
Abstract
Introduction:
Low birth weight (LBW) is a significant global health issue. While previous studies in Ethiopia have focused on single institutions or urban areas, this research aims to assess LBW prevalence and its risk factors among newborns in public hospitals in the Sidama Region.
Methods:
A cross-sectional study was conducted from January 10 to March 10, 2024, involving 380 women selected via systematic random sampling. Data were collected using a structured questionnaire, and associations were analyzed through bi-variable and multivariable logistic regression, with statistical significance set at P < .05.
Results:
The prevalence of LBW was 12.4% (95% CI: 8.8%, 15.8%). Significant risk factors included maternal age (15-19 years, AOR = 11.9), residence (AOR = 12.45), gestational age < 37 weeks (AOR = 4.01), and maternal mid-upper arm circumference (AOR = 5.519).
Conclusion:
The study aligns with national findings, highlighting the need for early detection and management of preterm births and addressing nutritional and social factors.
Introduction
According to the World Health Organization (WHO), low birth weight (LBW) is defined as a birth weight of less than 2.5 kg, regardless of gestational age. 1 LBW is a critical determinant of a newborn’s likelihood of survival and healthy growth and development. 2 Additionally, it predisposes infants to numerous health complications, including underweight, stunting, hypoglycemia, hypothermia, cognitive impairments, and physical and neurological developmental delays, which contribute to elevated morbidity and mortality rates.2 -4 Beyond being a major predictor of perinatal mortality and morbidity, recent studies have also linked LBW to an increased risk of non-communicable diseases such as diabetes and cardiovascular disorders later in life. Furthermore, LBW reflects both the past and current health status of the mother.4,5
LBW remains a critical public health concern worldwide, with significant short- and long-term implications. 6 In the short term, LBW infants are at increased risk of complications such as respiratory distress syndrome, infections, enterocolitis, hydrocephalus, and developmental delays. Long-term consequences may include coronary heart disease, non-insulin-dependent diabetes, childhood hypertension, behavioral disorders, impaired cognitive function, and psychological issues. 7
Globally, LBW affects an estimated 15% to 20% of all births, with over 95% of these cases occurring in low- and middle-income countries. 8 In sub-Saharan Africa, the prevalence of LBW is approximately 15%. 9 Furthermore, studies indicate that preterm and small-for-gestational-age births account for about 52% of neonatal deaths. 10 Infants with a birth weight below 2500 g are approximately 20 times more likely to experience mortality compared to infants with a birth weight within normal range. 11
Previous studies have identified several factors contributing to LBW, including insufficient weight gain during pregnancy, low pre-pregnancy weight, short stature, malaria and other infectious diseases, strenuous physical labor during pregnancy, and social factors such as lower status of women, malnutrition, and inadequate antenatal care.12,13 Furthermore, factors such as lack of antenatal follow-up, preterm delivery, chronic medical illnesses, lack of formal education, maternal age, and iron/folic acid supplementation have been associated with low birth weight in various studies.14,15
Recognizing LBW as a significant public health concern, the Ethiopian government has implemented various interventions to address it, including focused antenatal care, nutritional counseling during the prenatal and perinatal periods, and the promotion of institutional deliveries. 16 Despite these efforts, the rate of newborn deaths remains high.6,7 Regional data show that the prevalence of LBW varies considerably: 13.06% in Addis Ababa, 17 26.3% in Gojam, 18 34.1% in Dilla Town, 19 and 16.5% in the Sidama Region. 20
Although several studies have been conducted in different parts of Ethiopia, most have been limited to a single institution, small settings, and urban populations. This focus may underestimate the impact of potential risk factors on rural communities. Conducting research in broader settings will provide valuable information for policymakers to design interventions and develop more effective health policies, ultimately helping to reduce neonatal mortality. Additionally, in developing countries like Ethiopia, LBW data is limited due to many deliveries occurring at home or in smaller health facilities where cases may go unreported. So, the findings of this study will offer crucial insights and more accurate estimates that is essential for effective interventions and improving newborn health.
