
Abstract
Diagnosing pneumonia and identifying those requiring antibiotherapy remain challenging. Chest radiographs (CXR) are often used as the reference standard. We aimed to describe clinical characteristics, host-response biomarkers and etiology, and assess their relationship to CXR findings in children with pneumonia in Thimphu, Bhutan. Children between 2 and 59 months hospitalized with WHO-defined pneumonia were prospectively enrolled and classified into radiological endpoint and non-endpoint pneumonia. Blood and nasopharyngeal washing were collected for microbiological analyses and plasma levels of 11 host-response biomarkers were measured. Among 149 children with readable CXR, 39 (26.2%) presented with endpoint pneumonia. Identification of respiratory viruses was common, with no significant differences by radiological outcomes. No clinical sign was suggestive of radiological pneumonia, but children with radiological pneumonia presented higher erythrocyte sedimentation rate, C-reactive protein and procalcitonin. Markers of endothelial and immune activation had little accuracy for the reliable identification of radiological pneumonia.
Introduction
Pneumonia causes 15.5% of all deaths among children under 5 years of age worldwide, translating to over 800 000 deaths annually.1,2 Early identification and treatment of children with pneumonia is fundamental to reduce mortality. 3 However, we lack diagnostic tools with high sensitivity and specificity that allow for accurate identification of children that require antibiotics, and at risk of poor prognosis.4-7 Initial evaluation of clinical pneumonia cases is important to identify those of presumed bacterial etiology since these cases may become life-threatening in the absence of appropriate antimicrobial treatment. Clinical diagnostic criteria for pneumonia, such as those proposed by the World Health Organization (WHO), primarily used in low- and middle-income countries, are highly sensitive, but are not able to discern children requiring antibiotics from those who will present a self-limited pneumonia with unnecessary antibiotics. This leads to an overtreatment of clinical pneumonia cases with antibiotics, with potential implications in the emergence of antimicrobial resistance.8,9 Although the accuracy of chest radiographs (CXR) for diagnosing pneumonia and differentiating between bacterial and viral etiology is imperfect, CXR have been traditionally considered the practical reference standard.10-13 Radiograph-based standardized endpoints are also commonly used in vaccine trials.7,13,14 More recently, a series of inflammatory host-response biomarkers have been described that may help differentiate between bacterial and viral etiologies. Their diagnostic role in childhood pneumonia remains unclear.15-17
Recent findings suggest that clinical signs and host-response biomarkers associated with radiological findings might differ according to geographic areas. 18 Indeed, predominant respiratory pathogens, co-infections such as malaria, and other factors such as altitude vary between geographical regions and are likely to contribute to these correlations.
We aimed to describe the radiological findings of children under 5 years of age admitted with WHO-defined pneumonia in the Respiratory Infections in Bhutanese Children (RIBhuC) study conducted in Thimphu, the capital of Bhutan, where data on childhood pneumonia are scarce. We looked at differences in radiological findings by demographic characteristics, etiology, clinical presentation, host-response biomarkers, evolution, and final outcome.
Materials and Methods
Setting and Participants
The RIBhuC study was conducted prospectively for 12 consecutive months at the Jigme Dorji Wangchuck National Referral Hospital (JDWNRH) in Thimphu, Bhutan, to describe the epidemiology, etiology, and clinico-radiological presentation of WHO-defined pneumonia among children under 5 years of age. 19 Briefly, all children aged 2 to 59 months admitted with a diagnosis of WHO-defined pneumonia were eligible for recruitment. 9 Children with history of cough or breathing difficulty were classified as having pneumonia if they presented with increased respiratory rate or chest indrawing, or severe pneumonia if they presented with oxygen saturation <90%, central cyanosis, severe respiratory distress or a WHO general danger sign. 9 We recruited all eligible children provided parent(s) or caregiver(s) consented on writing to study participation. The pneumococcal conjugated vaccine (PCV) was introduced in the country in January 2019, after the study period.
Data Collection
On admission, we assigned a study identification number, recorded vital signs and performed a comprehensive physical examination. Demographic and clinical data from the medical records and through family interviews were collected. Blood samples and a nasopharyngeal washing (NPW) specimen were collected upon enrollment or as soon as possible after enrollment. An antero-posterior CXR was performed within 24 hours of admission using either a digital machine (Model IDC DR. 1590x 3C, Eureka) or an analog one (Model KH/HD/STANDIX-31667, Siemens), depending on availability. Recruited children were clinically managed and discharged as per the criteria of the treating nurses and pediatricians and were followed-up by one study investigator in terms of outcome determination.
Chest Radiographs Interpretation
CXR were classified as confirmed “endpoint pneumonia” (consolidation, pleural effusion, or both on any hemithorax), “other infiltrates” (all others non-endpoint infiltrates in any hemithorax), or “normal” (no abnormalities identified). 14 “Non-endpoint pneumonia” comprised other infiltrates and normal CXR. See Supplemental Material Annex 1 for further details.
