
Abstract
Despite being a known barrier to optimal breast-feeding indicators, the practice of Pre-lacteal Feeding (PLF) remains a key challenge in Bangladesh. This study examines the prevalence and underlying factors associated with PLF, for which data from a weighted sample of 4982 Bangladeshi mothers with children aged 0 to 36 months from the 2017-18 Bangladesh Demographic and Health Survey was used. Step-by-step multivariate logistic regression was performed to identify the association of significant determinants of PLF practices. Nearly 29% newborns received PLF before breastmilk and timely initiation of breastfeeding did not happen in case of 20.5% babies. The odds of PLF were significantly higher among the inhabitants of Dhaka division compared to other regions. In addition, birth-related factors such as optimal ANC visits (P < .01), home delivery (P < .01) and delivered by cesarean section (P < .01) showed significantly higher odds of introducing PLF to the newborns. Our results demonstrated the need for developing targeted policies and actions to prevent such practices of PLF in order to improve optimal breastfeeding behavior in Bangladesh.
Introduction
To maintain optimal health and nutritional status among children in a country, it is vital to improve their infant and young child feeding (IYCF) practices.1,2 Evidence from many low- and middle-income countries (LMICs) have shown significant association of IYCF practices with the nutritional status of children.3,4 Optimal breastfeeding practices such as the timely initiation of breastfeeding (ie, within 1 hour of birth) and Exclusive Breast Feeding (EBF) have been included as 2 crucial IYCF indicators because of their protective impact on infant survival and well-being.5,6 EBF means giving a newborn no food or drink other than the breastmilk for the first 6 months of life. 7 EBF plays a pivotal role in decreasing many early-life diseases in infants, and helps with their optimal growth and development. 8 Moreover, EBF is cost-effective 9 and have beneficial health effects for the mothers as well. 10 Also, to ensure that the newborn receives “colostrum” (ie, a nutrient-rich fluid produced by the mother immediately after giving birth), it is vital that the initiation of breastfeeding is done within 1 hour of birth. 11 Colostrum contains immune, growth and tissue repair factors which helps to develop newborn immunity. 12 Timely initiation of breastfeeding thus assists in preventing newborn deaths by reducing risk of infection and improving their nutritional status.13,14 However, introduction of pre-lacteal feeding to a newborn interferes with both the timely initiation of breastfeeding and the process of EBF; thereby, leading to suboptimal breastfeeding practices.15,16
Pre-lacteal feeding (PLF) refers to the provision of any food or drink other than the breastmilk/ colostrum to a newborn within first 3 days of birth before initiating breastfeeding; and these foods/drinks are known as “pre-lacteals.”17-19 Some common pre-lacteals are honey, sugar, sugar-juice, ghee (refined butter), cow’s milk, plain water, infant formula, rose water etc.20,21 These are often provided due to various misconceptions among people such as it helps clear the babies’ throat/bowel or the colostrum is too heavy for the newborn to digest etc. 22 Despite having insignificant nutrient and immunological values and bearing the risk of introducing contaminants in the newborn, giving pre-lacteal feeding remains a major cultural practice in the South Asian countries including Bangladesh.23-25
Regardless of introducing the national strategy for IYCF in 2007 with support from WHO and UNICEF, 26 improper breastfeeding practices including pre-lacteal feeding continue to pose a challenge for Bangladesh till this date. Previous data has shown the prevalence of pre-lacteal feeding in Bangladesh to be 27%. Furthermore, 49% and 45% of their newborns did not receive early initiation of breastfeeding and exclusive breastfeeding respectively, 27 which created substantial risks for the health and well-being of the neonates and children of the country. Such practices of sub-optimal breast feeding are concerning owing to their association with increased neonatal morbidity and mortality in many countries, which is evident by the fact that 47% of all under-five deaths across the world occur during the first month of their lives (ie, neonatal period). 28
Therefore, it is imperative to establish optimal breastfeeding practices like early initiation of breastmilk and EBF to prevent early-diseases and deaths among the newborns in Bangladesh. However, despite having such negative impact on the optimal breastfeeding practices, the available resources on pre-lacteal feeding in the country remains quite scarce. This research was therefore conducted using nationally representative data with the aim to explore the prevalence and underlying factors associated with pre-lacteal feeding practices among mothers having children aged 0 to 36 months in Bangladesh. The findings from this study will help develop policies and actions necessary to prevent the incidences of pre-lacteal feeding in the communities; thus, improving optimal breastfeeding practices like timely initiation and exclusive breastfeeding across the country.
