
Abstract
Children with severe acute kidney injury (AKI) have had a high mortality rate despite the use of advanced renal replacement therapy (RRT). This study aims to determine the clinical outcomes and the predictors of survival in pediatric AKI requiring RRT in Thailand. All patients aged 1 month to 18 years with AKI requiring RRT in the Department of Pediatrics, Ramathibodi Hospital from January 1st, 2010 to December 31st, 2019 were enrolled. Clinical and laboratory data were obtained through a medical record review. There were 92 patients with a 45% survival rate. Five factors associated with mortality included multi-organ dysfunction syndrome, presence of sepsis, high pediatric risk of mortality III, use of nephrotoxic drugs, and use of vasopressors. By multivariate analysis, the presence of sepsis and the use of nephrotoxic drugs were independently associated with mortality. Patients with fluid overload ≥10% was associated with poor survival.
Introduction
Acute kidney injury (AKI) is common in critically ill children, occurring in 10% to 82% of critically ill patients depending on the definition and population studied.1,2 According to the reported data from a tertiary care hospital in Thailand, the incidence of AKI varies from 4.6 to 9.9 cases per 1000 pediatric patients admitted to general pediatric wards. 3 Children with severe AKI often need renal replacement therapy (RRT). Indications for RRT initiation include fluid overload, electrolyte imbalance, and uremia, which is refractory to medical treatments.
Children with severe AKI have a high mortality rate. In the 2010s, despite an improvement in pediatric critical care and the use of advanced RRT in developed countries, the mortality rates remained high, ranging from 36% to 50%.2,8,13,14 Risks of mortality in severe AKI requiring RRT include bone marrow transplantation, multi-organ dysfunction syndrome (MODS), sepsis, high degree of fluid overload, vasopressor use, late initiation of RRT, and infant patient.4-14
Choices of RRT in AKI are acute peritoneal dialysis (PD), intermittent hemodialysis (HD), and continuous renal replacement therapy (CRRT). Previously, only HD and PD were available, but CRRT has been increasingly used in Southeast Asian countries. The objective of this study was to determine the clinical outcomes and the predictors of survival in pediatric AKI requiring RRT at a tertiary care university hospital, Thailand.
Material and Methods
All patients aged 1 month to 18 years with AKI requiring RRT in the pediatric department, Ramathibodi hospital from January 1, 2010 to December 31, 2019 were enrolled. Clinical and laboratory data were obtained through a medical record review. Collected data included demographic and clinical information (age, gender, diagnosis, weight, height, fluid balance at hospital admission, RRT modalities, indication for RRT initiation, fluid balance at RRT initiation, use of diuretics and/or vasopressors, Pediatric Risk of Mortality III (PRISM III) score, hospital length of stay, PICU length of stay, duration and complication of RRT, and outcomes). The estimated glomerular filtration rate (eGFR) was calculated using the modified Schwartz et al formula. 15 The consultant nephrologist decided on the timing of RRT initiation and modality.
Stage of AKI was defined by serum creatinine and urine output, according to KDIGO 2012. 16 Sepsis was defined as pediatric systemic inflammatory response (SIRS) in the presence of or suspected infection. Multi-organ dysfunction syndrome (MODS) was defined as the presence of at least 3 failed organs, based on the criteria from the International pediatric sepsis consensus. 17 Severe dengue infection was defined by dengue infection with massive plasma leakage, respiratory distress, severe bleeding, or organ impairment. 18 Nephrotoxic substances were medications, contrast media, and toxic chemicals that affect kidney function.
The following formula was used to calculate the degree of fluid overload (FO) that developed between the diagnosis of AKI and the start of RRT: fluid overload (%) = [(fluid in−fluid out) ÷ (weight)] × 100, where fluid in (or out) is the amount of fluid in liters, and weight is measured in kilograms. Timing of RRT initiation was defined as the duration from the diagnosis of severe AKI to the start of RRT. The primary outcome was survival to hospital discharge. The secondary outcomes were the duration of RRT administration, the length of pediatric intensive care unit (PICU) stay, the length of hospital stay, and the renal outcomes in survivors.
Ethical Approval and Informed Consent
This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Ramathibodi Hospital Ethics Committee for Human Research approved this study (ID 2020/326). Informed consent was waived due to the retrospective nature of this study.