Biological Sample Testing and Laboratory Methods
Blood samples were collected for hematology, biochemistry, and culture, following standard procedures. 19
NPW samples were subjected to molecular analysis for identification of respiratory pathogens (multiplex real-time polymerase chain reaction [RT-PCR], QIAStat respiratory panel, Qiagen) and for detection and capsular typing of Streptococcus pneumoniae (RT-PCR, lytA gene).20-24 We considered the serotypes 1, 3, 4, 5, 7F, 14, 18C, and 19A as highly invasive. 20
On site rapid influenza diagnostic tests (Alere BinaxNOW®) were performed as per discretion of the treating clinicians and nurses, independently of the RIBhuC study.
Host-Response Biomarker Assays
Host-response biomarkers were measured blinded to patient clinical and radiological characteristics. White blood cell (WBC) count, platelets, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) were analyzed at the study center (JDWNRH). At the reference center (Sandra Rotman Centre for Global Health in Toronto, Canada), CRP and procalcitonin (PCT) were quantified by enzyme-linked immunosorbent assay (ELISA), and the plasma concentration of 6 additional endothelial and immune activation biomarkers were measured using a multiplex Luminex platform with reagents from R&D Systems (Minneapolis, MN): interleukin-6 (IL-6), interleukin-8 (IL-8), angiopoietin-2 (Angpt-2), soluble fms-like tyrosine kinase-1 (sFLT1), soluble triggering receptor expressed on myeloid cells 1 (sTREM-1), and soluble tumor necrosis factor receptor 1 (sTNFR1). 25 Biomarker concentrations outside of the detection limits were assigned a value of one third below or above the lowest or highest limit in the standard curve, respectively. We refer to CRP-study and CRP-ref for differentiating CRP measured at the study and reference laboratories, respectively.
Data Management and Statistical Analysis
Data were entered into a computerized password-protected database (ODK Aggregate version 1.4.13) with study identification number. 26 Errors in data entry were limited by using pre-defined ranges for every value. Stata™ v.16.0 (StataCorp, College Station, Texas, USA) was used for data analyses. 27 We examined the association between radiological outcomes and a set of variables (demographic and clinical characteristics, and biomarkers) using Chi-square or Fisher exact tests for categorical variables. Mann-Whitney U and Kruskal-Wallis tests were used for non-parametric continuous variables. Univariable logistic regression models were used to estimate odds ratios of radiological outcomes for predictors of clinical characteristics and biomarkers, and multivariable logistic regression models to estimate the degree of association between each biomarker and radiological findings after adjusting for observed confounders. All continuous variables with non-parametric distribution were log transformed for inclusion in logistic regression models. To assess the predictive capability of each biomarker considered, area under the curve (AUC) and other classification performance measures (sensitivity and specificity) were calculated. These calculations were performed based on each univariable logistic regression model and defining the cut-points using the Youden’s index method (J = max[sensitivity + specificity − 1]). Significance was set at .05.
Ethical Approval
The study protocol was approved by the Research Ethics Board of Health, Ministry of Health, in Thimphu, Bhutan (protocol number PO/2016/086), and by the research ethics committee from the Hospital Clínic in Barcelona, Spain (HCB/2017/0741).
Results
Between 1st July 2017 and 30th June 2018, 189 children were recruited. 19 CXR was performed to 94.2% (178/189) of them. CXR images were not available for external evaluation for 15.7% (28/178) of participants and one film was deemed uninterpretable. Therefore, 149 children were included in the analysis: 26.2% with endpoint pneumonia, 20.8% with other infiltrates, and 53.0% with normal radiological findings (Figure 1). Comparing children with (n = 149) and without (n = 40) CXR available, we found no differences in term of baseline characteristics (Supplemental Table 1).
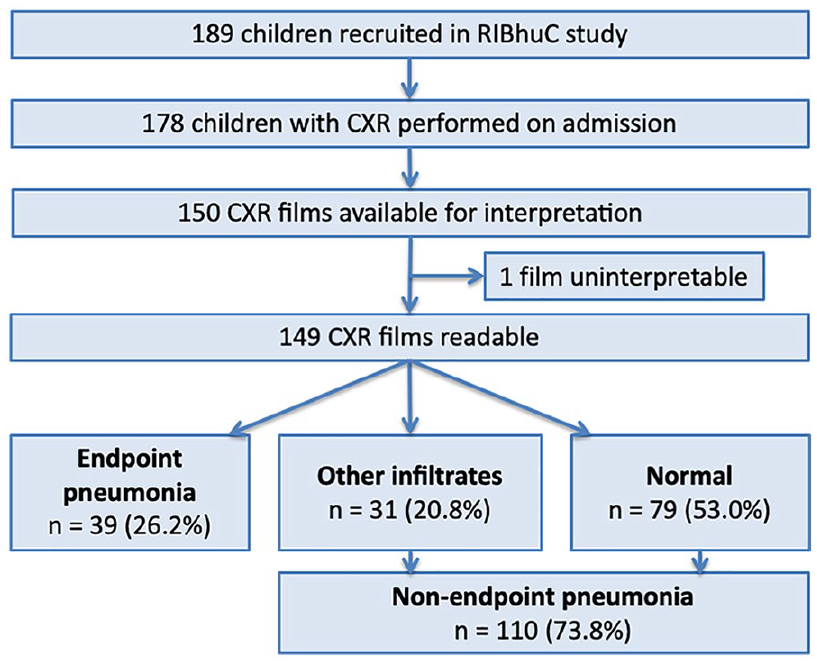
CXR interpretation and findings.
