
Abstract
Background:
Pre-lacteal feeding is associated with infant morbidity and mortality especially during the neonatal period. About 96% infant deaths in developing countries are attributable to inappropriate feeding practice during the first 6 months of life. This study assessed determinants of pre-lacteal feeding practices in Ethiopia using the data from nationally representative survey.
Methods:
Data were extracted from the 2016 Ethiopian Demographic and Health Survey to assess determinants of pre-lacteal feeding practices in Ethiopia. The analysis included a weighted sample of 5303 mothers having children aged 0–36 months. A multivariable logistic regression analysis was conducted and the results were presented with adjusted odds ratio at 95% confidence interval, declaring statistical significance at a p-value < 0.05 in all analyses.
Results:
From a total of 5303 mothers having children aged 0–36 months, 423 (8%, 95% confidence interval, 7.06%, 8.99%) had given pre-lacteal foods to their newborn baby. Being from agrarian region (adjusted odds ratio = 0.15, 95% confidence interval, 0.11, 0.20), poorest wealth status (adjusted odds ratio = 1.50, 95% confidence interval, 1.02, 2.22), home delivery (adjusted odds ratio = 1.35, 95% confidence interval, 1.01, 1.79), late initiation of breast feeding (adjusted odds ratio = 4.52, 95% confidence interval, 3.62, 5.64), having no counseling on breast feeding (adjusted odds ratio = 1.33, 95% confidence interval, 1.01, 1.75), and cesarean delivery (adjusted odds ratio = 2.47, 95% confidence interval, 1.45, 4.20) were factors significantly associated with pre-lacteal feeding practice.
Conclusion:
A significant proportion of Ethiopian mothers had given pre-lacteal foods to their newborn babies. Poorest wealth index, region, late initiation of breast feeding, not counseled on breast feeding, home delivery, and cesarean delivery were identified as determinants of pre-lacteal feeding. Thus, emphasis should be given to improve mothers’ Infant and Young Child Feeding practice through counseling and utilization of institutional delivery. Moreover, special attention should be given to mothers from pastoralist regions and poor socio-economic status to reduce pre-lacteal feeding practice.
Introduction
Exclusive breastfeeding (EBF) given to newborn from birth through 6 months of age has long-term health and emotional benefits for both child and mother and is related with lower neonatal morbidity and mortality. Proper breastfeeding contributes in increased cognitive and physical development and also has contraceptive importance for mother.1–4 Furthermore, provision of mother’s breast milk to newborns within 1 h of birth ensures that the neonates receives colostrum which is rich in immunoglobulin (Ig) for passive immunity, hormones, and nutrients that a baby needs to thrive.2,4–6 Improving breastfeeding rates around the world could save the lives of more than 820,000 children under age 5 every year, the majority (87%) under 6 months of age. 7
Pre-lacteal feeding is associated with increased mortality, serious morbidity, and other long-term adverse health outcomes; however, efforts at national level to minimize pre-lacteal feeding had only modest effect. 4 In 2017, about 59% of infants aged less than 6 months globally had given pre-lacteal feedings.3,6 In Ethiopia, its prevalence ranges from 6.1% to 75.8%.8–13 Pre-lacteal feeds are of any solid, semisolid, or liquid food other than breast milk given to newborns before breast feeding is established or within 3 days after delivery. 14 The commonest pre-lacteals given by Ethiopian women are butter, plain water, cow milk, sugar with water, and formula milk.8–13,15
Global risk assessment of suboptimal breastfeeding indicates that 96% of all infant deaths in developing countries are attributable to inappropriate feeding occurring during the first 6 months of life. 16 Pre-lacteal feeds interfering with EBF delays breast feeding initiation, disrupts the mother-baby bonding, interfering with sucking, and can also cause allergy to the infant. Moreover, pre-lacteal feeding exposes the baby to risk of infection, pneumonia, diarrhea, meningitis, HIV transmission, ear infections, and have fewer nutrients which lead to child malnutrition.1,12,13,17 In 2016, from a total of 667 million under five children, 155 million and 52 million were stunted and wasted, respectively, across the globe; of this, 59 million stunted and 14 million wasted were from Africa.1,5,18
Many studies documented that maternal age, place of residence, parity, antenatal care, wealth index regions, occupation, educational status, sex of child, place of delivery, and poor feeding knowledge associated with pre-lacteal feeding practices.8–11,13,17,19–22 In addition, mode of delivery, counseling on breast feeding, late initiation of breastfeeding, and colostrum avoidance8,9,11,13,17,21,22 were found to be factors associated with pre-lacteal feeding.
