaka et al. 25 among the participants in the study conducted in Lagos by who believed yellow fever is a cause of NNJ. Malaria in pregnancy, wearing of yellow clothes and maternal use of folic acid in pregnancy were also incorrectly chosen as causes of NNJ despite the fact that several authors in Nigeria have reported blood group incompatibility, prematurity, infections and glucose-6-phosphate dehydrogenase deficiency as common aetiological factors of NNJ.9,10 This further affirms the poor knowledge of the mothers.
Less than half of the participants correctly identified infection in the baby, use of icterogenic agents and disparity in the blood group of mother and baby as causes of NNJ. About a tenth of the respondents in this study do not know a cause of NNJ which is quite lower than 75% reported from the study done among pregnant women in Lagos. 25 This finding also shows that mothers who are mostly the primary caregivers of the babies are deficient in the knowledge of the causes of NNJ and this may hinder them from taking the necessary preventive measures. This finding also shows that there is need for massive awareness campaigns in the community about the causes of NNJ if we want to win the battle against severe NNJ.
This study demonstrated correct knowledge among the majority of participants regarding the treatment of NNJ which is in keeping with the findings of Egube et al. 24 in Benin city. This can be leveraged upon with appropriate counsel to further encourage mothers to do the right thing at the right time.
Close to two thirds of the respondents believed that babies with jaundice should be taken to the hospital within 24 hours of onset, this finding is however in contrast with what happens in practice as reported by Ibekwe et al. 30 in Abakaliki where mothers presented at about 48 hours after onset of jaundice. The study done by Owa and Ogunlesi 23 in Ilesa, reported that 26 of the 27 babies with ABE had developed the complication before presenting in the hospital also suggesting late presentation. A relatively high proportion (28.8%) of participants in this study did not know when a baby with jaundice should be taken to the hospital and this high number may be one of the reasons why some mothers present late for treatment. Thus, there is need to persuade and encourage mothers to present their babies on time for appropriate treatment in the hospital to prevent irreversible brain damage.
The knowledge of the participants with regards to the treatment of neonatal jaundice is also worrisome as more than a third chose exposure to sunlight and close to a third will give glucose water as treatment for NNJ. These findings are comparable to earlier reports from Lagos by Ezeaka et al. 25 in which the participants chose glucose water, exposure to sunlight and administration of herbal concoctions as treatment for NNJ. About 15% of the respondents will administer ampiclox® syrup as treatment for NNJ, this is appreciably lower than about 50% reported by Ezeaka et al. 25 in Lagos; this could probably be due to availability of appropriate information. These ineffective treatment options are commonly practiced by mothers thus contributing to delay in seeking appropriate treatment for NNJ. Unfortunately, some of these ineffective and deceptive treatment are also sometimes prescribed by health workers at primary health centers as revealed by the study done by Ogunfowora et al. 3 more than 2 decades ago; Findings from this study suggest that this ugly practice could still be happening till date because more than half of the respondents claim to have received their information from hospital. However, it is important to note that specially filtered sunlight phototherapy using available window coloring which sieves out the undesired and dangerous infrared and ultraviolet rays in sunlight has been developed and proven to be effective and safe like the conventional phototherapy. 31 This is good for low resource setting where availability and delivery of effective phototherapy is hindered by poor electricity supply or frequent power outage. 26
More than a third of the respondents in this study chose breastfeeding as a treatment option for NNJ while close to a third chose phototherapy as treatment for NNJ and this is comparable to 25% reported by Khalesi and Rakhshani 32 in Iran over a decade ago. The finding is however lower than 40.4% reported by the study done in Benin City 24 5 years ago. Exchange blood transfusion was chosen as a treatment for NNJ by 27.2% of the participants which is comparable to 26.2% reported by Egube et al. 24 in Benin City. This finding is however higher than 6% reported by Onyearugha et al. 26 in Abakaliki. Less than a fifth of the respondents in this study do not know any form of treatment for NNJ as against 28.3% reported by the study in Benin City. 24 These findings show that there has not been appreciable improvement in the mothers’ knowledge about treatment of NNJ. Nevertheless, it is noteworthy to say that 2 (0.4%) of the participants knew that surgery (treatment modality for biliary atresia and intestinal obstruction) could be a modality of treatment for NNJ caused by biliary atresia or intestinal obstruction.