Therefore, this study aims to assess the prevalence of low birth weight and its associated factors among newborns delivered in public hospitals in the Sidama Regional State of Ethiopia.
Materials and Methods
Study Setting and Period
The study was conducted from January 10 to March 10, 2024, in selected public general hospitals within the Sidama National Regional State. Located 272 km southeast of Addis Ababa, Ethiopia’s capital, the region has a population exceeding 4 million. It is divided into 4 zones: Northern, Southern, Central, and Eastern. It comprises 30 districts and 6 town administrations. Sidama is bordered to the south by the Oromia region, except for a small border with the Gedio Zone; to the west by the Bilate River, which separates it from the Wolaita Zone; and to the east and north by Oromia. The healthcare infrastructure includes 1 specialized referral teaching hospital, 4 general hospitals, 126 health centers, 531 health posts, 24 medium clinics, 83 primary clinics, and 7 NGO clinics. 21
Study Design, and Population
A facility-based, cross-sectional study design was employed. The source population included all mothers of newborns delivered in public general hospitals within the Sidama National Regional State during the study period. The study population consisted of mothers who delivered in selected public hospitals in the Sidama region, met the eligibility criteria, and had resided in the study area for at least 6 months. Mothers were excluded if they were temporary residents of less than six months, were seriously ill during the study period, or did not have early ultrasound examinations to confirm gestational age.
Sample Size Determination and Sampling Procedures
The required sample size was calculated using a single population proportion formula, based on the following assumptions: a 34.1% prevalence of low birth weight from a previous study, 19 a 95% confidence interval, a 5% margin of error, and a 10% allowance for non-response. With these parameters, the initial sample size was 345. After adjusting for the 10% non-response rate, the final sample size was set at 380. Six hospitals were selected from 21 public hospitals using a simple random sampling (lottery) method. Study subjects were allocated to each hospital proportionally based on the number of deliveries. Participants were then selected using a systematic sampling technique.
Data Collection Tools and Procedures
The standardized questionnaire was adapted from previous similar studies (20, 45). Data were collected using a structured, pretested, interviewer-administered questionnaire. The questionnaire was first translated into Amharic and then back-translated into English to ensure consistency. Six BSc midwives served as data collectors, and 3 Health Officers, fluent in the local languages, acted as supervisors.
Data Quality Control
Data collectors and supervisors received a 1-day training session from the principal investigator. The training covered sampling procedures, techniques for approaching participants during interviews, inclusion and exclusion criteria, proper use of the data collection tool, maintenance of confidentiality, and ensuring participants understood their right to decline participation. Practical role-playing exercises supplemented the training. The questionnaire was pre-tested on 5% of the sample size of mothers to assess completeness, clarity, length, and skip patterns. This pre-test was conducted in a separate health facility not included in the study. A standard baby weighing scale, graded in grams, was used by data collectors to measure the nude weight of each baby within 1 hour of delivery. The principal investigator checked the weighing scales daily, and data collectors verified measurements and adjusted the scales to 0 as needed.
Data Processing and Analysis
Data were collected using Kobo Toolbox and downloaded as Excel files, then exported to SPSS version 26 for analysis. Descriptive statistics, such as frequency distributions, were computed for socio-demographic and other key variables. Binary logistic regression was performed, and variables with a P-value < .25 were entered into the multivariable logistic regression model to control for confounders. Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were reported. A P-value < .05 was considered statistically significant. Model fit was assessed using R-square, with values ≥ 0.1 (10%) indicating acceptable fit, and the Hosmer–Lemeshow goodness-of-fit test. Multicollinearity was evaluated using tolerance and variance inflation factor (VIF). Results were presented in tables, text, frequencies, and figures.
Variables
The outcome variable for this study is Low birth weight. The independent variables were socio-demographic, obstetric/reproductive, health service-related, maternal life style, and nutritional related characteristics of the study participants.
