
Abstract
Objective
To investigate the association between serum phosphate levels and the risk of 28-day mortality in critically-ill patients with septic acute kidney injury (AKI) undergoing continuous renal replacement therapy (CRRT).
Methods
This retrospective cohort study analysed data from critically-ill patients with septic AKI who underwent CRRT between January 2009 and September 2016. Demographic, clinical and routine biochemical data were retrieved from a database and analysed to identify risk factors for 28-day mortality.
Results
A total of 796 patients were included in the analyses. Multivariate regression analyses showed that phosphate (0 h), phosphate (24 h) and delta phosphate were associated with the 28-day mortality in patients with septic AKI undergoing CRRT. The adjusted odds ratios (95% confidence interval) were 1.12 (1.03, 1.22), 1.22 (1.14, 1.30) and 1.12 (1.04, 1.20) for phosphate (0 h), phosphate (24 h) and delta phosphate, respectively. Curve fitting and threshold analyses showed that when phosphate (0 h) was between 5.6 mg/dl and 8.7 mg/dl, phosphate (24 h) was >3.8 mg/dl and delta phosphate was >–1, the 28-day mortality risk increased significantly.
Conclusion
In patients with septic AKI undergoing CRRT, serum phosphate level was associated with the prognosis of patients in terms of 28-day mortality.
Introduction
Approximately 20–30 million people suffer from sepsis every year worldwide and approximately 1400 people die of sepsis every day. 1 Septic acute kidney injury (AKI) is the most common AKI syndrome observed in the intensive care unit (ICU) and it accounts for approximately half of all cases of AKI. 2 The renal function of these patients may be temporarily or completely lost. 3 In such cases, the use of continuous renal replacement therapy (CRRT) becomes necessary and appropriate. CRRT is superior compared with intermittent haemodialysis in terms of maintaining hemodynamic stability, solute clearance, and ultrafiltration capacity. 4 Phosphate is the third most abundant mineral in living systems. 5 The serum phosphate level is associated with the outcomes of critically-ill patients. 6 Serum phosphate is associated with disease severity and adverse outcomes of patients undergoing CRRT. 7 To date, research into the relationship between serum phosphate levels and disease severity in sepsis patients with AKI undergoing CRRT is lacking. Therefore, this current study investigated the association between the serum phosphate level and the 28-day mortality risk of sepsis patients with AKI undergoing CRRT.
Patients and methods
Study design and population
This retrospective cohort study analysed data provided by Seung Hyeok Han, Department of Internal Medicine, College of Medicine, Institute of Kidney Disease Research, Yonsei University, Seoul, Korea, which were stored on the Dryad Digital Repository. 8 The database is a public data repository into which the authors had uploaded previously published data.7,9 The study participants included patients undergoing CRRT between January 2009 and September 2016 in the ICUs at Yonsei University Health System Severance Hospital, Seoul, Korea and the National Health Insurance Service Medical Centre Ilsan Hospital, Ilsan, Korea. The inclusion criteria were as follows: (i) patients that met the diagnostic criteria for Sepsis-3 (patients with infection and a sequential organ failure assessment [SOFA] score ≥2); 10 (ii) patients with stage 2 according to the Acute Kidney Injury Network (AKIN) criteria; 11 (iii) patients treated using CRRT. The exclusion criteria were as follows: (i) aged <18 years; (ii) pre-existing chronic kidney disease (CKD), dialysis or CRRT use prior to the study; (iii) pregnancy; (iv) postrenal obstruction; (v) prior kidney transplantation.
Ethical approval was provided by the Ethical Review Board of The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi Province, China (no. 2018049). Consent was not required because of the retrospective nature of this study.