This study also revealed that the participants’ knowledge of the danger signs of NNJ was poor and this is similar to reports from previous studies20,24,26 as just a little above one-third of the respondents identified brain damage as a complication of severe NNJ. Other complications listed were identified by less than a third of the participants. This also shows poor knowledge of the complications of severe NNJ. This finding is not different from that of Ezeaka et al. 25 in Lagos where only a quarter of the respondents were able to identify the complications of NNJ. Another major gap revealed by this study is that about a third of the respondents did not know any complication of severe NNJ. Having pregnant women who do not know any complication of severe NNJ is not an encouraging finding, further strengthening the need for continued aggressive community education and sensitization on NNJ and its possible untoward sequalae if not effectively managed.
Close to three quarter of the study participants knew that severe NNJ can be prevented, more than a fifth do not know that severe NNJ can be prevented while 3.3% claimed severe NNJ cannot be prevented. This also demonstrates poor understanding of the condition. More than two third of the participants claimed that severe NNJ can be prevented by taking the baby to the hospital for regular check-ups and by checking the eyes of the baby every day after delivery. More than a fifth of the participants believed that administration of ampiclox® syrup to the baby can prevent severe NNJ, this further demonstrates poor knowledge of NNJ by some of the participants.
More than half of the study participants claimed to have acquired their knowledge of NNJ from healthcare facility/hospitals. A major source of information for women or expectant mothers about newborn care is health talks given during antenatal clinic, childhood immunization or infant welfare clinic visits. The findings of poor knowledge of the causes, danger signs, treatments and complications of severe NNJ in this study probably reflect either poor communication skills by those who give the health talks or poor knowledge on the part of those giving the health talks in the health care facilities. It has been documented that significant proportion of healthcare workers on occasions display inadequate knowledge of certain aspects of health issues and therefore can give inadequate information to antenatal attendees. 1 Thus, there may be the need for training and retraining of the healthcare workers who give health talks during antenatal clinic or immunization sessions on appropriate delivery of health information to mothers and training to deepen their understanding of the subject matter. Also, the fact that some respondents claimed they got their information from the media and some books/literatures raises the need for healthcare professionals to make good use of these avenues especially the print and electronic media (social media inclusive) to provide qualitative and reliable information to their clients and larger community on NNJ and other common childhood illnesses or diseases. It is also important to sound a note of warning to expectant mothers and mothers generally to censor their sources of information so as not to make the wrong choice for their babies because of uncontrolled advertisement of “magic treatments” on social media.
This study revealed that the level of education of the participants did not confer any advantage on their knowledge of the causes, the danger signs and treatment of NNJ and this is a sad finding in the twenty-first century. This probably suggests that the current education system needs to be improved on so as to improve mothers’ quest for appropriate knowledge about common illnesses thereby improving their healthcare seeking behavior.
Inadequate knowledge of the causes, danger signs, treatment options and complications of NNJ among pregnant women puts them at a very high risk of missing some avoidable predisposing factors and even signs that will demand immediate presentation in the hospital for adequate management of babies with jaundice. This delay puts the newborn baby at risk of developing severe forms of NNJ and its most feared complication of bilirubin encephalopathy before presenting at the appropriate facility for management. Adequate knowledge of this preventable irreversible chronic handicapping and disabling complications of NNJ by pregnant women and women of reproductive age group generally will likely increase the mothers’ healthcare seeking behavior with regards to NNJ to avert those complications. 26
Conclusion
The majority of the respondents in this study demonstrated poor knowledge of the causes, danger signs, treatment, and complications of NNJ. There is a need for serious public enlightenment campaigns about NNJ and other childhood diseases generally highlighting the risk factors, causes, appropriate treatment options, danger signs, complications, and preventive measures. There is also the need for healthcare workers at all levels to be appropriately trained about common childhood diseases. Also, it is also imperative to train healthcare workers about effective communication skills to ensure appropriate dissemination of information to the clients whenever they have contact with healthcare personnel.
Limitations
The study did not assess the content of the education received by the participants prior the survey. There is also the challenge of missing data (non-response to some questions). Nonetheless, this study provides information on the knowledge and perception of NNJ by pregnant women.
Footnotes
Acknowledgements
The authors appreciate the Obstetricians who allowed us to use their patients; all the nurses working in the antenatal clinic of our institution and the interns who assisted in data collection. We deeply appreciate all the expectant mothers who participated in the study. We also appreciate the people who assisted with data entry.
Author Contributions
The study was conceived and designed by OEO together with AOT and FOA. OEO, TAB and AOT collected the data. OAC, FOA and OEO analyzed the data. OEO wrote the initial draft. BAO, AAB, AAT, OAC, FOA, OOA, OIO, OOS critically reviewed the manuscript. All authors read and approved the final draft of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was obtained from the Ethics and Research Committees of the tertiary hospital in Southwest Nigeria. The approval number is EKSUTH/A67/2019/04/0011.