Operational Definitions
Low birth weight: A new born with weight less than 2500 g will Considered as low birth weight irrespective of gestational age. 1
Pre term birth: Gestational age less than 37 weeks from last normal menstrual period or early ultrasound. 22
Term birth: Gestational age greater than 37 weeks from last normal menstrual period or early ultrasound. 22
Ethical Approval and Informed Consent
Ethical approval was obtained from the Institutional Review Board of Yirgalem Hospital Medical College (Reference Number YHMC/IRB001). Additionally, consent letters were secured from selected General Hospitals before interviewing study participants.
Before commencing data collection, the researchers ensured that participants provided verbal informed consent, which included a full disclosure of the study’s purpose, benefits, and potential risks. Participants were informed of their right to withdraw from the interview at any time and were assured that their responses would remain confidential.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 380 respondents participated in this study, achieving a 100% response rate. Approximately half of the respondents, 195 (51.3%), were aged between 25 and 29 years, with a mean age of 25.2 years (±4.17 SD). Most women, 375 (98.7%), were currently married. Nearly half of the respondents, 191 (50.3%), resided in urban areas. Regarding education, 168 (44.2%) of the respondents had not attended formal schooling, while 159 (41.8%) of their husbands also lacked formal education. In terms of occupation, 281 (73.9%) of the women were housewives, followed by 47 (12.4%) who were government employees. The most common occupation among husbands was merchant, accounting for 40.8% (Table 1).
Socio-Demographic Characteristics of Study Participants in Public Hospitals of Sidama National Regional State, Ethiopia, 2024.

Single, divorced or windowed.
Student.
Obstetric and Health Services Related Characteristics of Study Participants
More than two-thirds of the mothers, 289 (76.1%), delivered their neonates at or beyond 37 weeks of gestation, with a mean gestational age of 37.97 ± 1.74 weeks. Among the participants, 263 (69.2%) were multiparous. One hundred and thirty (34.2%) mothers had a pregnancy interval exceeding 2 years between their current and previous pregnancies. Antenatal care (ANC) visits were reported by 313 (82.4%) mothers, with 273 (71.8%) attending 4 or more visits. Iron supplementation was taken by 307 (80.8%) respondents, and over half, 208 (54.7%), took iron tablets for more than 60 days. Dietary counseling was provided to 313 (82.4%) mothers during their current pregnancy, and 293 (77.1%) reported consuming extra meals. Most mothers, 331 (87.1%), did not develop pregnancy-induced hypertension, and the vast majority, 376 (98.9%), had no history of delivering small babies (Table 2).
Obstetric and Health Service Characteristics of Study Participants in Public Hospitals of Sidama National Regional State, Ethiopia, 2024.

Maternal Anthropometric and Life Style Characteristics
The majority of mothers, 319 (83.4%), were taller than 150 cm. Nearly half, 192 (50.5%), had a mid-upper arm circumference (MUAC) below 23 cm. Most respondents, 326 (85.8%), had a body mass index (BMI) within the normal range of 18.5 to 24.99 kg/m2. During the current pregnancy, 11 (2.9%) mothers reported consuming alcoholic beverages such as beer, wine, while 369 (97.1%) abstained from alcohol. None of the respondents used any form of tobacco, including cigarettes, pipes, cigars, or smokeless tobacco during pregnancy.
Magnitude of Low Birth Weight
Out of 380 respondents, 47 (12.4%); 95% CI: 8.8%-15.8%) had low birth weight. The mean birth weight of babies was 3181.97 (±556.7 SD) g.
Factors Associated With Low Birth Weight
In the bivariable analysis, 8 variables were identified as candidates for the multivariable model: maternal age, place of residence, gestational age, parity, hypertension, maternal weight, mid-upper arm circumference (MUAC), and alcohol consumption. The multivariable logistic regression analysis indicated that maternal age, place of residence, gestational age, and MUAC were significantly associated with low birth weight.