Clinical and biochemical data collection
Demographic and clinical data including age, sex, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), the reason for using CRRT and comorbidities were recorded. Phosphate (0 h) was measured before starting CRRT (0 h), phosphate (24 h) was measured at 24 h after CRRT initiation and delta phosphate was the difference between phosphate (24 h) and phosphate (0 h). The following biochemical laboratory data were recorded at baseline (0 h): haemoglobin (Hb), white blood cell (WBC) count, serum creatinine (Cr), albumin (Alb), HCO3–, K+, blood urea nitrogen (BUN), C-reactive protein (CRP) and glomerular filtration rate (GFR). The following disease severity indices were also recorded: SOFA score, APACHE II score and Charlson comorbidity index (CCI).12,13
CRRT protocol
Nephrologists decided whether or not to initiate CRRT upon the development of sepsis with AKI in ICU patients. The indications for CRRT use included uncontrolled volume overload, intractable hyperkalaemia or metabolic acidosis. The type of CRRT used was continuous venovenous haemodiafiltration through the internal jugular, subclavian or femoral veins. CRRT was started at a blood flow rate of 100 ml/min and was increased up to 150 ml/min. The total effluent volume as a sum of the dialysis and replacement doses was targeted to deliver ≥35 ml/kg per h in all patients using a multiFiltrate machine (Fresenius Medical Care, Bad Homburg, Germany) or a PRISMAFLEX System (Baxter International, Lund, Sweden).
Statistical analyses
All the statistical analyses were performed using EmpowerStats (version 2018-05-05; copyright 2009; X&Y Solutions, Boston, MA, USA) and R software (version 3.5.2). 14 Data are presented as mean ± SD for continuous variables at baseline and categorical data are shown as n of patients (%). Univariate analyses were undertaken to detect the possible risk factors for 28-day mortality. Multivariate analyses were adjusted for the possible variables that may affect the prognosis of patients to determine the relationship between phosphate (0 h), phosphate (24 h) and delta phosphate and 28-day mortality. A sensitivity analysis was carried out based on the indications for CRRT use and whether or not mechanical ventilation was used in order to verify the relationship between phosphate and 28-day mortality. A two-piecewise linear regression model was used to examine the threshold effect of serum phosphate on the risk of 28-day mortality in patients with sepsis being treated with CRRT using a smoothing function. Finally, the threshold effect was analysed to find the cut-off value. The threshold level (i.e. turning point) was determined using trial and error, including selection of turning points along a pre-defined interval and then choosing the turning point that gave the maximum model likelihood. A log likelihood ratio test was used to compare the one-line linear regression model with a two-piecewise linear model. Pearson's test was used to analyse the correlation between serum phosphate and 28-day mortality in patients with sepsis being treated with CRRT. A P-value < 0.05 was considered statistically significant.
Results
From January 2009 to September 2016, 2391 patients underwent CRRT. Of these, 1595 patients were excluded for the following reasons: stage I AKIN (n = 281); age < 18 years (n = 42); pre-existing CKD or dialysis or CRRT prior to the study (n = 585); pregnancy (n = 12); postrenal obstruction (n = 263); prior kidney transplantation (n = 64); and non-sepsis patients (n = 348). A total of 796 cases met the inclusion and exclusion criteria and were included in this study. The baseline clinical and demographic characteristics of the patients are shown in Table 1. The mean ± SD age of the patients was 63.51 ± 14.18 years and 494 (62.1%) were male. The mean ± SD BMI of the study cohort was 23.59 ± 4.45 kg/m2. The mean ± SD mean arterial pressure (MAP) was 77.58 ± 14.90 mmHg. The prevalence of cerebrovascular disease, peripheral vascular disease, hypertension, diabetes mellitus and chronic obstructive pulmonary disease (COPD) was 72 (9.05%), 30 (3.77%), 420 (52.76%), 269 (33.79%) and 68 (8.54%), respectively.
The baseline clinical and demographic characteristics of the patients (n = 796) who participated in this study to determine the association between the serum phosphate level and the 28-day mortality risk of sepsis patients with acute kidney injury undergoing continuous renal replacement therapy (CRRT).

Data presented as mean ± SD or n of patients (%).
