
Abstract
In the Republic of Congo, a country where tuberculosis is endemic, there have not been many reports about tuberculosis pneumonia. This study aimed to describe the epidemiology, clinical features, and outcome of tuberculosis pneumonia in children. This was a retrospective study of 9 cases of children admitted from 2002 to 2015, that is, 0.7 cases per year. The average age was 37 months. The mean delay from the beginning of symptoms to the visit to a medical center was 36 days (range = 4-93 days). Physical examination indicated a pulmonary consolidation in 6 cases. Chest X-ray revealed a unilateral opacity in all cases. Sputum and gastric washing bacilloscopies were positive in all cases, and HIV serology was positive in 2 cases. Therapeutic observance was perfect and the evolution favorable. Tuberculosis pneumonia must be systematically proposed for children under 5 years of age, who present symptoms that are in contrast with the seriousness of chest X-ray injuries.
Introduction
Tuberculosis pneumonia (TP) is an acute form of pulmonary tuberculosis. Despite the fact that the advent of HIV/AIDS has changed the epidemiological, clinical, and prognostic face of tuberculosis, TP remains a rare disease entity, not much described even in countries where tuberculosis is endemic.1-3 The semiologic difference with community-acquired pneumonia is not always easy and causes delays in the diagnosis and initiation of treatment. In Congo, preliminary study on TP was done in a study of radiographic aspects of tuberculosis in children. 4 Using this broader series, epidemiological aspects, clinical aspects, and evolution are described in this study.
Patients, Methods, and Results
This is a retrospective study of the records of 9 children admitted between 2002 and 2015 for TP in the Pediatrics Department at the University Hospital Center of Brazzaville, with an incidence of 0.7 cases per year. Table 1 summarizes the epidemiological, clinical, and laboratory features of the children. The sex ratio was 2 boys for 7 girls. The median age was 37 months (range = 2 months to 6½ years).
Epidemiological, Clinical, and Laboratory Features of Children.

Abbreviations: TB, tuberculosis; ESR, erythrocyte sedimentation rate.
The mean delay in admission to hospital was 36 days (range = 4-93 days). Fever and cough were the main reasons for consultation. No child had hemoptysis. On the contrary, 4 children (Nos. 1, 4, 5, and 8) had pleuritic chest pain. Before admission, 7 children (Nos. 1, 2, 4, 6, 7, 8, and 9) received antimalarial and oral antibiotics. Amoxicillin was the antibiotic that was used most (all cases) followed by cotrimoxazole (2 cases), cefuroxime (1 case), and cefixime (1 case). On admission, physical examination revealed a frank pulmonary condensation syndrome (Nos. 1, 2, 3, 4, 5, and 7) or isolated crackles (Nos. 6 and 9). However, one child had a normal auscultation (No. 8). Chest X-ray revealed unilateral opacity in all cases, sitting right in 7 cases; it concerned 1 lobe in 7 cases (Figure 1) and 2 lobes in 2 cases (Figure 2). When the opacity was localized to one lobe, it was the lower lobe in 5 cases (Nos. 1, 2, 5, 6, and 8) and the upper lobe in 2 cases (Nos. 4 and 9). The middle lobe was concerned in 2 cases but associated with upper lobe damage (Nos. 3 and 7). Aeric bronchogram was found in the opacity in 3 cases (Figures 1 and 2). The affection of the lung parenchyma was associated with the pericardial one (No. 4), confirmed by echocardiography. Complete blood count highlighted the following: a median number of white blood cells at 12 671 GB/mm3 (range = 4000 to 18 600 GB/mm3) with a median number of polynuclear at 13 040/mm3 (range = 3700 to 17 000/mm3) and lymphocytes at 10 800/mm3 (range = 2500 to 13 000/mm3). The median rate of hemoglobin was 8.45 g/dL (range = 6.7 to 14), and the median platelet count was 310 × 103 (range = 78 103 to 599 × 103/mm3). Smear, performed by direct examination of gastric lavage fluid (Nos. 3, 6, 7, and 9), or sputum (Nos. 1, 4, 5, and 8) were all positive. All children in this series received antituberculosis treatment according to the short protocol, except for child No. 4, who was treated for 8 months because of associated tuberculous pericarditis. Therapeutic compliance was perfect. Corticosteroids were used in addition to tuberculosis treatment (prednisone 1 mg/kg/24 h) in 2 cases. One case of TP was associated with pericarditis (No. 4), and another case of TP was associated with respiratory distress (No. 7). Tuberculosis treatment started within 7 to 10 days after admission. In the service, except for child No. 9, patients received first usual antibiotics (amoxicillin, amoxicillin-clavulanic acid, ceftriaxone) without success. No child benefited from a follow-up smear microscopy. However, the outcome was favorable in all cases, apart from the child No. 7, who presented, during treatment, excavations in the opacity (Figure 3).