Since 2004, Ethiopia has been implementing the Infant and Young Child Feeding (IYCF) strategy as a key component of child survival approach. 23 However, suboptimal breast feeding practices including pre-lacteal feeding has been continued as challenges. In the past two decades, though there is reduction of child mortality in Ethiopia, half of the prevailing mortality happens during neonatal period.24,25 Thus, investigating the burden and determinants of this problem is vital to promote implementation of IYCF thereby reducing neonatal mortality. Moreover, understanding of factors associated with pre-lacteal feeding is important in the promotion of early initiation of breast feeding and EBF.
In Ethiopia, studies have been conducted assessing pre-lacteal feeding practices. However, these studies are conducted at pocket level and also show variations in prevalence and determinant factors.11,20,26,27 Therefore, this study assessed the prevalence and determinants of pre-lacteal feeding in Ethiopia using nationally representative data which covers the nine regions and two city administrations.
Methods
Data sources
The data were extracted from the 2016 Ethiopian Demographic and Health Survey (EDHS), a nationally representative survey that collected data on basic health, demographic, and socio-economic indicators. The Central Statistical Agency (CSA) together with the Ministry of Health (MoH) and the Ethiopian Public Health Institute conducted the survey from 18 January 2016 to 27 June 2016 and The United States Agency for International Development (USAID) funded the survey. 28
Population and sample size
Among 16,583 eligible women, the interview was completed for 15,683 women (15–49 years) across the nine administrative regions and two city administrations. 28 We extracted data for all mothers who had child birth in the last 3 years prior to the survey, and a weighted sample of 5303 mothers with a children of 0–36 months age were included in the study for the purpose of this analysis. Details about the DHS sampling techniques and sample size are available at http://www.dhsprogram.com/. The EDHS research protocol complies with the National Health Research Ethics Committee and Institutional Review Board guidelines.
Study variables
Dependent variable
The outcome variable was pre-lacteal feeds. The mothers were asked two questions to assess if the child was provided with any pre-lacteal feeds: In the first 3 days after delivery, was the child given anything to drink other than breast milk? What was the child given to drink? (Options were milk (other than breast milk); plain water; sugar or glucose water, gripe water, sugar salt water solution; fruit juice; baby formula; tea infusion; coffee, honey; and others). The main outcome variable (provided pre-lacteal feeds = 1 and did not provide pre-lacteal feeds = 0) was derived from the response to the first question. The types of pre-lacteal feeds were reported as a frequency.
Independent variables
This study included place of residence (urban and rural), religion, maternal education (no education, primary education, secondary, and higher education), age of the mother (15–24, 25–34, 35–49 years), sex of the child (male, female), and access to media was recorded as frequency of reading newspaper, listening to radio and watching TV (categorized as Yes or No). The number of antenatal clinic (ANC) visits was also categorized into no ANC visits, one to three ANC visits, and four or more ANC visits. Counseling on breast feeding (Yes or No), timing of breastfeeding initiation categorized as timely if initiated within 1 h of delivery and late if initiated after 1 h after delivery. Mode of delivery (vaginal or cesarean), and places of delivery (categorized as institutional or home). Number of children was also categorized into one child, two children, and three or more children.
The 11 regions of Ethiopia are delineated for administrative purposes, and in this study, they were categorized into three contextual regions: pastoralist, agrarian, and city (which were defined on the basis of the cultural and socio-economic backgrounds of their populations). 29
Household wealth is represented by wealth index (in five categories: poorest, poorer, middle, richer, and richest). Wealth index was constructed using data on a households’ ownership of selected assets, such as television and bicycles, materials used for housing construction, and types of water access and sanitation facilities. The index placed individual households on a continuous scale relative to their wealth status. 28
Statistical analysis
Extracted data were weighted so that the sample was representative of 15- to 49-year-old respondents in 2016 EDHS. Analyses were performed using STATA version 14. To assess the association between socio-demographic characteristics and other explanatory variables, and pre-lacteal feeding practices of mothers with children aged 0–36 months, a logistic regression model was employed.
First, each variable was entered into a binary logistic regression model. Second, variables which were significant at a p-value of less than or equal to 0.25 were fitted into a multivariable logistic regression model to identify independent factors of pre-lacteal feeding practices among mothers with children aged 0–36 months in Ethiopia. Statistical significance was declared at a p-value < 0.05 in all analyses. The results from the logistic regression analyses are presented as adjusted odds ratios (AORs) with 95% confidence intervals (CIs).