Missing demographic or clinical data were due to a lack of collection for these variables. Blood samples were collected and analyzed for WBC (148/149, 99.3%), platelet (146/149, 98.0%), CRP-study (143/149, 96.0%), ESR (131/149, 87.9%), and the remaining biomarkers at the reference center (96/149, 64.4%).
Children with radiological endpoint and non-endpoint pneumonia presented similar demographical characteristics in terms of age, gender, vaccine status, and parental education and employment (Table 1). However, there was a higher proportion of children with endpoint pneumonia that had an access time to health care facilities (proxy measurement of distance to the health system) of 30 minutes or longer (17.1% vs 2.8%, P = .008). Five children died, one with radiological endpoint pneumonia. A higher proportion of children with endpoint pneumonia required hospitalization for ≥5 days (48.7% vs 27.3%, P = .016), with no significant differences regarding the need of ventilation, oxygen therapy, or antibiotherapy. No additional differences were observed between the 3 radiological outcomes (endpoint pneumonia, other infiltrates and normal findings) (Supplemental Table 2).
Baseline Characteristics of Children With WHO-Defined Clinical Pneumonia for Radiological Endpoint Versus Non-Endpoint Pneumonia.
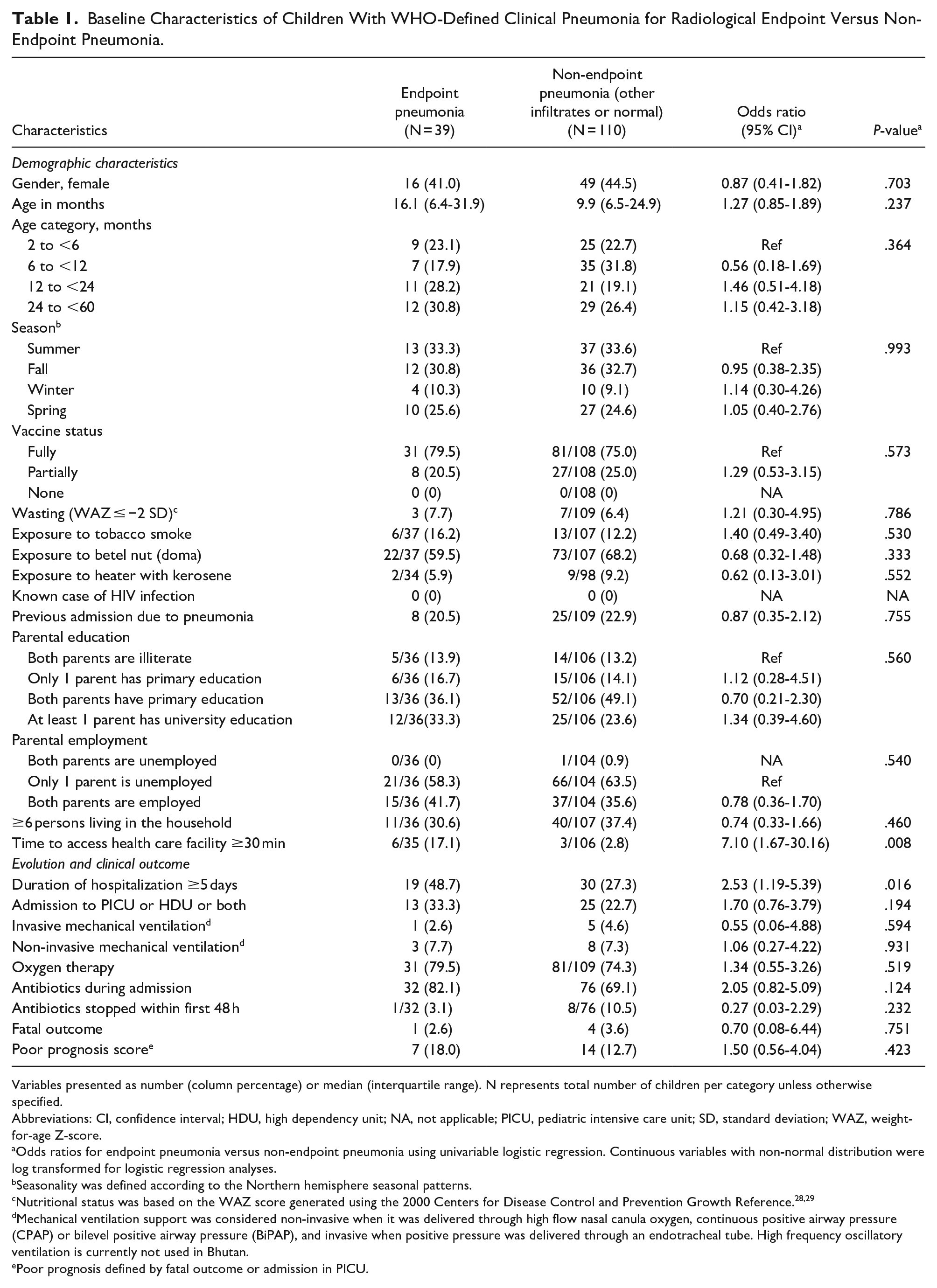
Variables presented as number (column percentage) or median (interquartile range). N represents total number of children per category unless otherwise specified.
