
Abstract
Objectives:
This case report describes two cases of high-dose methotrexate–induced nephrotoxicity: death in the case of conventional supportive care and successful renal function recovery in a patient treated with glucarpidase and continuous dialysis.
Methods:
High dose methotrexate is widely used for management of adult and pediatric malignancies. However, high-dose methotrexate–induced renal nephrotoxicity may cause severe, even lethal complications. Here we present examples of such outcomes.
Results:
We present one case of lethal high-dose methotrexate nephrotoxicity in a patient treated with conventional rescue therapy. We contrast this outcome with another patient with high-dose methotrexate–induced anuric acute kidney injury, who has recovered renal function following therapy with glucarpidase and continuous dialysis.
Conclusions:
This is only the second reported case of high-dose methotrexate–induced anuric acute kidney injury, and the only one with a reported clinical outcome. This first report of recovery from high-dose methotrexate–induced anuric acute kidney injury after glucarpidase administration supports available evidence pointing to the effectiveness of this therapy.
Introduction
Methotrexate (MTX) is a dihydrofolate reductase inhibitor that blocks de novo nucleotide synthesis. It is used in the treatment of many conditions ranging from autoimmune disease to malignancies, with doses ranging from 20 mg/m2 per week to 1000–33,000 mg/m2 depending on indication. 1 The latter dose range is known as high-dose methotrexate (HDMTX), which is often used as the first-line treatment of central nervous system (CNS) lymphoma and acute lymphoblastic leukemia, among other indications.1–3 However, HDMTX therapy may be nephrotoxic in up to 12% of patients.1,3 It is believed that MTX induces renal injury either by precipitation in, or a direct toxic effect on, the renal tubules. 1 MTX and its metabolites are poorly soluble when in acidic environments, promoting potential precipitation in acidic urine. 1 Strategies for prevention of the HDMTX nephrotoxic effects include adequate hydration, urine alkalinization, and leucovorin rescue. 3
Since over 90% of MTX is cleared by kidneys, 1 HDMTX-induced kidney injury is central in the development of other HDMTX toxicities including myelosuppression and mucositis. 1 The threshold MTX levels triggering such toxicity are 5–10, 1, and 0.1 µM at 24, 48, and 72 h, respectively.1,3
Once HDMTX-induced renal dysfunction is manifested by oliguria, rising creatinine, or elevated MTX levels, management options include high-dose leucovorin rescue, extracorporeal methods of MTX removal (e.g. hemodialysis (HD)), or administration of glucarpidase.1,3 The recently developed therapy glucarpidase, a recombinant bacterial enzyme that hydrolyzes MTX to inactive metabolites, rapidly lowers plasma MTX concentrations (by over 98% within 15 min of administration) and is relatively well tolerated. 1
Here, we contrast outcomes of two cases of HDMTX nephrotoxicity: death in the case of conventional supportive care and successful renal function recovery in a patient treated with glucarpidase and continuous dialysis.
Patient A
A 54-year-old white male with Waldenstrom’s macroglobulinemia was scheduled for treatment with autologous stem cell transplant. Due to rising immunoglobulin M level to 1600 mg/dL, he received chemo-mobilization with cyclophosphamide. This therapy was complicated by acute kidney injury (AKI; serum creatinine rising to 1.8 mg/dL); however, his kidney function recovered with intravenous hydration (serum creatinine returned to baseline of 0.9 mg/dL). This episode of AKI was closely associated with receiving cyclophosphamide and attributed to pre-renal injury because of its improvement with intravenous fluids. Three months after chemo-mobilization with cyclophosphamide, he was diagnosed with CNS lymphoma and, instead of the stem cell transplant, was scheduled to receive HDMTX therapy.
His physical examination on the day of HDMTX was unremarkable with the exception of class 2 obesity (body weight 128.6 kg; body mass index (BMI) of 38.5). Therefore, his MTX dose was reduced to intravenous 6 g/m2 from a standard 8 g/m2 (total 14 g), and it was given with leucovorin rescue and prophylactic maintenance intravenous fluids.
After administration of MTX, the patient became anuric and encephalopathic with only 65 mL of urine output over 24 h after the HDMTX. His creatinine rose from 1.3 to 3.1 mg/dL during this time period and potassium to 5.7 from normal baseline. Urinalysis reported 2+ blood and protein, but manual urine microscopy was bland (no crystals or active sediment) and there was no evidence of obstruction on renal ultrasound. His MTX level at 24 h post-HDMTX was 201.2 µM (Figure 1, left panel). The proximity of AKI to MTX administration, elevated serum MTX levels, and lack of other obvious causes lead to the suspected diagnosis of HDMTX nephrotoxicity.