Results
Socio-demographic characteristics of the study participants
A total of 5303 of mothers were included in the analysis. The mean age of respondents were 28.39 (± SD 6.49) and ranged from 15 to 49 years. Majority (67.4%) of the mothers were in the 25–34 years age group. Three-fifth (62%) of the respondents had no formal education. Islam was the dominant religion accounting for 39.7%. Nine out of 10 (90.6%) were from agrarians region (Table 1).
Socio-demographic characteristics of mothers of children aged 36 months or less in Ethiopia, 2016.

Breastfeeding practices and obstetric factors
Of the total mothers, 423 (8%, 95% CI: 7.06%, 8.99%) gave pre-lacteal foods to their children. The most common pre-lacteal foods were plain water (56.5%) and powdered/cow milk (30.5%), Juice (8.1%), and baby formula (4.9%). More than four out of five (83.6%) had initiated breast feeding in less than 1 h. Less than half (42.9%) of the mothers had counseling on breast feeding. Two-thirds (31.5%) of the mothers had no antenatal care visit. Majority (64.3%) of the mothers were delivered at home. Almost all (97.6%) of the mothers were delivered through vaginal mode of delivery (Table 2).
Breastfeeding practices and obstetric factors among mothers of children aged 0–36 months or less in Ethiopia, 2016.

BF: breastfeeding; ANC: antenatal clinic.
Factors associated with pre-lacteal feeding practices
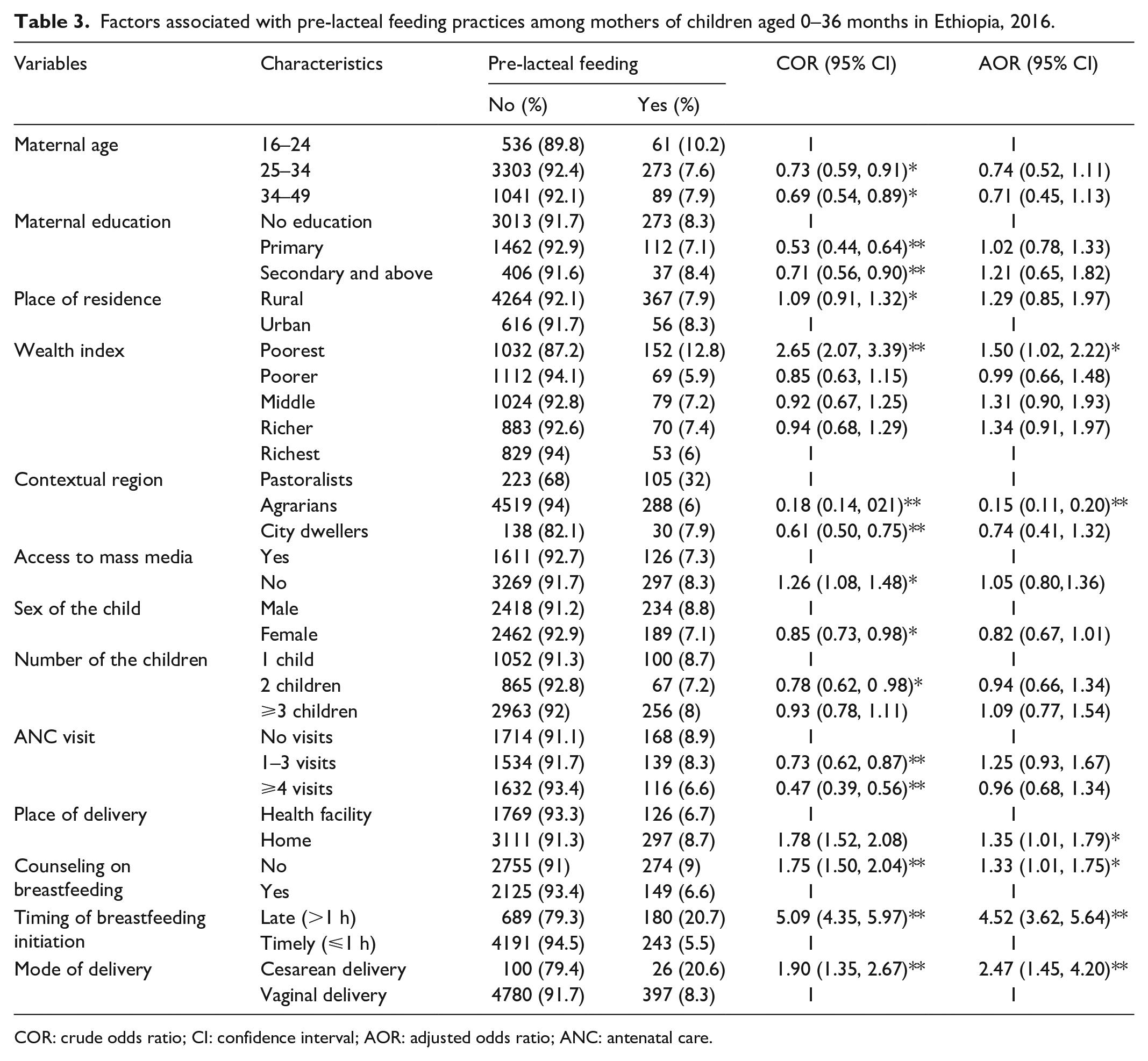
In bivariate analysis, maternal age, maternal education, place of residence, number of children, place of delivery, mode of delivery, counseling on breast feeding, breast feeding initiation, antenatal care, wealth index, regions, sex of the child, and access to mass media were associated with pre-lacteal feeding at p-value < 0.05.