Mothers aged 15 to 19 years were nearly 12 times more likely to deliver low birth weight infants compared to mothers in other age groups (AOR = 11.9; 95% CI: 5.7-22.7). Similarly, mothers from rural areas had approximately 12 times higher odds of delivering a low birth weight baby than urban residents (AOR = 12.45; 95% CI: 6.7-16.2). Preterm delivery (before 37 weeks of gestation) was associated with a fourfold increase in the likelihood of low birth weight compared to deliveries at or beyond 37 weeks (AOR = 4.01; 95% CI: 1.59-10.08). Additionally, mothers with a MUAC below 23 cm were more than 5 times as likely to deliver low birth weight infants compared to those with MUAC ≥ 23 cm (AOR = 5.52; 95% CI: 4.7-17.8; Table 3).
Factors Associated With Low Birth Weight in Public Hospitals of Sidama Regional State, Ethiopia, 2024.
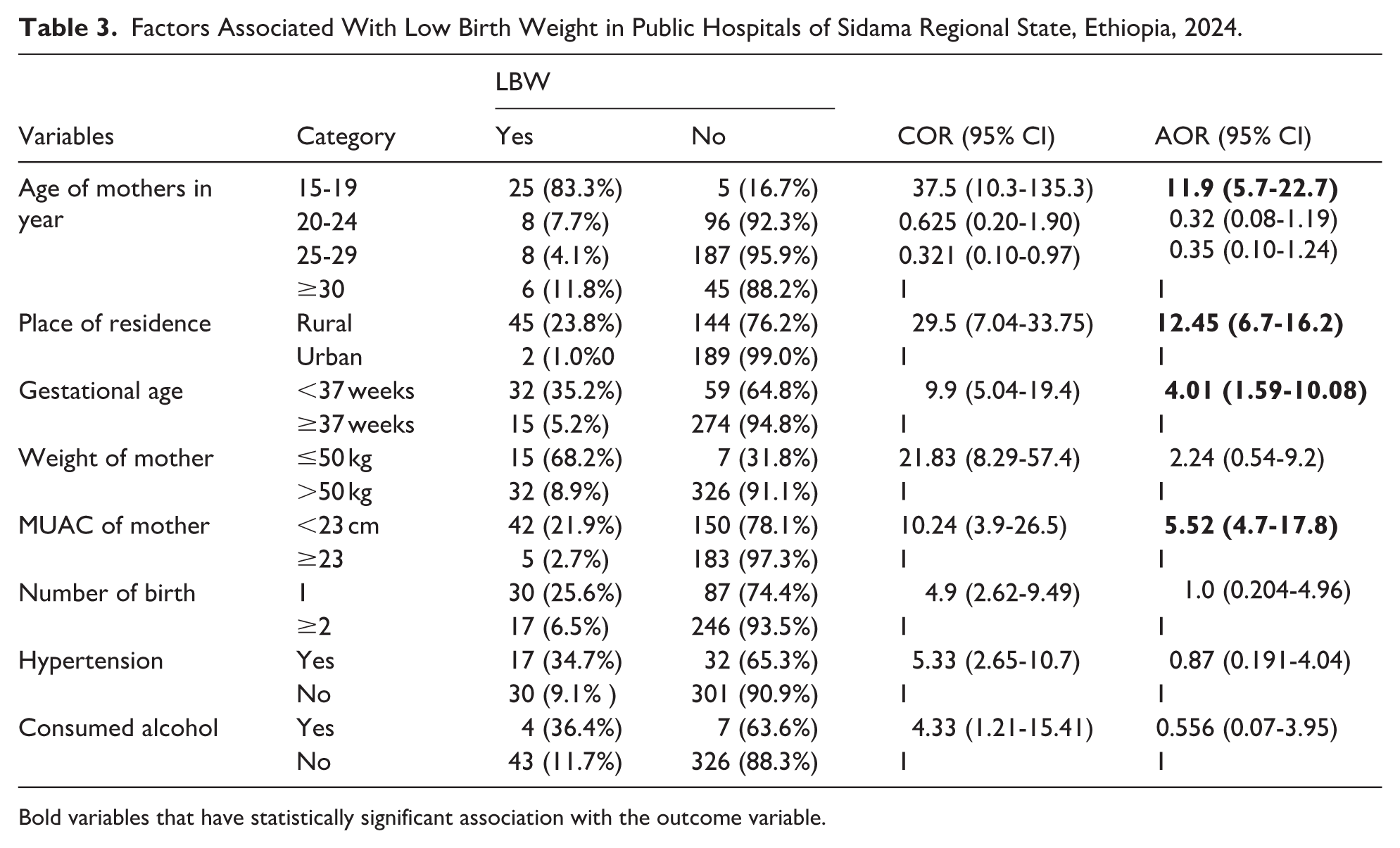
Bold variables that have statistically significant association with the outcome variable.