Abbreviations: CI, confidence interval; HDU, high dependency unit; NA, not applicable; PICU, pediatric intensive care unit; SD, standard deviation; WAZ, weight-for-age Z-score.
Odds ratios for endpoint pneumonia versus non-endpoint pneumonia using univariable logistic regression. Continuous variables with non-normal distribution were log transformed for logistic regression analyses.
Seasonality was defined according to the Northern hemisphere seasonal patterns.
Nutritional status was based on the WAZ score generated using the 2000 Centers for Disease Control and Prevention Growth Reference.28,29
Mechanical ventilation support was considered non-invasive when it was delivered through high flow nasal canula oxygen, continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP), and invasive when positive pressure was delivered through an endotracheal tube. High frequency oscillatory ventilation is currently not used in Bhutan.
Poor prognosis defined by fatal outcome or admission in PICU.
Association of Etiology With Radiological Findings
Bacteria were isolated by blood culture in 6 children, 2/31 (6.5%) with endpoint pneumonia and 4/63 (6.4%) with normal CXR (Table 2). Detailed findings are published elsewhere. 19 There were no significant differences in the proportion of nasopharyngeal pneumococcal carriers and highly invasive serotype distribution between children with endpoint and non-endpoint pneumonia. At least 1 virus was detected in most children and a third of those had ≥2 viruses identified. All children with other infiltrates had at least 1 virus, and half of them had ≥2 viruses identified. Respiratory syncytial virus was the most commonly isolated virus (44.0%), detected in around 1-quarter of children with endpoint pneumonia and in half of those with non-endpoint pneumonia (P = .056). Rhinovirus was isolated in over half of children with other infiltrates and a third of those with endpoint pneumonia (P = .083). Parainfluenza virus was more frequent in children with endpoint pneumonia compared to those with non-endpoint pneumonia (28.6% vs 9.7%, P = .023; Supplemental Table 4). Other viruses were identified in similar proportion between children with different radiological endpoints.
Microbiological Investigations by Radiological Findings.

Variables presented as n/N (column percentage).
Abbreviations: CI, confidence interval; NA, not applicable; NPW, nasopharyngeal washing; OR, odd ratio; RT-PCR, real-time polymerase chain reaction.
Viral analysis was first performed in NPW samples. For some children, no NPW was left for pneumococcal analysis after viral analysis, explaining the lower number of children with pneumococcal results as compared to viral results.
Four children with endpoint pneumonia were positive for influenza A virus, and 1 child for both influenza A and B virus.
Two children with other infiltrates were positive for influenza A virus.
Five children with normal radiological findings were positive for influenza A virus, and 1 child for both influenza A and B virus.
Coronavirus-OC43 was identified in 1 child with endpoint pneumonia.
Coronavirus-NL63 was identified in 1 child with normal radiological findings.
P < .05 when comparing the proportions between endpoint pneumonia and other infiltrates, using univariable logistic regression (Supplemental Table 3).
P < .05 when comparing the proportions between endpoint pneumonia and non-endpoint pneumonia, using univariable logistic regression (Supplemental Table 4).
Association of Clinical Characteristics With Radiological Findings
A high proportion of children presented with clinical signs usually considered more indicative of radiological consolidation (endpoint pneumonia) as a proxy for bacterial pneumonia, including hypoxemia (79/108, 73.1%) or crackles (63/108, 58.3%), despite having CXR which did not confirm the pneumonia endpoint. Similar proportions of children with and without radiological pneumonia presented with increased work of breathing.
A higher proportion of children with endpoint pneumonia were symptomatic for at least 5 days prior to admission (64.1% vs 38.5%, P = .007), had fever for at least 5 days (42.1% vs 21.3%, P = .045), and presented with WHO severe pneumonia (92.3% vs 75.5%, P = .033) (Table 3). No single clinical sign could differentiate between radiological outcomes. Hypoxemia was less frequent in children with radiological normal findings (Supplemental Table 5).
Association of Clinical Characteristics With Radiological Endpoint Pneumonia in Children With WHO-Defined Clinical Pneumonia.

Variables presented as number (column percentage). N represents total number of children per category unless otherwise specified.
Abbreviations: CI, confidence interval; NA, not applicable.
Odds ratios for endpoint pneumonia versus non-endpoint pneumonia using univariable logistic regression.
Danger signs as per WHO definition: inability to breastfeed or drink, lethargy or reduced level of consciousness, convulsions.
Increased respiratory rate according to age is defined as >50 breaths per minute in children aged 2 to 12 months and >40 breaths per minute in children aged ≥12 months.
Peripheral capillary oxygen saturation was measured in room air using Mindray VS-800 Vital Sign Monitor or Biolight BLT M800 Handheld pulse oximeter, and hypoxemia was defined as oxygen saturation in room air under 90%. 30
Severe chest indrawing was defined as supraclavicular and/or suprasternal indrawing.