In multivariate logistic regression analysis, the odds of pre-lacteal feeding practice was 1.5 times higher among mothers who were from the poorest wealth status compared to those from richest wealth status (AOR = 1.50, 95% CI, 1.02, 2.22). The odds of pre-lacteal feeding practice was reduced by 85% among mothers who were from the agrarians region compared to those from the pastoralist regions (AOR = 0.15, 95% CI, 0.11, 0.20).
The odds of pre-lacteal feeding practice was 1.35 times higher among mothers who had home delivery compared to those who had delivered at health facility (AOR = 1.35, 95% CI, 1.01, 1.79). The odds of pre-lacteal feeding practice was 1.33 times higher among mothers who had no counseling on breast feeding compared to those who had counseling on breast feeding (AOR = 1.33, 95% CI, 1.01, 1.75). The odds of pre-lacteal feeding practice was 4.52 times higher among mothers who lately initiated breast feeding compared to those who initiated the breast feeding early (AOR = 4.52, 95% CI = 3.62, 5.64). The odds of pre-lacteal feeding practice was 2.47 times higher among mothers who had cesarean delivery compared to those who had vaginal delivery (AOR = 2.47, 95% CI, 1.45, 4.20; see Table 3).
Factors associated with pre-lacteal feeding practices among mothers of children aged 0–36 months in Ethiopia, 2016.
COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; ANC: antenatal care.
Discussion
This study reveals that 8% (95% CI: 7.06%, 8.99%) of mothers gave pre-lacteal foods to their children. This proportion is comparable with findings from east Wollega zone (5.9%), 30 Ambo district (9.7%), 31 and Gonder town (8.2%) Ethiopia. 32 However, the current finding is lower than study results done in different parts of Ethiopia, 15% in Bahirdar city, 33 15.9% in Benishangul-gumuz region, 34 17.2% in Axum town, 35 and 16.8% in Debre birhan town. 36 The study results from low- and middle-income countries also report higher magnitude of pre-lacteal feeding, Nigeria (49.8% in urban and 66.4% in rural), 37 Kenya (26.8%), 38 in south Sudan (53%) 39 and in Himachal Pradesh, India (49.5%). 40 Such discordance may be linked with sample size, study design, and socio-economic and cultural variations.
In this study, we observed that poor wealth status is associated with pre-lacteal feeding practice. This is in consonance with study finding from northwest Ethiopia 20 and Mansur, Egypt. 41 This could be related with the fact that mothers with poor wealth status may not access health service and counseling from health care providers on infant feeding practice. Contrary to this, studies evidenced that being in poor wealth status is the preventive for pre-lacteal feeding. Because those in low socio-economic status could not afford the expensive pre-lacteal food like honey and ghee so the only available option to them is EBF. 14 Similarly, Parashar et al. reported that mothers with higher socio-economic status were more likely to give pre-lacteal food to their child. Even though butter and plain water are typically practiced in most low-income countries, those women of high socio-economic status may have the ability to pay and feed extra foods to their children. 40
Regional disparity on breastfeeding and newborn care practices could be in part a function of access to service, inequitable distribution of service, information, resources, and geographic variations. Our study finding established being from agrarian region is a preventive for pre-lacteal breast feeding compared to mothers from pastoralist area. This could be justified by the differences in ethnic composition of regions and their respective cultural practices that may have an impact on pre-lacteal feeding practices.