Methodology
Data Sources
This study used secondary data drawn from the latest nationally representative cross-sectional household survey, Bangladesh Demographic and Health Survey (BDHS), 2017-18. The survey collected data on demographic characteristics, health indicators and biomarkers from all the 8 administrative divisions of Bangladesh. The detailed methods of sampling technique and data collection instruments have been described elsewhere. 29
Population and Sample Size
A total of 20 127 ever married women of 15 to 49 years were interviewed during the survey. For our research, data were extracted for all the mothers who had child birth in the last 3 years prior to the survey. In the cases of women with a history of giving more than one live birth preceding the 3 years of the survey, data regarding the most recent live birth were collected only and that made the total number of samples to be 5051. However, considering the outcome variable of this study, the missing values were disregarded and finally, a weighted sample of 4982 mothers with a children of 0 to 36 months of age were included for the analysis.
Study Variables
Dependent variable
Pre-lacteal feeding was the outcome variable of this study. The mothers were asked one question to assess if the child was provided with any pre-lacteal feeds: ‘In the first 3 days after delivery, was the child given anything to drink other than the breast milk?’ Based on the answer, the variable was coded as 1 = provided pre-lacteal feeding, and 0 = did not provide any pre-lacteal feeding.
Independent variables
This study included division, place of residence (urban and rural), mother’s age (15-19, 20-24, 25-29, 30-49 years), mother’s education (no education, primary education, secondary education and higher education), mother’s occupation (categorized as not working/home maker, agriculture related employment, professional employment) and sex of the child (male and female) as independent variables. In addition, access to media was recorded as frequency of reading newspaper, listening to radio, and watching TV (categorized as “Yes” if they had access to any one these medias at least once in a week; and “No” otherwise). Moreover, wealth index of the participants was categorized as “poorest,” “poorer,” “middle,” “richer,” and “richest” using the principal component analysis. 1
Additionally, the number of antenatal care (ANC) visit was categorized into no visit, 1 to 3 visits and 4 or more visits; mode of delivery was categorized as normal vaginal delivery (NVD) and cesarean section; and “home” and “health facility” were labeled to indicate the place of delivery. If breastfeeding initiation occurred within 1 hour of delivery, then the timing of breastfeeding initiation was categorized as timely; otherwise, it was categorized as late. Birth weight of the child was categorized into 3 groups as low (<2500 g), average or more (≥2500 g), and not weighted at the time of birth.
Statistical Analysis
All the extracted data were weighted to make the sample representative. STATA version 14.1 was used to perform the analysis. In order to explore the association of pre-lacteal feeding practices among the mothers with the socio-demographic characteristics and other explanatory variables, a logistic regression model was employed.
Binary logistic regression was employed first; from where the significant variables (P-value less than or equal .05) were fitted into a multivariable logistic regression model to identify the influencing factors of pre-lacteal feeding practices among mothers with children aged 0 to 36 months. The findings were presented in terms of adjusted odds ratios (aOR) with 95% confidence interval (CI) and statistical significance was considered at a P-value of <.05 in all analyses.
Results
Socio-Demographic and Economic Characteristics of the Participants
The key socio-demographic and economic characteristics of the 4982 participants has been presented in Table 1. Among the 8 divisional cities of Bangladesh, majority (25.5%) participants were from Dhaka division, while Barisal division had the lowest number of respondents (5.7%). Almost 73% respondents lived in rural areas and nearly 61% were homemakers. Age of about 61% mothers were in between 20 and 29 years, and only 18% mothers were 15 to 19 years old. 6.3% mothers did not receive any education, whereas 49.1% had secondary level education. Distribution of respondents were almost equal across the wealth quintiles as evident by the presence of approximately 20% participants in each group. Nearly 66% mothers had access to some form of mass media platform (TV/Radio/Newspaper) and about 52% gave birth to a male child.
Socio-Demographic and Economic Characteristics of Mothers of Children Aged 36 Months or Less in Bangladesh [BDHS, 2017-18].