The univariate analyses found that the phosphate (0 h), phosphate (24 h) and delta phosphate were associated with 28-day mortality; with the odds ratio (OR) and 95% confidence interval (95% CI) being 1.08 (95% CI 1.04, 1.12), 1.16 (95% CI 1.12, 1.19) and 1.09 (95% CI 1.05, 1.14), respectively (Table 2). The univariate analyses also found that BMI, SBP, DBP, MAP, hypertension, mechanical ventilation, CCI, CRRT indication, Alb, APACHE II score, SOFA score and Hb were also associated with 28-day mortality.
Univariate analysis of the risk factors for 28-day mortality in patients (n = 796) who participated in this study to determine the association between the serum phosphate level and the 28-day mortality risk of patients with septic acute kidney injury undergoing continuous renal replacement therapy (CRRT).

NS, no significant association with 28-day mortality (P ≥ 0.05).
The multivariate regression analysis adjusted for the following confounding variables: age, sex, BMI, SBP, DBP, myocardial infarction, congestive heart failure, cerebrovascular disease, peripheral vascular disease, diabetes mellitus, hypertension, COPD, CRRT indication, CCI, Alb, APACHE II score, SOFA score, CRP, GFR, Cr, mechanical ventilation at CRRT initiation, WBC, Hb, BUN, K+ and HCO3–. In the adjusted models, the analyses found that the phosphate (0 h), phosphate (24 h) and delta phosphate were associated with 28-day mortality: the adjusted ORs (95% CI) were 1.12 (1.03, 1.22), 1.22 (1.14, 1.30) and 1.12 (1.04, 1.20), respectively (Table 3). The findings of the univariate analyses and multivariate regression analyses were consistent. The size of the risk effect of phosphate (0 h), phosphate (24 h) and delta phosphate on 28-day mortality increased after adjusting for confounding variables.
Multivariate regression analysis of the risk factors for 28-day mortality in patients (n = 796) who participated in this study to determine the association between the serum phosphate level and the 28-day mortality risk of patients with septic acute kidney injury undergoing continuous renal replacement therapy (CRRT).

Adjusted variables: age; sex; body mass index; systolic blood pressure; diastolic blood pressure; myocardial infarction; congestive heart failure; cerebrovascular disease; peripheral vascular disease; diabetes mellitus; hypertension; chronic obstructive pulmonary disease; continuous renal replacement therapy indication; Charlson comorbidity index; albumin; APACHE II score; sequential organ failure assessment score; C-reactive protein; glomerular filtration rate; serum creatinine; mechanical ventilation at CRRT initiation; white blood cell count; haemoglobin; blood urea nitrogen; K+; HCO3–.
A subgroup analysis was carried out separately based on the reason for CRRT use and whether or not mechanical ventilation was used at CRRT initiation. As the phosphate (0 h) increased, the risk of 28-day mortality of patients with volume overload and metabolic acidosis increased; adjusted ORs (95% CI) were 1.60 (1.07, 2.38) and 1.31 (1.02, 1.69), respectively (Table 4). As the phosphate (24 h) increased, the risk of 28-day mortality of patients with volume overload and oliguria increased; adjusted ORs (95% CI) were 13.32 (3.67, 48.35) and 1.21 (1.03, 1.41), respectively. However, as the delta phosphate increased, the risk of 28-day mortality did not increase in the different subgroups based on the reason for CRRT use. In the mechanically ventilated patients, the subgroup analysis found that if the phosphate (0 h), phosphate (24 h) and delta phosphate increased, the risk of 28-day death increased; adjusted ORs (95% CI) were 1.13 (1.03, 1.24),1.23 (1.15, 1.32) and 1.13 (1.04, 1.22), respectively (Table 5). In the patients without mechanical ventilation, as the phosphate (0 h) and phosphate (24 h) increased, the risk of 28-day mortality also increased; adjusted ORs (95% CI) were 2.08 (1.27, 3.40) and 2.13 (1.23, 3.69), respectively. However, as delta phosphate increased in patients without mechanical ventilation, the risk of 28-day mortality did not increase; the adjusted OR (95% CI) was 1.21 (0.76, 1.92).
Subgroup analysis of the risk for 28-day mortality in patients (n = 796) with septic acute kidney injury undergoing continuous renal replacement therapy (CRRT) stratified according to the reason for CRRT use.