Association of Host-Response Biomarker Levels With Radiological Findings
Children with endpoint pneumonia presented higher ESR (P = .008), CRP-study (P = .007), and PCT (P = .003) (Table 4; Figure 2). After adjusting for demographic and clinical variables, ESR, CRP-study and PCT remained significantly higher among children with endpoint pneumonia (Table 5). IL-6 and sTNFR1 levels were higher in children with endpoint pneumonia but they did not reach statistical significance. When analyzing biomarkers as dichotomous variables (high versus normal) using thresholds widely used in clinical practice, we found that neutrophilia, ESR ≥ 50 mm, CRP-study > 4 mg/dL and PCT ≥ 250 pg/mL were more frequent among children with endpoint pneumonia (Table 4).
Association of Host Response Biomarkers With Radiological Endpoint Pneumonia in Children With WHO-Defined Clinical Pneumonia.
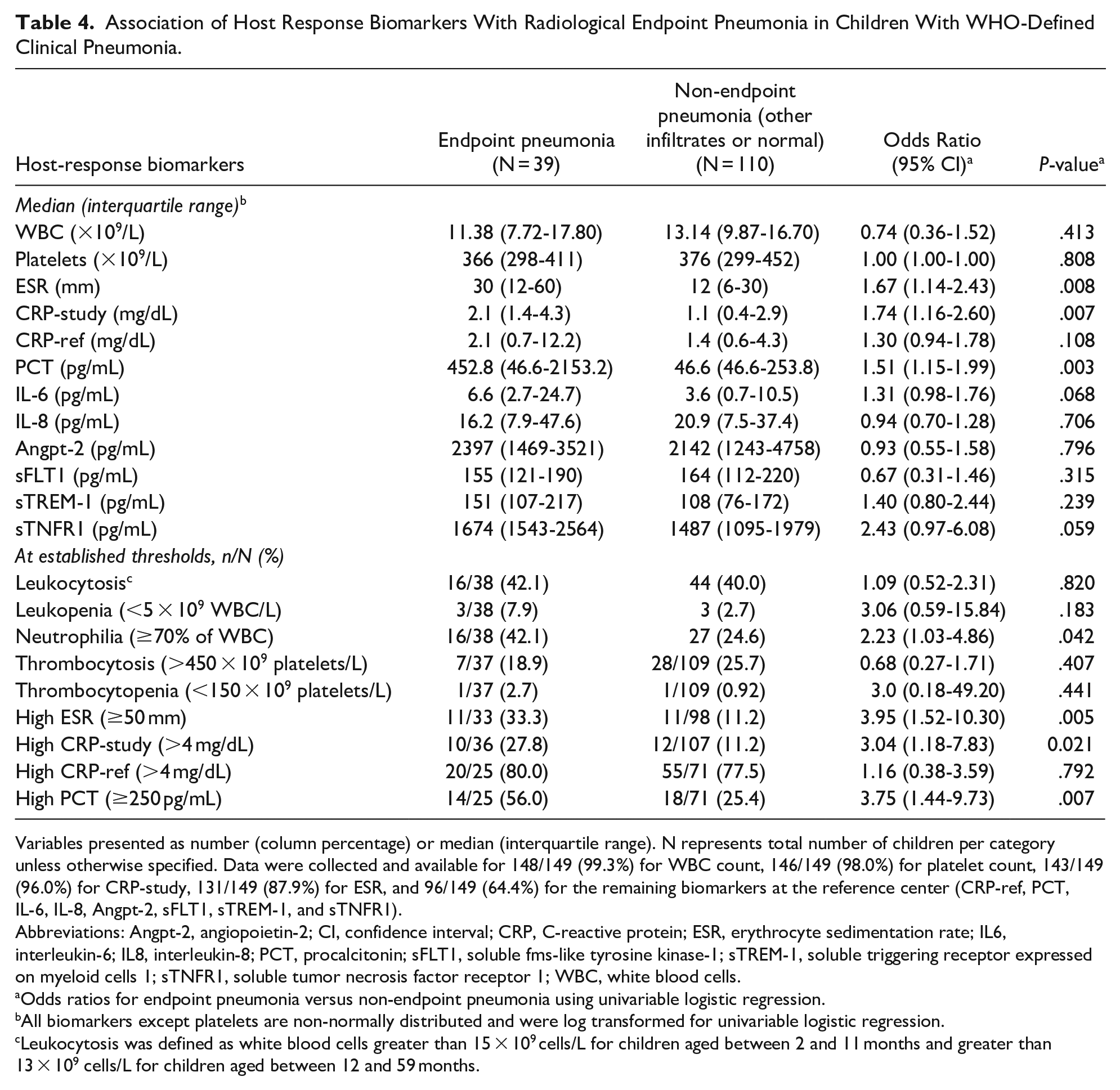
Variables presented as number (column percentage) or median (interquartile range). N represents total number of children per category unless otherwise specified. Data were collected and available for 148/149 (99.3%) for WBC count, 146/149 (98.0%) for platelet count, 143/149 (96.0%) for CRP-study, 131/149 (87.9%) for ESR, and 96/149 (64.4%) for the remaining biomarkers at the reference center (CRP-ref, PCT, IL-6, IL-8, Angpt-2, sFLT1, sTREM-1, and sTNFR1).