Breastfeeding Practices and Birth Related Factors
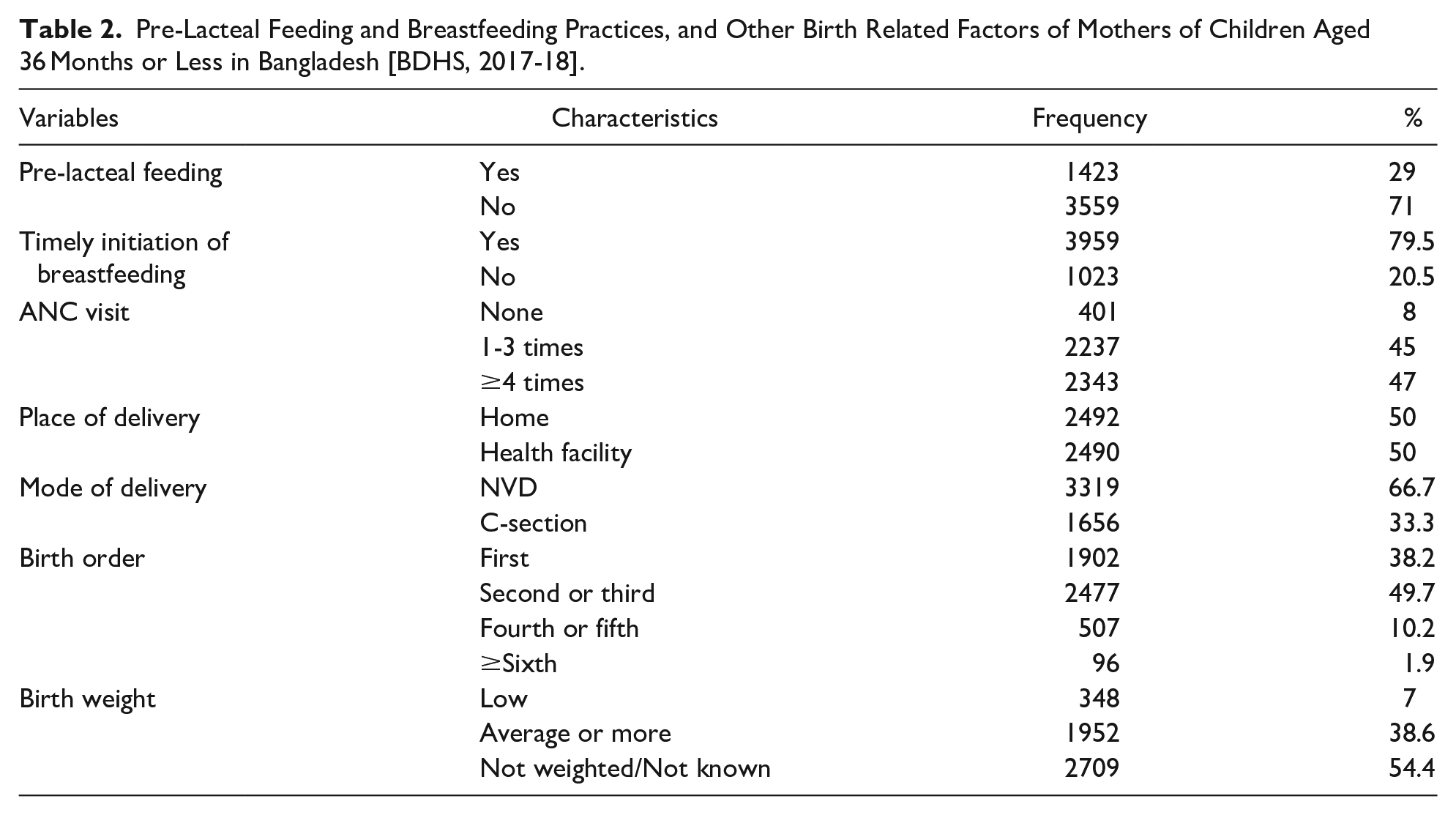
Out of the 4982 participant mothers, 29% reported giving pre-lacteal feeds to their newborns, while 71% did not. Nearly 79.5% of the mothers reported initiating breastfeeding to their newborns in time. When inquiring about the number of ANC visits during their pregnancies, only 8% stated that they did not go for any ANC visit, whereas 47% took 4 or more visits. Half of the participants had the delivery of their child at home and about 67% mothers had normal vaginal delivery (NVD). Majority (54.4%) of respondents did not know the birth weight of their newborn. Among the rest who knew about the birth weight, 38.6% reported of average or more weight at birth for their babies (see Table 2).