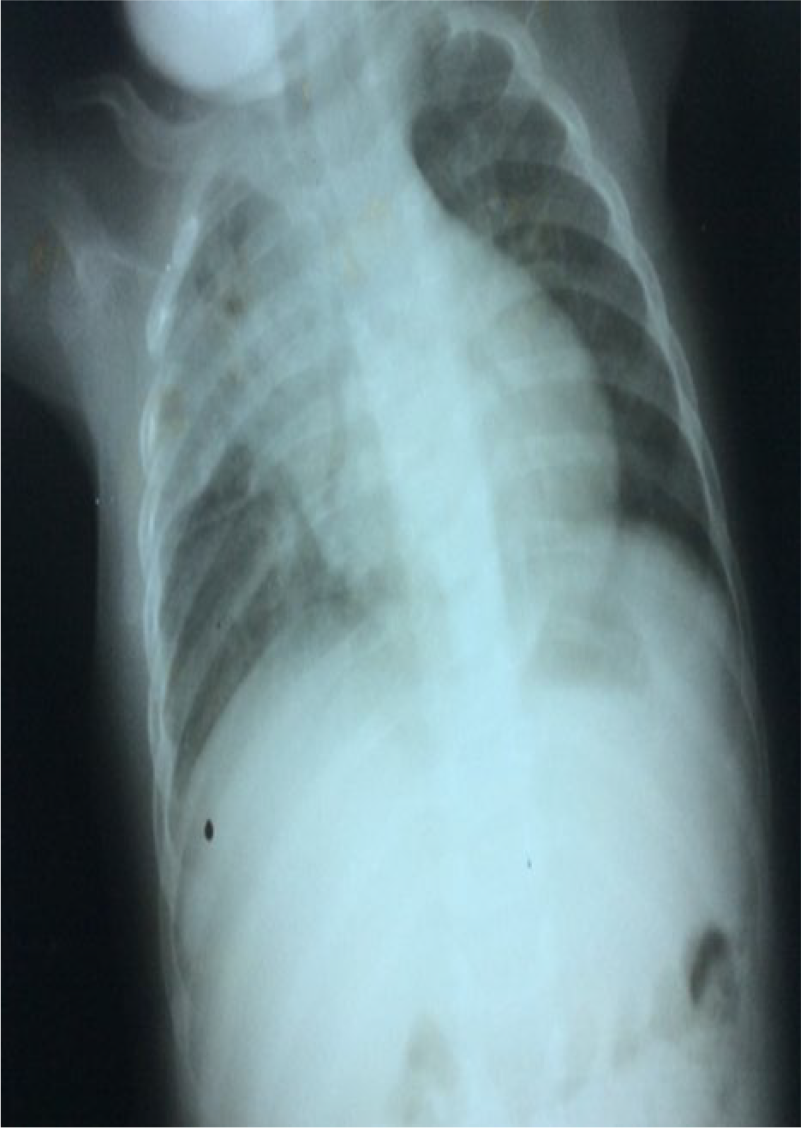
Opacity of apical-posterior segment of the left upper lobe with discreet air bronchogram in a 10-year-old girl.