Adjusted variables: age; sex; body mass index; systolic blood pressure; diastolic blood pressure; myocardial infarction; congestive heart failure; cerebrovascular disease; peripheral vascular disease; diabetes mellitus; hypertension, chronic obstructive pulmonary disease; Charlson comorbidity index; albumin; APACHE II score; sequential organ failure assessment score; C-reactive protein; glomerular filtration rate; serum creatinine; mechanical ventilation at CRRT initiation; white blood cell count; haemoglobin; blood urea nitrogen; K+; HCO3–.
NS, no significant association with 28-day mortality (P ≥ 0.05).
Subgroup analysis of the risk for 28-day mortality in patients (n = 796) with septic acute kidney injury undergoing continuous renal replacement therapy (CRRT) stratified according to the use of mechanical ventilation at CRRT initiation.
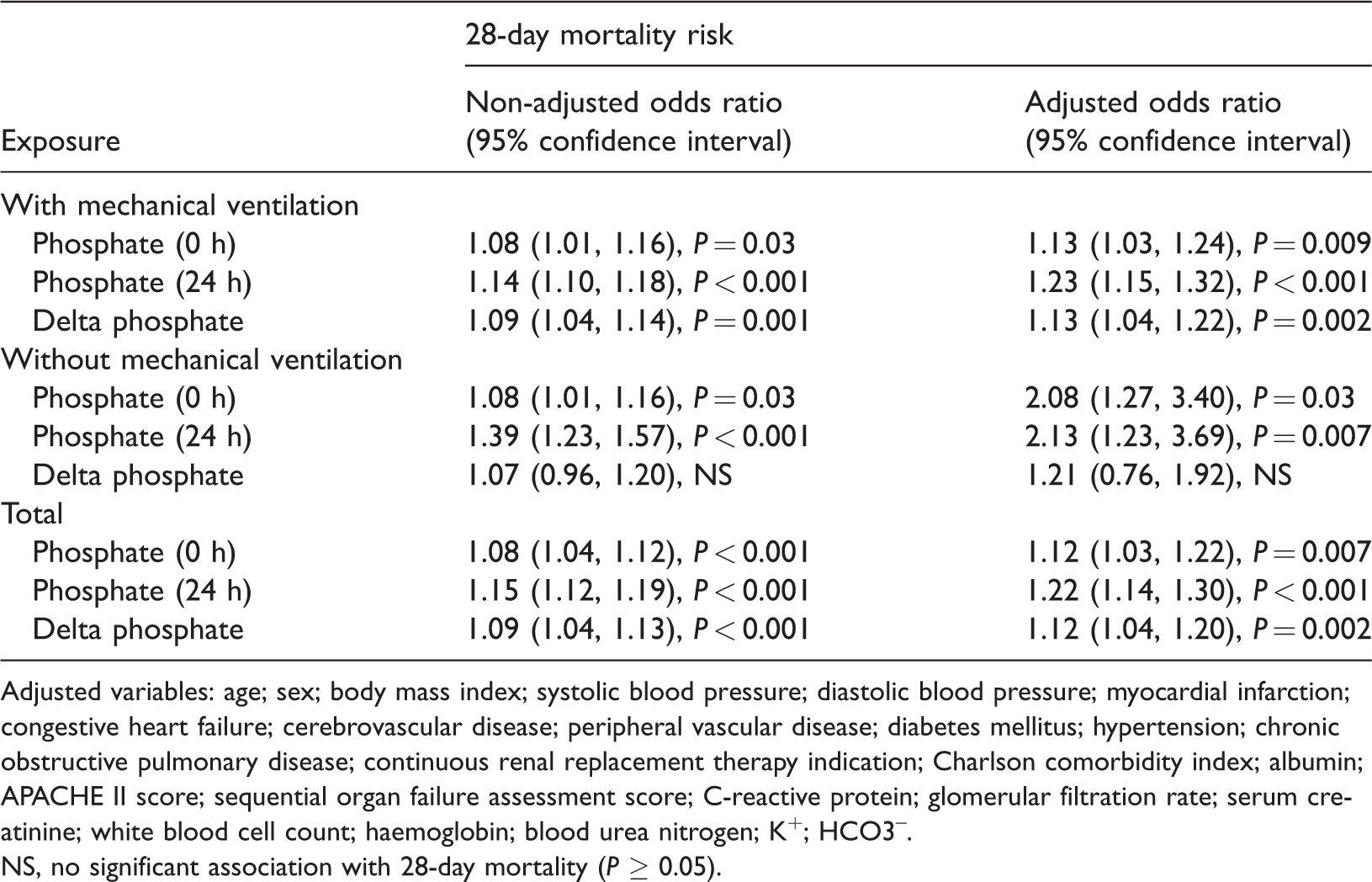
Adjusted variables: age; sex; body mass index; systolic blood pressure; diastolic blood pressure; myocardial infarction; congestive heart failure; cerebrovascular disease; peripheral vascular disease; diabetes mellitus; hypertension; chronic obstructive pulmonary disease; continuous renal replacement therapy indication; Charlson comorbidity index; albumin; APACHE II score; sequential organ failure assessment score; C-reactive protein; glomerular filtration rate; serum creatinine; white blood cell count; haemoglobin; blood urea nitrogen; K+; HCO3–.
NS, no significant association with 28-day mortality (P ≥ 0.05).
When phosphate (0 h) was between 5.6 mg/dl and 8.7 mg/dl, for every 1 mg/dl increase in phosphate (0 h), the risk of 28-day mortality increased by 35%; the adjusted OR (95% CI) was 1.35 (1.07, 1.70) (Table 6; Figure 1). When phosphate (0 h) was >8.7 mg/dl or <5.6 mg/dl, as the phosphate (0 h) increased, the risk of 28-day mortality did not increase. When phosphate (24 h) was >3.8 mg/dl, for every 1 mg/dl increase in phosphate (24 h), the risk of 28-day mortality increased by 23%; the adjusted OR (95% CI) was 1.23 (1.15, 1.33) (Figure 2). When delta phosphate was >–1, for every 1 mg/dl increase in delta phosphate, the risk of 28-day mortality increased by 22%; the adjusted OR (95% CI) was 1.22 (1.10, 1.35) (Figure 3). When phosphate (24 h) was ≤3.8 mg/dl and delta phosphate was ≤–1, the risk of 28-day mortality did not increase.

Adjusted smoothing function of the threshold effect analysis of phosphate (0 h) on 28-day mortality in patients (n = 796) with septic acute kidney injury undergoing continuous renal replacement therapy. The colour version of this figure is available at: http://imr.sagepub.com.

Adjusted smoothing function of the threshold effect analysis of phosphate (24 h) on 28-day mortality in patients (n = 796) with septic acute kidney injury undergoing continuous renal replacement therapy. The colour version of this figure is available at: http://imr.sagepub.com.

Adjusted smoothing function of the threshold effect analysis of delta phosphate on 28-day mortality in patients (n = 796) with septic acute kidney injury undergoing continuous renal replacement therapy. The colour version of this figure is available at: http://imr.sagepub.com.
Threshold effect analysis of phosphate (0 h), phosphate (24 h) and delta phosphate on 28-day mortality in patients (n = 796) with septic acute kidney injury undergoing continuous renal replacement therapy (CRRT).

Adjusted variables: age; sex; body mass index; systolic blood pressure; diastolic blood pressure; myocardial infarction; congestive heart failure; cerebrovascular disease; peripheral vascular disease; diabetes mellitus; hypertension; chronic obstructive pulmonary disease; continuous renal replacement therapy indication; Charlson comorbidity index; albumin; APACHE II score; sequential organ failure assessment score; C-reactive protein; glomerular filtration rate; serum creatinine; mechanical ventilation at CRRT initiation; white blood cell count; haemoglobin; blood urea nitrogen; K+; HCO3–.
NS, no significant association with 28-day mortality (P ≥ 0.05).