Mothers who gave birth at home were more likely to give pre-lacteal food for their new born child as compared to those who delivered at health facility. 30 This is supported by the study result from demographic and health survey data of Nigeria, where the odds of pre-lacteal feeding increase among mothers delivered at home. 37 Similarly, Bekele et al. 26 pointed out that mothers who deliver at home were more likely to give their child pre-lacteal feeding than mothers delivered at health facility. The reason for this could be the fact that mothers who gave a birth on the hands of health care providers were more likely to receive an advice and counseling on optimal infant and young child feeding.33,42 In addition, mothers who gave birth at health facility would have better ANC visits and antenatal counseling which includes proper breastfeeding practices and the risks associated with pre-lacteal feeds.
Evidences suggested that peer or providers’ counseling and social support are very effective to improve optimal breast feeding practice. 43 According to this study, mothers who have not received counseling from health care providers concerning the breast feeding were more likely to give pre-lacteal feeding for their children than those mothers who received appropriate counseling. In agreement to this, Nguyen and his colleagues found that counseling from health care providers and volunteers encourage the mothers to breastfeed their children. 44 Study finding from south Sudan also revealed that antenatal counseling on breast feeding decrease the odds of pre-lacteal feeding. 39 Post-natal counseling and advice for the mother concerning infant care is must to do intervention by health care providers. 45
Timing of breastfeeding initiation was found to be independent determinant of pre-lacteal feeding practices. Mothers who lately (after 1 h of delivery) initiated breastfeeding were more likely to practice pre-lacteal feedings. This result is supported by other study findings from Ethiopia. 12 There is a close relationship between early initiation and avoiding pre-lacteal feeds.
Our study finding showed that mode of delivery is important determinant of pre-lacteal feeding. The odds of pre-lacteal feeding practice among mothers delivered through cesarean section is higher compared to those mothers who gave birth through spontaneous vaginal delivery. This is consistent with findings from studies conducted in Uganda, 46 Egypt, 41 India, 47 and Vietnam. 44 This may be associated with the fact that mothers’ common concern that the antibiotics and other medications such as anti-pain and anesthesia that they receive during their perioperative care could harm their infants, which discourages them from breastfeeding. 48 In the post cesarean period, insufficiency of breast milk may also be a concern of mothers. In addition, the effect of anesthesia, the pain, and discomfort due to cesarean section may delay the early initiation of breast feeding and the family may provide an infant pre-lacteal feeding. 49
Strengths and limitations
The study utilized data from a nationwide survey, which could be considered as strength and could increase representativeness. However, this study may suffer from a recall bias as a pre-lacteal feeding practice was a self-reported event. The other limitation is that the cross-sectional study design cannot establish temporal relationship between the outcome and response variables.
Conclusion
In summary, about 1 out of 12 Ethiopian mothers had given pre-lacteal food to their newborn babies. Poorest wealth index, region, late initiation of breast feeding, not counseled on breast feeding, home delivery, and cesarean delivery were identified as determinants of pre-lacteal feeding. Thus, emphasis should be given to improve mothers’ Infant and Young Child Feeding (IYCF) practices through counseling focusing on optimum breastfeeding during antenatal care and delivery service. Improving utilization of institutional delivery would help to reduce the prevalence of pre-lacteal feeding. Mothers who delivered by cesarean section should also be counseled and supported to not give pre-lacteal feeds to her newborn baby. Moreover, strategies that consider disadvantaged population segments should be devised to reduce pre-lacteal practices of mothers from pastoralists regions and poor socio-economic status to reduce pre-lacteal feeding practice.
Footnotes
Acknowledgements
We would like to express our deepest gratitude to measure DHS, ICF International, Rockville, Maryland, USA, for providing the data for the analysis.
Author contributions
B.T.M. and B.B. initiated the research and drafted the manuscript, and the other authors contributed to the manuscript writing, data extraction, and analysis. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The original survey was conducted after being ethically approved by the National Research Ethics Review Committee (NRERC) of Ethiopia (Ref. No: 3.10/114/2016). Prior to analysis, we obtained permission from the Demographic and Health Survey program to access the dataset.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
In the original survey, written informed consent was obtained from all subjects before the study.
Data availability
All data analyzed are available from corresponding author up on reasonable request.