Pre-Lacteal Feeding and Breastfeeding Practices, and Other Birth Related Factors of Mothers of Children Aged 36 Months or Less in Bangladesh [BDHS, 2017-18].
Factors Associated With Pre-Lacteal Feeding Practices
Table 3 shows the results from the bivariate analysis of factors associated with pre-lacteal feeding practices among our respondent mothers who had children aged 0 to 36 months. Among the socio-demographic and economic factors, significant association (ie, P-value <.05) of PLF practices were found with the divisional city where the mother and child lived in, maternal age, wealth index, and access to mass media. The prevalence of PLF practices were significantly lower among those living in Barisal (cOR = 0.51; CI = 0.38, 0.69), Chittagong (cOR = 0.42; CI = 0.35, 0.51), Rangpur (cOR = 0.53; CI = 0.42, 0.67), Sylhet (cOR = 0.26; CI = 0.19, 0.35), and Mymensingh (cOR = 0.74; CI = 0.58, 0.94) divisions compared to the capital of the country, Dhaka division. The odds of introducing PLF was 17% less likely among mothers in the age group of 25-29 (cOR = 0.83; CI = 0.69, 1.00) compared to the younger mothers aged 15 to 19 years. Mothers from the richer quintile (cOR = 1.18; CI = 0.97, 1.43) were more likely to give pre-lacteals to their newborn compared to the poorest quintile. Also, participants with access to any form of mass media showed 1.21 times higher odds of practicing PLF (cOR = 1.21; CI = 1.06, 1.38) than those with no access to media.
Bivariate Analysis of Pre-Lacteal Feeding Practices Among Mothers of Children Aged 0 to 36 months in Bangladesh, [BDHS, 2017-18].

Abbreviations: cOR, crude odds ratio; CI, confidence interval.
P < .1. **P < .05. ***P < .01.
Significant associations were also found between some breastfeeding and birth related factors, and the PLF practices among the mothers. For instance, not initiating breastfeeding timely (cOR = 3.29; CI = 2.85, 3.80), not having any ANC visits (cOR = 1.21; CI = 0.97, 1.52), delivery at home (cOR = 1.17; CI = 1.03, 1.32), delivery by cesarean section (cOR = 1.63; CI = 1.44, 1.85) and delivery of first child (cOR = 1.52; CI = 0.93, 2.48) were found to be significantly associated with pre-lacteal feeding practices at P-value of <.05 (Table 3).
Consequently, the step-by-step multivariate logistic regression was performed to understand the independent factors responsible for pre-lacteal feeding practices and Table 4 presents the findings from the analysis. After controlling for the effect of non-significant variables, the odds of pre-lacteal feeding were found to be significantly lower among those living in Barisal (aOR = 0.49; CI = 0.36, 0.67), Chittagong (aOR = 0.37; CI = 0.30, 0.67), Rangpur (aOR = 0.56; CI = 0.44, 0.72), Sylhet (aOR = 0.24; CI = 0.17, 0.34) and Mymensingh (aOR = 0.76; CI = 0.60, 0.97) compared to Dhaka division. Participants who did not timely initiate breastfeeding had 3.42 times higher odds (aOR = 3.42; CI = 2.93, 3.99) of giving pre-lacteal feeding to their newborns compared to the others. The odds of introduction of prelacteals were significantly high among mothers who had no ANC visits (aOR = 1.66; CI = 1.28, 2.14), and 1-3 ANC visits (AOR = 1.21; CI = 1.05, 1.40). Mothers who had delivery at home (aOR = 1.57; CI = 1.28, 1.93), and by cesarean section (aOR = 1.69; CI = 1.37, 2.09) also showed significantly higher odds of introducing pre-lacteal feeding to their newborns compared to the other groups.
Multivariate Analysis of Pre-Lacteal Feeding Practices Among Mothers of Children Aged 0 to 36 Months in Bangladesh, [BDHS, 2017-18].

Abbreviations: aOR: adjusted odds ratio; CI: confidence interval.
**P < .05. ***P < .01.
Discussion
Providing pre-lacteal feeding to the newborn hinders the process of optimal breastfeeding by delaying the initiation of breastfeeding and nullifying the concept of EBF (which warrants the notion of giving nothing but breastmilk to babies for the first 6 months after birth). Nevertheless, the custom of giving PLF to the newborns is widely practiced in many parts of Bangladesh which can be attributed to several underlying factors. Our study attempted to identify the factors which led to the practice of PLF among the mothers in the country.