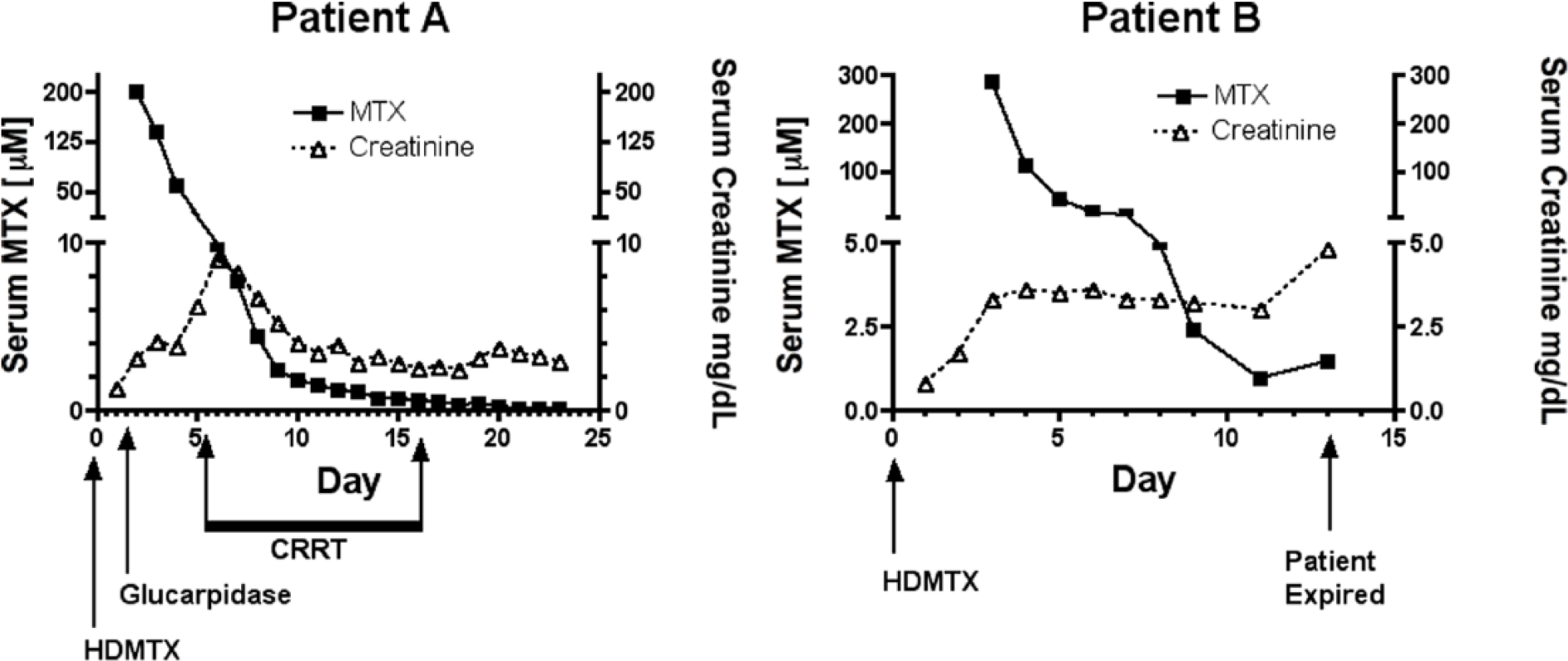
High-dose methotrexate (HDMTX) therapy outcomes. Patient A (left panel) has developed anuric acute kidney injury after HDMTX. However, he has recovered renal function with supportive care that included glucarpidase administration and continuous renal replacement therapy (CRRT). Patient B (right panel) has developed HDMTX-induced AKI that was milder and non-oliguric; however, later died due to complications of severe sepsis.
Intermittent HD was performed 1 day after the HDMTX to facilitate MTX clearance as well as management of emerging AKI complications and the patient was transferred to the intensive care unit for close monitoring. However, a standard 4-h intermittent HD treatment decreased MTX levels to 139.4 µM/L (a 30.73% reduction), and 60 µM by day 3 post-HDMTX. At that time, continuous renal replacement therapy (CRRT) was initiated and glucarpidase (BTG International, Inc.) was administered intravenously at the recommended dose of 50 U/kg. The decision was made to use CRRT based on the patient developing relative hypotension and our institutional practices for care of patients in the intensive care unit. Post-glucarpidase MTX levels were 9.92 µM (an 83.5% reduction). CRRT was held for 3 days after glucarpidase administration, but was restarted and continued from day 6 to day 17 post-HDMTX to aid management of AKI complications. However, his urine output subsequently improved and renal function recovered to a serum creatinine of 1.6 on day 27 post-HDMTX (MTX level at that time was 0.07 µM). Similarly, he recovered from additional HDMTX complications that included myelosuppression, urinary tract infection, pulmonary edema, and mildly increased liver function tests.