Statistical Analysis
Categorical variables were presented as number (percentage). Continuous variables were presented as mean ± standard deviation (SD), or median (interquartile range, IQR) as appropriate. The significance of differences between survivors and non-survivors was analyzed with the Chi-square test or the Fisher’s exact test, as appropriate. Comparisons between patient groups were performed using independent t-test or Mann-Whitney U test for continuous variables. Comparison of mortality rates among the 3 groups of fluid overload was performed using one-way analysis of variance. A univariate analysis was performed on clinical variables to identify the potential risk factors for mortality. Significant variables from univariate analysis were adopted in the multivariate logistic regression model to evaluate the association with mortality. Crude and adjusted odds ratios (ORs) and their corresponding 95% CIs were estimated. SPSS version 18 (SPSS, Inc., Chicago, IL, USA) was used for all statistical analysis. The P-value < .05 was considered statistically significant.
Results
There were 96 AKI patients requiring RRT in our pediatric department. Four patients were excluded due to known ESKD. Therefore, 92 patients were enrolled in the study. CRRT, HD, and PD were used in 69%, 26%, and 5% of these patients respectively. The patient survival rate was 44.6%. Demographic and clinical data are shown in Table 1. There were no significant differences in demographic data between survivors and non-survivors. The 5 most common comorbidities were sepsis (56.5%), hemato-oncologic diseases (37%), primary renal diseases (31.5%), severe dengue (10.9%), and status post hematopoietic stem cell transplant (10.9%). Primary renal disease comorbidity was more frequent in the survivor group than the non-survivor group. The non-survivor group had a higher percentage of sepsis comorbidity, nephrotoxic-drug uses, and vasopressor uses than the survivor group. The mean percentage of fluid overload (%FO) at RRT initiation was 14.9 ± 8.9. The non-survivor group showed a significantly higher amount of FO when compared with that of the survivor group.
Demographic and Clinical Data of Study Population.

Abbreviations: BMT, bone marrow transplantation; ECMO, extracorporeal membrane oxygenation.
When patients were stratified by degree of FO, patients with %FO < 10%, 10–20%, and >20% had significantly different mortality rate of 35.3%, 65.8%, and 70% respectively (P-value .011) (Figure 1).

Percentage of fluid overload at RRT initiation and mortality rate. Error bars represent 95% CI for the mortality rate. P = .011.
Univariate analysis showed that factors associated with mortality included the presence of sepsis, use of nephrotoxic drugs, use of vasopressors, MODS, PRISM III score ≥ 15%, and FO ≥ 10% (Table 2). On the other hand, patients with primary renal disease comorbidity had a lower mortality rate. Potentially influential variables were used in the multivariate logistic regression model. We found that sepsis and the use of nephrotoxic drugs were the independent risk factors for mortality with an adjusted odds ratio of 4.816 [95% CI, 1.488-15.587] and 3.434 [95% CI, 1.015-11.612] respectively. Primary renal disease was significantly associated with a better survival rate (Table 3).
Factors Associated With Patient Mortality by Univariate Logistic Regression.

Abbreviations: MODS, multi-organ dysfunction syndrome; PRISM III, pediatric risk of mortality III.
Predictors of Mortality in AKI Patients Requiring RRT by Multivariate Logistic Regression.

Abbreviations: MODS, multi-organ dysfunction syndrome; PRISM III, pediatric risk of mortality III.
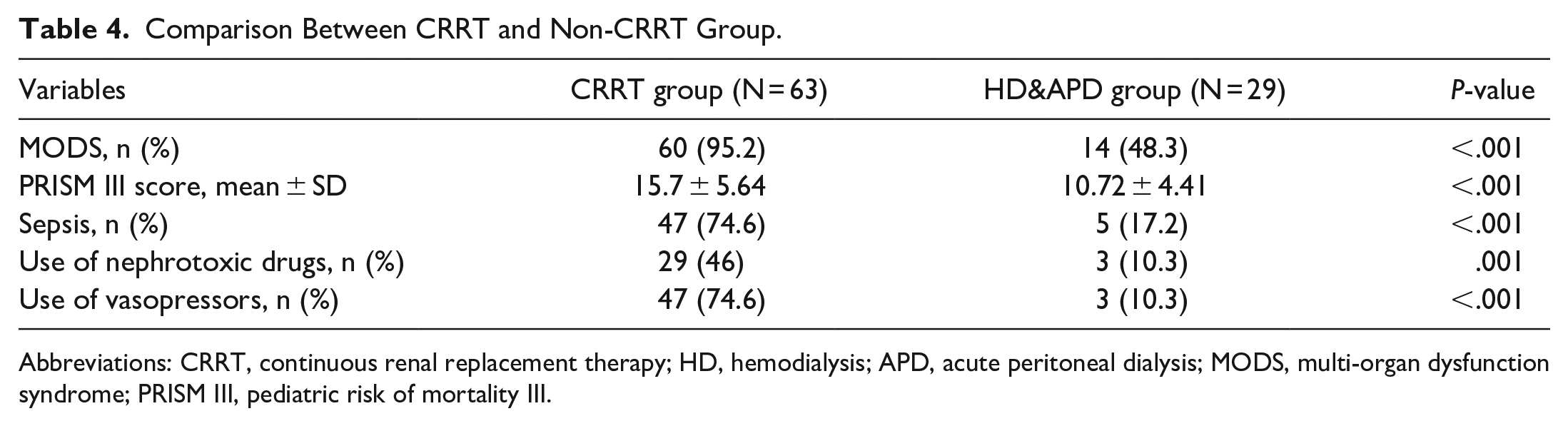
The mortality rate between RRT modalities was significantly different (P-value < .001). Those who received CRRT had a significantly higher mortality rate (47/63, 74.6%) than those who received PD (1/5, 20%) and HD (3/24, 12.5%). We then divided patients into 2 groups: the CRRT group and the non-CRRT (HD & PD) group. When we compared these groups, we found that patients who received CRRT had a significantly higher proportion of MODS (95.2% vs 48.3%, P-value < .001) and a mean PRISM III score (15.7 ± 5.64 vs 10.72 ± 4.41, P-value < .001). In addition, sepsis comorbidity, the use of nephrotoxic drugs, and the use of vasopressors were more common in the CRRT group (Table 4). In CRRT group, patients with %FO < 10%, 10–20%, and >20% had mortality rates of 58.8%, 82.8%, and 76.5% respectively, which were not significantly different (P-value .201).