During our analysis of BDHS 2017-18 data, we found the prevalence of pre-lacteal feeding to be 29% which is slightly higher than the prevalence reported during BDHS 2014 (27%). This rising prevalence over the years is indicative of the continuance of PLF practices among a substantial number of mothers in the country. However, this prevalence is lower compared to some other LMICs such as Pakistan (64.7%), 30 Vietnam (73.3%), 31 Indonesia (45%), 32 and Nigeria (59%); 33 whereas countries like Nepal (26.5%), 21 India (21%), 34 and Ethiopia (8%) 35 reported even lower prevalence of PLF than Bangladesh. Such variations in PLF practices among different LMICs is possibly a reflection of the country specific socio-cultural norms and beliefs; availability and utilization of maternal and child healthcare services; level of knowledge and education regarding the importance of optimal breastfeeding practices etc. 36
From our analysis, it was observed that compared to the capital division of Dhaka, most of the other divisions had significantly lower prevalence of PLF practices. Similar to the variance of PLF practices between countries, such within-country regional variation of pre-lacteal feeding could also be attributed to the variety in socio-cultural and economic norms across communities within the country. One study conducted in Ethiopia also reported regional differences to be a significant factor in initiating pre-lacteal feeds among children, and pointed out the disparities in access and distribution to healthcare services, information, resources and geography as the contributing factors behind such regional variations of PLF. 35
Additionally, not initiating timely breastfeeding was found to have significant association with PLF practices among our participants. This relationship of delayed initiation of breastfeeding with provision of pre-lacteal feeding has been evident by other studies as well.23,37,38 Misconceptions regarding colostrum and early breastfeeding, post-cesarean physical difficulties of mother, insufficient breastmilk production, and the customary practice of providing pre-lacteal feeds to a newborn have been reported to be some key reasons resulting in the delayed initiation of breastfeeding.39,40 Such delayed initiation of breastfeeding has been repeatedly discouraged by multiple studies as it has often found to be interlinked with the use of alternative foods (other than breastmilk) for the babies during the first 6 months of life; thereby hindering the process of EBF.41,42
Our participants who had none, or less than 4 antenatal check-ups were also more likely to give pre-lacteal feeds to their babies than those who completed 4 or more ANC visits. These findings resonate with evidence from other South Asian countries such as India, Nepal and Sri Lanka where inadequate numbers of antenatal appointments have also been reported to be an obstacle toward timely initiation of breastfeeding.43-46 Completing the full schedule of ANC visits carries immense significance as they are designed to positively influence optimal breastfeeding practices among the mothers. Therefore, mothers who completed 4 or more ANC visits were more likely to have developed the awareness regarding the harmful effect of PLF along with the significance of early initiation of breastfeeding in newborns.
In addition, women who had their childbirth at home showed higher odds of giving pre-lacteals to their newborns compared to those having delivery at healthcare facilities in our analysis. These findings are supported by other studies which have shown that women having home delivery are more likely to give pre-lacteal feeds to their children.47,48 One possible reason behind this could be that home deliveries are usually assisted by traditional birth attendants or midwives who can negatively influence the decision of mothers regarding early breastfeeding. A previous Bangladeshi study corroborates our findings in this regard and reported that midwives who assisted the home deliveries discouraged the mothers to breastfed their children for the first 3 days after birth. 49 Moreover, home deliveries are often accompanied/assisted by family members and friends whose misconceptions or advices regarding breastfeeding based on personal experiences and hearsay evidence may also influence the mother’s decision of giving pre-lacteal feeds to the baby which has been validated by an Indian study. 44 On the other hand, those who had institutional delivery reportedly received professional advice and counseling from their healthcare providers regarding optimal breastfeeding practices which prohibited them from giving pre-lacteal feeding to their children.50,51
In our study, participants who had cesarean section delivery also showed higher odds of PLF practices compared to those having normal vaginal delivery (NVD) which is similar to the findings from some previous studies. 52 In such cases, postoperative pain, effect of anesthesia and insufficiency of breast milk reportedly led to the delayed initiation of breastfeeding followed by the introduction of PLF to cover the feeding needs of the baby. 53 Furthermore, receiving antibiotics and analgesics drugs during post-cesarean period created concerns among mothers regarding the passage of these medicines to their children via breastmilk which often discouraged them to breastfeed. 54