Discussion
This current study found that phosphate (0 h), phosphate (24 h) and delta phosphate were associated with 28-day mortality risk in critically-ill patients with septic AKI undergoing CRRT according to both univariate analyses and multivariate regression analyses. The curve fitting and threshold analysis showed that the threshold of phosphate (0 h) was between 5.6 mg/dl and 8.7 mg/dl, the threshold of phosphate (24 h) was 3.8 mg/dl and the threshold of delta phosphate was –1. When phosphate (0 h) was between 5.6 mg/dl and 8.7 mg/dl, phosphate (24 h) was >3.8 mg/dl and delta phosphate was >–1, the 28-day mortality risk increased significantly.
Acute kidney injury and systemic inflammatory response syndrome are two reasons for using CRRT patients with sepsis.15,16 AKI occurs in approximately 25–50% of patients with severe sepsis and is associated with a high mortality rate (40–60%) and long-term morbidity. 3 Most patients with septic AKI need renal replacement therapy.17,18 CRRT is the most appropriate and most frequently used treatment in patients with sepsis because they are generally haemodynamically unstable. 19 Studies have shown that the serum phosphate level was associated with the outcomes of critically-ill patients and those undergoing CRRT.7,20 However, investigations into the role of serum phosphate levels in patients with septic AKI undergoing CRRT in the ICU are lacking.
Phosphate is present in all cells of the body and is involved in almost all physiological chemical reactions. 21 Phosphate is also an important substance that makes the heart beat regularly, 22 maintains normal kidney function, 23 and conveys nerve stimulation. 24 A meta-analysis that included 1555 critically-ill patients showed that hypophosphataemia was associated with severity of illness, prolonged duration of mechanical ventilation, length of ICU stay and higher mortalities. 20 Another study that analysed 198 mechanically-ventilated ICU patients with severe sepsis or septic shock found that time-weighted hyperphosphataemia increased mortality. 25 These previous findings suggest that phosphate metabolic disorders are associated with the prognosis of critically-ill patients.20,25
This current study found that the serum phosphate level was associated with the prognosis of critically-ill patients with septic AKI undergoing CRRT, which was consistent with the relevant previous research results. 7 The analyses undertaken in this current study adjusted for confounding variables that may have affected the prognosis of critically-ill patients, 7 so that the findings should be more reliable. At the same time, a sensitivity analysis by subgroup was undertaken to further improve the reliably of the findings. 26 The subgroup analyses found that some of the results became nonsignificant or were missing, but the direction of the trend for most of the results was consistent. The possible reasons for this was that the sample size of each subgroup decreased, which might decrease the ability of the statistical test to identify significant associations. In addition, this current study not only found that the serum phosphate level was associated with the prognosis of critically-ill patients with septic AKI undergoing CRRT, but it also found the threshold serum phosphate level using curve fitting and threshold analyses. Most previous studies have only shown a correlation between serum phosphate level and the prognosis of patients;5–7 with only one study providing a cut-off value of serum phosphate level that was obtained by clinical research. 7
A limitation of the current study was that the study population only comprised of patients with septic AKI undergoing CRRT, so the clinical application of the conclusions beyond that specific population is limited.
In conclusion, this current study demonstrated that serum phosphate was associated with the prognosis of patients with septic AKI undergoing CRRT. The findings suggest that phosphate (0 h) < 5.6 mg/dl, phosphate (24 h) ≤3.8 mg/dl and delta phosphate ≤ –1 may be the optimum phosphate levels to reduce the 28-day mortality rate. Subgroup analyses suggested that the phosphate levels should be controlled more strictly, especially in patients with volume overload and mechanical ventilation, because for every 1 mg/dl increase in serum phosphate, the risk of 28-day mortality increased.
Footnotes
Authors' contributions
Hai Wang and Zheng-Hai Bai wrote the manuscript; Jun-Hua Lv, Jiang-Li Sun and Yu Shi undertook the statistical analyses; Zheng-Liang Zhang and Hong-Hong Pei were responsible for designing the research, process guidance, checking and correction.
Acknowledgements
The authors thank Seung Hyeok Han for providing data from the Dryad Digital Repository.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.