Comparison Between CRRT and Non-CRRT Group.
Abbreviations: CRRT, continuous renal replacement therapy; HD, hemodialysis; APD, acute peritoneal dialysis; MODS, multi-organ dysfunction syndrome; PRISM III, pediatric risk of mortality III.
Overall, the median (IQR) duration of RRT administration was 6 (2.0-14.75) days, the median (IQR) length of PICU stay was 11.27 (5.56-18.66) days, and the median (IQR) length of hospital stay was 26.17 (12.77-48.85) days. In the survivor group, the median (IQR) duration of RRT administration was 7.13 (2.57-15.0) days and the median (IQR) length of PICU stay was 13 (7.0-18.58) days. In the non-survivor group, the median (IQR) duration of RRT administration was 5 (1.38-13.58) days and the median (IQR) length of PICU stay was 9.96 (4.0-20.46) days. The median duration of hospital stay was longer in the survivor group than in the non-survivor group (32.9 vs 19.0 days, P-value .008).
We assessed the renal outcomes of 41 survivors 3 months after starting RRT. The average eGFR was 104.2 ml/min/1.73 m2. Nine of the 41 patients had an eGFR of less than 60 ml/min/1.73 m2, and 8 of them had primary renal disease comorbidity. There are 4 dialysis-dependent patients, all of whom had primary renal disease comorbidity.
Discussion
Children with severe AKI requiring RRT have a high mortality rate. In this study, the overall mortality rate was 55.4%. This was higher than the mortality rate in previous pediatric studies.2,8,13,14 Various studies have attempted to determine risk factors for mortality. Higher severity of illness scores, including the pediatric index of mortality (PIM) and PRISM scores, was found in the non-survivors.9-11,13 On the other hand, some studies reported that these scores were not significantly different between survivors and non-survivors.7,12,14 In our study, the PRISM III scores were significantly higher in the non-survivors in univariate analysis but were not an independent factor in the multivariate analysis.
Patients with severe AKI usually have other organ dysfunctions. Studies in The Prospective Pediatric Continuous Renal Replacement Therapy (ppCRRT) Registry Group have reported that MODS was common in pediatric patients receiving CRRT and independently associated with mortality.8,10 Similarly, Hayes et al reported that the presence of MODS was significantly associated with increased mortality. 12 We also found MODS at 80.4% in our study population and MODS was significantly associated with mortality.
The use of vasopressors has been described as a poor prognostic factor in several studies. Bunchman et al reported that the requirement for vasopressors was the most predictive of outcome in children. The survival rates were 35% and 89% in children requiring vasopressors and not requiring vasopressors respectively. 6 Moreover, Foland et al reported that vasoactive infusion, which was used for cardiovascular support, was significantly more frequent in non-survivors. 9 Our study is consistent with these studies in that the use of vasopressors was significantly associated with poor survival.
Sepsis was a common leading cause of CRRT use.8,10,13 Although sepsis was not associated with survival, according to a recent study, 13 sepsis was the independent risk factor for mortality in our study. We found that AKI patients with sepsis comorbidity preceding RRT administration had 4 times increased risk of mortality. In the same way, Hayes et al reported that the odds ratio of mortality in the presence of sepsis was 6.8 after controlling covariates. 12
The use of nephrotoxic drugs is one of many causes of AKI.3,16 Some drugs result in irreversible kidney damage and may contribute to morbidity and mortality. In our multivariate analyses, we found that the use of nephrotoxic drugs was an independent risk factor for death.