Case B
A 55-year-old white male with newly diagnosed large B-cell lymphoma, otherwise unremarkable history and physical examination with the exception of borderline class 1 obesity (weight of 96 kg; BMI, 30.3). His baseline renal function was normal with a serum creatinine of 0.7 mg/dL. He received HDMTX at intravenous dose 8 g/m2 (total 17 g) without any additional chemotherapy. Standard supportive HDMTX care included prophylactic intravenous fluids pre- and post-HDMTX administration and timely leucovorin rescue. However, his serum creatinine increased to 1.7 mg/dL on day 1 post-HDMTX. On day 2 post-HDMTX, the MTX level was 286.5 µM, intravenous fluids were continued, and leucovorin dose increased from 25 to 100 mg every 6 h. His creatinine peaked at 3.6 mg/dL on day 5 post-HDMTX and declined to 2.5 mg/dL by day 7 post-HDMTX. A renal ultrasound demonstrated normal-appearing kidneys without obstruction. However, he also developed HDMTX-induced myelotoxicity complicated by severe pancytopenia; for example, 9 days post-HDMTX white blood cell count declined to 370 per cubic millimeter (cmm), hemoglobin to 8.8 g/dL, and platelet count to 27,500 per cmm). In addition, on day 7 post-HDMTX, he developed septic shock with severe persistent hypotension and eventually become unresponsive to intravenous fluids or vasopressors. His AKI was thought to be secondary to HDMTX initially, with contribution of acute tubular necrosis from septic shock later in his clinical course. Due to the progressively worsening septic shock complications, intensive supportive care was discontinued on day 12 post-HDMTX and the patient died later that day.
Discussion
This case report demonstrates the importance of quickly identifying and treating the MTX toxicity. In addition, consistent with previous report, 4 it points to potential beneficial adjuvant effects of glucarpidase and high-flux HD therapy.
Risk factors predisposing to nephrotoxic complication of HDMTX are incompletely understood. Obesity, seen in both Patient A and Patient B, is among such risk factors since it delays MTX clearance. 5 Consequently, an alternative dosing regimen of HDMTX was suggested for obese patients.5,6–8 However, even 25% MTX dose reduction did not protect Patient A from developing HDMTX-induced anuric AKI.
The severity of AKI seen in Patient A represents an extremely rare example of severe HDMTX nephrotoxicity. This is only the second reported case of anuric AKI induced by HDMTX, 9 and the only case with a reported clinical outcome. For example, in a case series of patients with CNS lymphoma that were treated with HDMTX, nobody developed severe nephrotoxicity. 10 While the exact etiology of anuric AKI in Patient A is unknown, it is likely that it included obesity complications and reduction of renal reserve due to history of previous AKI, and Waldenstrom’s macroglobulinemia, a potential cause of renal insufficiency. Waldenstrom’s macroglobulinemia has been reported to cause AKI by IgM deposition in the glomerular basement membrane, as well as lymphoid cell infiltration of the interstitium. 11 He had no other easily identifiable HDMTX risk factors. 5
The limitations of this study include the MTX measurement method. Specifically, MTX levels were measured by automated fluorescence polarization immunoassay (FPI) and not by the more accurate high-performance liquid chromatography. Inactive metabolites of glucarpidase-mediated MTX degradation can cross-react with MTX when using FPI and likely led to falsely elevated post-glucarpidase MTX levels. Also, without biopsy confirmation, the cause of AKI is not definitive in both cases and could have been significantly impacted by factors unique to each of their hospital courses.
In summary, this case report points to the danger of HDMTX-induced nephrotoxicity, importance of its early recognition and initiation of effective therapy. We report the second case of HDMTX-induced anuric AKI, and this case is the first one with a reported clinical outcome. This report points to administration of glucarpidase as rapid effective treatment of HDMTX toxicity and supports the use of adjuvant therapy with extracorporeal removal such as high-flux HD and CRRT to improve MTX clearance in patients with severe AKI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.M. was supported in part by R01 DK097423; Hepato/Renal Fibrocystic Disease Core Center P30 DK074038, UAB-UCSD O’Brien Center 1P30 DK079337, and 1 I01 BX002985 from the Office of Research and Development, Medical Research Service, Department of Veterans Affairs. M.M. received research funding from Otsuka Pharmaceuticals and Genzyme.
Informed consent
Informed consent for patient information to be published in this article was not obtained because it was not possible for us to obtain consent for this case report from the two patients because they died 2 or 3 years ago. However, this case report meets all conditions for protection of individual data as specified by the Committee on Publication Ethics’ (COPE) Code of Conduct (see the Compliance with ethical standards section).