Abbreviations: Angpt-2, angiopoietin-2; CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IL6, interleukin-6; IL8, interleukin-8; PCT, procalcitonin; sFLT1, soluble fms-like tyrosine kinase-1; sTREM-1, soluble triggering receptor expressed on myeloid cells 1; sTNFR1, soluble tumor necrosis factor receptor 1; WBC, white blood cells.
Odds ratios for endpoint pneumonia versus non-endpoint pneumonia using univariable logistic regression.
All biomarkers except platelets are non-normally distributed and were log transformed for univariable logistic regression.
Leukocytosis was defined as white blood cells greater than 15 × 109 cells/L for children aged between 2 and 11 months and greater than 13 × 109 cells/L for children aged between 12 and 59 months.

Host biomarkers levels according to radiological findings (endpoint pneumonia vs non-endpoint pneumonia).
Adjusted Associations for Host-Response Biomarkers With Radiological Endpoint Pneumonia in Children With WHO-Defined Clinical Pneumonia.
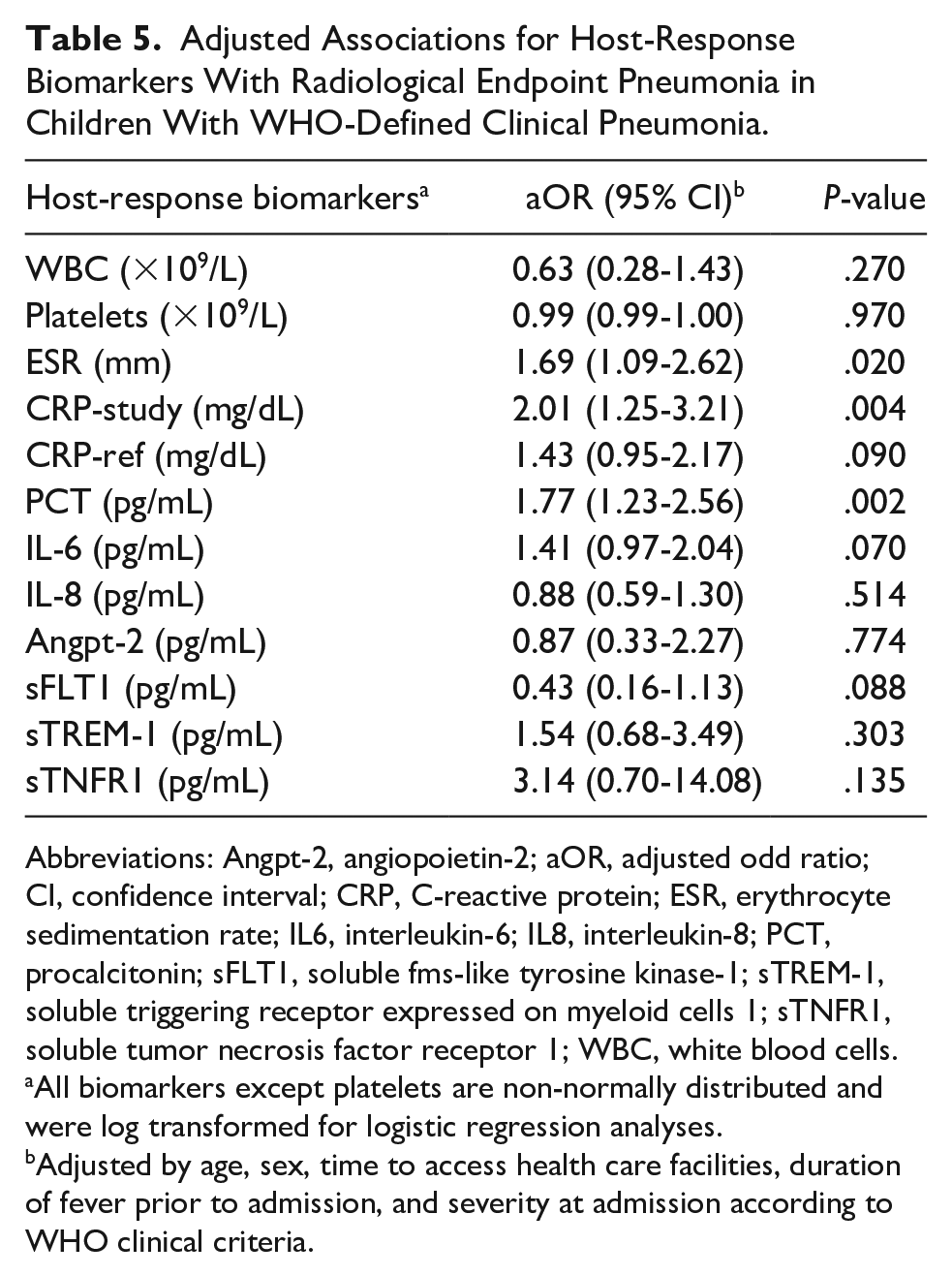
Abbreviations: Angpt-2, angiopoietin-2; aOR, adjusted odd ratio; CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IL6, interleukin-6; IL8, interleukin-8; PCT, procalcitonin; sFLT1, soluble fms-like tyrosine kinase-1; sTREM-1, soluble triggering receptor expressed on myeloid cells 1; sTNFR1, soluble tumor necrosis factor receptor 1; WBC, white blood cells.