Apart from these factors, being a teenage mother (15-19 years old), belonging to a richer wealth quintile, not having access to any form of mass media, and primiparity/delivery of first child were also found to have association with the practice of PLF among our respondents. However, after controlling for effects of other variables during multivariate analysis, these factors did not show significant association with PLF anymore. Also, no significant association of PLF was found with mother’s age, education and occupation which suggests that the role of traditional beliefs and customs play a more important role in women’s decision-making regarding PLF practices irrespective of their own educational and economics status and exposure to mass media. In a previous study, introduction of pre-lacteal feeding has been shown to be associated with suboptimal breastfeeding practices (such as the delayed initiation of breastfeeding in children) even when the neonate was able to suck breastmilk normally and there were no other issues which would prevent the mother from initiating breastfeeding. 55 The findings of this study showed how traditional beliefs and socio-cultural prejudice justified the provision of PLF to newborns without any specific medical reasons. The customary influence of elderlies/mothers-in-laws, and the role of social and religious traditions in decision-making regarding the pre-lacteal feeding and breastfeeding practices have also been stated to influence the suboptimal breastfeeding practices in the communities by several studies conducted in Bangladesh and other countries.49,56,57 For example, the belief that colostrum is dirty and harmful for the baby as it was stored in the breast for 9 months was found to be a common misconception in neighboring countries of Pakistan and India which lead to the discarding of colostrum followed by introduction of PLF in newborns. 58
From the findings of our analysis, it is evident that there are some crucial risk factors responsible for the practice of PLF among Bangladeshi mothers. Lack of knowledge and the deeply embedded socio-cultural norms seemed to be one of the root causes behind such practice in the country. Therefore, well-designed and targeted awareness campaigns need to be developed and implemented across the country to promote optimal breastfeeding behavior and prevent PLF practices in the society. In addition, having access to and utilizing proper maternal healthcare services during pregnancy can impose a significant impact on mother’s decision making regarding optimal breastfeeding practices. 35 Hence, access to and utilization of ANC services and institutional delivery in the presence of skilled healthcare professionals need to be insured so that proper counseling and care to the mothers can be given regarding PLF practices during pregnancy and childbirth. In cases of women having cesarean delivery, it is crucial to make them aware of the fact that there are no contradictions against early initiation of breastfeeding for mothers who undergo operative delivery. Having this knowledge can help change the practices of PLF by enabling women who undergo cesarean delivery to begin breastfeeding their newborns as early as possible. 59
Strengths and Limitations of the Study
The strength of this study lies in its use of data obtained from the recent nationwide survey which increases the representativeness of the study. However, this study may suffer from recall bias since the responses were self-reported by the participants. Also, the cross-sectional design of the study limits its ability to draw any causal inferences. Despite these limitations, the current study does provide crucial findings which can be used to design interventions to remove the determinants of PLF practices in Bangladesh.
Conclusion
To persuade people away from suboptimal breastfeeding practices in Bangladesh, awareness campaigns and promotional messages should be designed based on a clear understanding of the traditional beliefs and customs of each particular area or groups of population. Involving the influential societal figures such as religious leaders for the promotion of EBF and dissuasion of PLF practices can be a useful way to eliminate the prejudice and misconception regarding the issue. Furthermore, use of participatory health promotion techniques such as exclusive breast-feeding support group for women in the community has been proven to be successful in reducing pre-lacteal feeding practices in other countries, 60 and it can be applied for Bangladeshi women as well, especially to those living in rural and remote areas with limited access to correct information. Finally, ANC facilities should be made easily available in all regions/divisions of the country, and interventions should be designed to encourage women to complete the full schedule of their ANC visits so that they can receive proper counseling and advice regarding optimal breastfeeding practices.
Footnotes
Acknowledgements
We are grateful to Measure DHS for allowing us access to the 2017-18 DHS dataset for Bangladesh.
Author Contributions
Both authors conceptualized and designed the study together. They were involved in the data analysis, interpretation and writing of the manuscript. Finally, they both critically read and reviewed the manuscript before giving final approval for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The authors declare that the research work meets the ethical guidelines.
Informed Consent
In the original survey, written informed consent was obtained from all subjects before the study.