Discussion
This study aimed to assess the prevalence and factors associated with low birth weight among newborns delivered in public hospitals in the Sidama Region. The findings revealed a prevalence of LBW at 12.4% (95% CI: 8.8%-15.8%). Key predictors of low birth weight included maternal age, place of residence, gestational age, and maternal mid-upper arm circumference (MUAC).
The observed prevalence of 12.4% aligns with previous studies in Ethiopia, such as 1 conducted in Addis Ababa Public Hospitals (13.06%) 7 and another in Dangila Primary Hospital, Northwest Ethiopia (10.3%). 21 This finding is also consistent with research from Nepal (11.3%), 22 Burkina Faso (10.7%) 23 and Tanzania (13.6%). 24 The observed similarity in low birth weight (LBW) prevalence may largely stem from comparable socioeconomic profiles, including poverty levels, access to healthcare, nutritional practices, and education rates. These factors significantly impact maternal and child health outcomes, potentially resulting in similar LBW rates. Additionally, the quality and accessibility of healthcare services, particularly antenatal care, delivery practices, and neonatal care may be similar across these regions. Shared strengths or limitations within these healthcare systems could further explain the observed prevalence rates.
This prevalence is higher than that reported in a study conducted in southwestern Ethiopia, where the rate of low birth weight was 7.5%, 25 and in Bale Zone, Oromia Region, where it was 5.3%. 26 The discrepancy may be attributed to methodological differences: previous studies relied on birth weights recorded in medical records, whereas the present study measured the actual birth weight of newborns at delivery. Additionally, the current study was conducted in hospital settings, where referrals of high-risk pregnancies are more common, potentially increasing the observed prevalence. Furthermore, the inclusion of preterm births and multiple pregnancies in this study may have contributed to a higher prevalence of low birth weight.
In contrast, our finding of 12.4% is lower than that reported in several other studies. For instance, a study in Ghana found a prevalence of 23.7%. 3 It is also lower than studies from Gondar Town (17.4%), 27 Dire Dawa (21%), 28 Debre Markos Referral Hospital (26.3%) 29 and Dilla Town (34.1%). 19 These differences may be attributed to variations in study settings. While this study was conducted in selected public hospitals, the previous studies were carried out in specialized tertiary hospitals that often receive referrals of high-risk pregnancies from peripheral facilities. Additionally, geographical variations could influence health service utilization, socioeconomic status, and maternal nutritional status during pregnancy, all of which may contribute to the observed disparities in low birth weight prevalence.