All biomarkers except platelets are non-normally distributed and were log transformed for logistic regression analyses.
Adjusted by age, sex, time to access health care facilities, duration of fever prior to admission, and severity at admission according to WHO clinical criteria.
ESR, CRP-study and PCT were significantly higher in children with endpoint pneumonia compared to those with normal radiological findings, and PCT and sTNFR1 were also higher in children with endpoint pneumonia compared to those presenting other infiltrates. Children with other infiltrates presented higher levels of CRP-study and IL-8 compared to those with normal radiological findings (Supplemental Table 7; Supplemental Figure 1).
We further explored the performance of the biomarkers that showed significant association with radiological findings for identifying endpoint pneumonia, by analyzing the AUC (Figure 3). Although none of the biomarkers presented good discriminatory ability between endpoint and non-endpoint pneumonia, PCT presented the best overall discriminatory ability with 72% (95% CI 50.6-87.9) sensitivity and 66.2% (95% CI 54.0-77.0) specificity.

Performance of ESR, CRP and PCT for identifying radiological endpoint pneumonia among children with WHO-defined clinical pneumonia.
Discussion
The following study is the first published series of comprehensive radiological findings and its association with clinical signs, host-response biomarkers and etiology, among Bhutanese children admitted with pneumonia. Over half of the children presented a normal CXR and a quarter showed radiological endpoint pneumonia, which is comparable to the findings of the recently conducted multicenter study that used the same criteria for CXR classification. 18
Although CXR are still used as reference standard for the diagnosis of pneumonia in clinical practice and for investigation purposes, CXR remain an imperfect diagnosis tool to discriminate between bacterial and viral etiology. It is widely accepted that consolidation is the radiographic finding most frequently associated with bacterial etiology, and this is the basis of our analysis.13,31 However, 85.7% of children with radiological endpoint pneumonia (presumably of bacterial origin) presented with at least 1 respiratory virus, similar to children with other radiological outcomes. We found no association for any single virus with radiological findings, except parainfluenza virus with radiological endpoint pneumonia among a small number of children identified with such virus (n = 15). Furthermore, nasopharyngeal identification of respiratory virus requires careful interpretation. Distinction between nasopharyngeal carriage and causative agent is difficult, 4 and respiratory virus detection does not exclude a bacterial infection.4,32 There is a growing evidence showing an overlap of viral and bacterial etiology in respiratory infections, and the probable important interaction between them in the pathogenesis of pneumonia.32-34
The association between clinical signs and radiological findings has been assessed to identify children with pneumonia that need antibiotics. Increased respiratory rate, hypoxemia, crackles, fever on admission, and duration of illness were found to be associated with endpoint pneumonia, indicative of bacterial pneumonia. 13 Other studies found that no single clinical finding is sufficient to predict radiological pneumonia. 3 These contradictory findings might be in part due to differences in the definition of clinical pneumonia and the interpretation methods and classification of CXR. In our study, days of fever and severity of pneumonia were associated with endpoint pneumonia. However, increased respiratory rate and hypoxemia (the 2 backbone criteria of the WHO definition for clinical pneumonia) were present in similar proportions of children with and without endpoint pneumonia, despite hypoxemia occurring significantly more often in children with endpoint pneumonia or with other infiltrates than with normal CXR. Other single clinical characteristics such as crackles and fever on admission were not associated with endpoint pneumonia either. These findings suggest that a high proportion of children presenting with clinical signs usually considered more indicative of bacterial pneumonia, such as hypoxemia (73.1%) or crackles (58.3%), have radiological evidence of non-endpoint pneumonia. Therefore, a proportion of children with radiological non-endpoint pneumonia truly have pneumonia, supporting the notion that standardized definitions of radiological pneumonia have low predictive value for clinical management and decision on antibiotic needs. 18
Despite clinical similarities between radiological outcomes, CRP, PCT, and ESR, were significantly higher among children with endpoint pneumonia. The association between CRP and PCT and radiological endpoint pneumonia (as a proxy for bacterial pneumonia) or microbiologically confirmed bacterial pneumonia has already been reported,16,35-44 but results are not as clear for ESR.38,45,46 The other biomarkers investigated in this study were not associated with radiological outcomes.
A point-of-care biomarker to identify bacterial etiology, would help decision-making to start or discontinue antibiotics in children with clinical pneumonia.47,48 Measurement of biomarkers in patients with acute respiratory infections at the point-of-care has shown to reduce antibiotic use.49,50 This has also been evidenced for PCT-guided antibiotherapy in children with pneumonia in high-income countries.37,51-53 In our study, PCT was the biomarker with most promising results to identify radiological endpoint pneumonia as a proxy for bacterial etiology. PCT has shown to have a better diagnosis performance for bacterial pneumonia compared to CRP, WBC, and ESR, although there is no consensus on precise cut-off to be used.37,38,40,45 However, PCT is currently not available in Bhutan. Findings of this study could encourage policymakers in Bhutan to contemplate incorporating the measurement of PCT in clinical practice, with the potential to improve decisions about antibiotic needs, leading to better clinical outcomes and reducing antibiotic overuse. Rural and remote areas where laboratory facilities are of difficult access are likely to benefit of its readiness as a PCT point-of-care diagnostic tool. However, clinical efficacy and cost-effectiveness studies are required to estimate its potential impact in the Bhutanese setting.