Several CRRT studies reported the association between the degree of fluid overload (%FO) and survival. Foland et al collecting data of fluid balance up to 7 days before CVVH, found that the median %FO were 7.8 and 15.1 in survivors and non-survivors respectively. The authors demonstrated that the amount of fluid retention before the initiation of CVVH was independently associated with survival, as well as in subgroups of patients with MODS. 9 According to Pichler et al non-survivors had more severe FO than survivors (45% vs 12% respectively). 11 Goldstein et al calculated %FO by considering total fluid intake and output data from ICU admission to CRRT initiation. Survivors and non-survivors had the mean %FO of 14.2 and 25.4 percent respectively, and %FO remained substantially lower for survivors versus non-survivors in a multivariate analysis adjusted for illness severity. 10 Hayes et al reported that the median %FO were 7.3 and 22.3 in survivors and non-survivors respectively, and the odds ratio of mortality in patients with >20% FO was 6.1. 12 In a large cohort of critically ill children receiving CRRT, the mean %FO was 12.5 and 23 in survivors and non-survivors respectively. The mortality rates were 29.4%, 43.1%, and 65.6% in patients with <10% FO, 10% to 20% FO, and >20% FO respectively. In addition, there was a 3% increase in mortality for each 1% increase in the degree of fluid overload at CRRT initiation. 8 Recently, Cortina et al reported the mortality rate of 20.6%, 54.1%, and 77.3% in patients with <10% FO, 10% to 20% FO, and >20% FO respectively. They reported that greater FO was an independent risk factor for death in multivariate analysis. 13 In our study, an increase in survival of pediatric AKI patients who required RRT was associated with less fluid overload. This finding is comparable with data from previous studies. However, the greater degree of FO was not significant in our multivariate analysis controlling for comorbidities and severity of illness. Furthermore, in our CRRT subgroup, the difference in mortality rates among the groups of FO was not statistically significant. This discrepancy may be explained by a slightly higher mortality rate in our CRRT subgroup and a small number of each group of FO.
To date, CRRT has been increasingly used in developing countries. CRRT studies in the last decade reported that the mortality rate was 36% to 63%.2,8,13,14 The presence of MODS was described at 57.7% to 78.5%.8,13 The mean PRISM III score was 14.0 to 14.3.8,14 In our CRRT subgroup, the mortality rate was higher than that of previous studies. This may be explained by the fact that most of our CRRT patients had MODS and a relatively high PRISM III score. The higher mortality rate of CRRT patients among all RRT modalities was more likely to be related to more severe underlying conditions, not the RRT modality itself.
Focusing on the timing of initiation, in a pediatric study, Cortina et al determined the timing of initiation as an independent predictor of mortality. 13 On the other hand, a large, multinational, randomized trial in critically ill adult patients with severe acute kidney injury found that an accelerated renal replacement strategy was not associated with a lower risk of death at 90 days than a standard strategy. 19 In our study, the timing of initiation was not associated with survival. We prefer that a prospective pediatric study with a standardized protocol be required to determine the effect of timing of RRT initiation on survival.
Patients with AKI are considered to be at increased risk for CKD. 16 A quarter of the survivors in our study had developed chronic kidney disease. Patients with primary renal disease were at a high risk for chronic kidney disease and end-stage kidney disease despite having lower mortality.
Our study has some limitations. First, we did not include pediatric postoperative cardiac surgical patients requiring RRT because, in our institute, peritoneal dialysis prescription in these children was decided by cardiovascular surgeons, not by the nephrologists. Second, it is a small retrospective study conducted in a single center. Third, there was no record of the delivered dose of CRRT. Accordingly, we could not demonstrate the outcome of different doses of CRRT.
In conclusion, pediatric patients with severe AKI requiring RRT in our country still had a high mortality rate. Fluid overload more than 10% associated with poor survival. Sepsis and the use of nephrotoxic drugs were the independent risk factors of mortality.
Footnotes
Author Contributions
Kanchana Tangnararatchakit made substantial contributions to the conception, design, and interpretation of data; supervised the results; drafted the manuscript; and granted approval to the final version of the manuscript. Chayuttra Voraruth made substantial contributions to the conception, design, and acquisition of data; performed statistical analysis; drafted the manuscript; and granted approval to the final version of the manuscript. Kwanchai Pirojsakul, Pawaree Saisawat and Songkiat Chantarogh made substantial contributions to the conception and design, discussed the results, commented on previous versions of the manuscript, and contributed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.