Maternal age was significantly associated with low birth weight. Mothers aged 15 to 19 years were 11.9 times more likely to deliver low birth weight babies compared to mothers in other age groups. This finding is consistent with a study conducted in Dilla, which reported that maternal age under 20 years was significantly linked to low birth weight. 19 Several studies have observed that younger maternal age increases the risk of delivering a low birth weight infant.21 -23 This association is largely attributed to the physiological immaturity of adolescent mothers, whose reproductive systems may not be fully developed.4,10 Additionally, younger mothers, particularly first-time mothers, often experience poorer socioeconomic and reproductive conditions compared to older mothers, further elevating the risk of low birth weight. 23
Mothers from rural areas were 12.45 times more likely to deliver low-birth-weight babies compared to those from urban areas. This finding is consistent with previous studies conducted in Burkina Faso 23 and Dilla. 17 The similarity may be attributed to comparable socioeconomic conditions and geographical contexts in these settings.
Gestational age was a significant factor associated with low birth weight. Mothers who delivered before 37 weeks of gestation were 4.01 times more likely to have a low-birth-weight baby compared to those who delivered at or beyond 37 weeks. This finding is consistent with previous studies, including those conducted in Addis Ababa, 30 Dire Dawa, 28 and South-West Ethiopia. 25 The fetal origins of adult disease hypothesis suggests that events during fetal development, such as poor nutrition or stress can permanently alter organ development and metabolism, increasing the risk for low birth weight as a marker of poor fetal gsrowth. 31 The increased risk of low birth weight among preterm babies can be attributed to incomplete fetal growth and development. Babies born prematurely may not have reached the optimal stage of fetal development, where they would have gained sufficient weight. As a result, preterm babies are more likely to have low birth weight, which can have significant implications for their health and well-being. 32
Maternal mid-upper arm circumference (MUAC) was significantly associated with low birth weight. Mothers with a MUAC of less than 23 cm were 5.52 times more likely to deliver low-birth-weight infants compared to mothers with a MUAC of 23 cm or greater. This finding aligns with several studies in Ethiopia that have identified maternal MUAC as a factor associated with low birth weight, including research conducted in the Bale Zone, Oromia Region, 26 and the Sidama region. 33 This association may be due to inadequate food intake among pregnant women, leading to undernutrition and, consequently, low-birth-weight newborns. The intergenerational cycle of malnutrition further exacerbates this risk, with malnourished mothers being more prone to delivering low-birth-weight infants.
This study’s strength lies in the fact that trained midwives performed the weight measurements, and birth weights were recorded within 1 hour of childbirth. However, several limitations should be considered. The cross-sectional design of the study makes it difficult to establish causal relationships. Also, this study assessed alcohol use during pregnancy; it did not capture the experience of using other substances that could contribute for LBW. Furthermore, the exclusion of private health facilities and health centers may limit the generalizability of the findings to the broader population.
Conclusion
The prevalence of low birth weight is 12.4%, aligning with national studies. Factors such as the mother’s age, place of residence, gestational age, and maternal mid-upper arm circumference were significantly associated with low birth weight among neonates in the Sidama region of Ethiopia. Based on these findings, we recommend that healthcare providers focus on the early detection and management of risk factors leading to preterm delivery. This should be achieved through targeted antenatal care aimed at preventing low birth weight. Additionally, couples are encouraged to visit healthcare facilities early in pregnancy for counseling on the importance of nutritional supplementation. It is also advisable strengthened efforts to prevent adolescent pregnancies and discourage early marriage.
Footnotes
Acknowledgements
We would like to thank Yirgalem Hospital Medical College for its support to conduct this study. We would like to extend our genuine gratitude to the data collectors, supervisors and study participants.
Abbreviations
ANC = Antenatal Care
BMI = Body Mass Index
LBW = Low Birth Weight
MUAC = Mid-upper arm circumference
PTB = Preterm Birth
Author contributions
GN made considerable contributions to the conceptualization, data acquisition, and analysis, interpretation of data. AD contributed to formal analysis, interpretation of data, drafting and revising the document. The authors agreed to submit to the current journal, approved the version for publication, and took full responsibility for the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The finding of this study is generated from the data collected and analyzed based on stated methods and materials. The original data supporting this finding are available from the corresponding author on reasonable request.