In addition, and prior to implementation of any point-of-care diagnostic tool, an important question remains unanswered regarding care of childhood pneumonia. Which kind of marker would best assist clinicians in decision making: etiological markers or prognostic ones? It is possible that the lack of single clinical signs or biomarkers, or simple clinical algorithm that clearly discern bacterial from viral pneumonia is explained by the common mixed etiology. 16 The combination of several biomarkers—or biomarker signature—derived from different pathophysiological pathways, associated or not with clinical signs, seems to provide a better performance in the differentiation of bacterial from viral pneumonia.16,35,45,54,55 However, a biomarker able to identify children at risk of severe disease that would benefit from prioritization of care from those (the majority) with a self-limited disease without antibiotics, is likely to present major benefits.5,56,57 We report the performance of biomarkers to risk stratify children with pneumonia elsewhere (unpublished). We encourage further investigation to help identify a biomarker with such characteristics, guiding clinical care for children with pneumonia to improve clinical outcome and reduce the unacceptable high mortality associated to this disease.
Our study was not designed to assess the predictive diagnostic value of clinical characteristics or biomarkers. Therefore, due to the relatively small sample size, this study was underpowered to rule in or rule out biomarkers to detect children with antibiotics needs.
It remains very challenging to identify children with pneumonia that require antibiotics, by contemplating clinical, laboratory, and radiological characteristics. Conclusions regarding single clinical signs and biomarkers are conflicting, and further investigation is required to validate biomarker signatures capable of accurately identifying bacterial pneumonia and overall prognosis.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X221078698 – Supplemental material for Association of Clinical Signs, Host Biomarkers and Etiology With Radiological Pneumonia in Bhutanese Children
Supplemental material, sj-docx-1-gph-10.1177_2333794X221078698 for Association of Clinical Signs, Host Biomarkers and Etiology With Radiological Pneumonia in Bhutanese Children by Sophie Jullien, Melissa Richard-Greenblatt, Aina Casellas, Kinley Tshering, Jose Luis Ribó, Ragunath Sharma, Tashi Tshering, Dinesh Pradhan, Kumbu Dema, Michelle Ngai, Carmen Muñoz-Almagro, Kevin C. Kain and Quique Bassat in Global Pediatric Health
Footnotes
Acknowledgements
We are grateful to the children and families who participated in this study. We are thankful to the nurses who contributed in the collection of the samples, the pediatric department of JDWNRH who contributed to identifying eligible cases, and to the radiology and microbiology departments for their support. We also thank Kathleen Zhong for the measurement of host-response biomarkers, and Laia Blanco Lopez and Selene Garcia-Garcia for contributing to the microbiological analysis of viruses. We are grateful to the Spanish Society of Paediatric Infectology (Sociedad Española de Infectología Pediátrica, SEIP) for their financial support, which contributed to the shipment and testing of biological samples. ISGlobal receives support from the Spanish Ministry of Science and Innovation through the “Centro de Excelencia Severo Ochoa 2019-2023” Program (CEX2018-000806-S), and support from the Generalitat de Catalunya through the CERCA Program. CISM is supported by the Government of Mozambique and the Spanish Agency for International Development (AECID). This study was supported in part by the Canadian Institutes of Health Research (CIHR) Foundation grant FDN-148439 [KCK] and the Canada Research Chairs program [KCK].
Author Contributions
Conceptualization: SJ, MRG, KCK, QB. Data curation and analysis: SJ, AC. Investigation: SJ, KT, JLR, RS, TT, DP, KD, MN, CMA. Methodology: SJ, MRG, KCK, QB. Project administration: SJ, QB. Writing original draft: SJ. Writing, review and editing: SJ, MRG, AC, CMA, KCK, QB.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SJ reecived a pre-doctoral fellowhip from the Secretariat of Universities and Research, Ministry of Enterprise and Knowledge of the Government of Catalonia and co-funded by European Social Fund. This study received financial support from the Spanish Society of Paediatric Infectology (Sociedad Española de Infectología Pediátrica, SEIP), which contributed to the shipment and testing of biological samples [SJ]. ISGlobal receives support from the Spanish Ministry of Science and Innovation through the “Centro de Excelencia Severo Ochoa 2019-2023” Program (CEX2018-000806-S), and support from the Generalitat de Catalunya through the CERCA Program [SJ, AC, QB]. CISM is supported by the Government of Mozambique and the Spanish Agency for International Development (AECID) [QB]. This study was supported in part by the Canadian Institutes of Health Research (CIHR) Foundation grant FDN-148439 [KCK] and the Canada Research Chairs program [KCK]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.