Alveolar opacity of right upper and middle lobe with air bronchogram in a 13-month-old girl.
Tuberculosis-excavated pneumonia of the right upper and middle lobes on the 20th day of tuberculosis treatment (Case No. 7).
Discussion
TP is a rare clinical form of pulmonary tuberculosis. Its incidence varies from one series to another. Steponaviciene and Kudzyte, 5 in Lithuania, reported a series of 69 cases in 10 years, and Goussard et al, 2 in a South African cohort, reported 24 cases. Other authors have rather described TP within a cohort with pneumonia from all causes, for example, Oliwa et al, 6 in a series of 3644 children admitted with acute pneumonia and smear, reported a TP prevalence of 7.5%. In contrast, in countries where the incidence of HIV infection is very high, the prevalence was higher, in the range of 12% to 18.9%.7,8 TP occurs at any age but with a predominance in children under 5 years or under 2 years. Thus, in our series, 6 children were under 5 years of age, including 4 under 2 years of age. These results are similar to those of Goussard et al 2 and Steponaviciene and Kudzyte, 5 who reported, respectively, 75% and 79% of children under 5 years of age. Close-contact tuberculosis was found only in 3 children, that is, 33.3% of cases. These are common findings, since in infants who are dependent on relatives, tuberculosis contact is never found in all cases. 9 Similarly, BCG vaccination, found in 7 children in this series, did not prevent the occurrence of the disease, the same as in 75.2% of infants in a series reported by Mabiala-Babela et al. 9 The state of malnutrition reported in 5 children is one of the signs guiding to TP, 7 although for other authors, the value of the body mass index is not statistically different between children with TP and those with nontuberculous pneumonia. 10 Concerning the Mantoux tuberculin skin test, skin anergy was found in 6 cases. The TP is a severe form of tuberculosis, and high incidence of anergy is only logical as it is seen in other serious forms of tuberculosis such as miliary tuberculosis. In this series, the mean delay in admission to hospital was 36 days. The delayed diagnosis in developing countries is constant. The regular use of alternative medicine in our country 11 is one of the reasons. In addition to these diagnostic difficulties of this entity, clinically it can be taken for a community-acquired pneumonia. Besides, 7 children in this series received antibiotics before admission and even as initial therapy during hospitalization. Now, some authors believe that prolonged duration of symptoms is an element in favor of TP. 10 In most cases, the most striking clinical feature lies in the contrast between the importance of radiological damage and the absence or at least the discretion of symptoms during the greater period of the evolution. The location of parenchymal opacity is variable. In our study, the right unilateral impairment was predominant, and mostly the lower lobe. The predominance of right lung injury during pulmonary tuberculosis has been reported by several authors.4,9,12 The rarity of air bronchogram (3 of 9 cases in this series), and the involvement of the lower lobe (7 children, among them 2 children had an associated impairment of the middle lobe), is a constancy in TP. 10 As for biological abnormalities during TP, abnormal platelet and red blood cell have no contribution for diagnosis. On the contrary, speaking of white blood cells, leukocytosis described at the expense of lymphocytes is not always found; however, a normal leukocytosis is a discriminating element between TP and community-acquired pneumonia 10 as observed in 5 cases (cases 1, 2, 3, 6, and 9). Besides this normal leukocytosis often contrasts with an elevated erythrocyte sedimentation rate as reported in Cases 1, 2, 3, 4, and 5 of this series. Two children had a positive HIV serology. Given our results and those reported in the literature,2,13 TP is not boosted by HIV infection, although other authors have reported a high incidence of tuberculosis in severely malnourished children and those HIV-positive admitted for pneumonia.7,8 Therapeutic compliance was considered good in all cases and no deaths have been recorded. Overall, mortality from this form is higher compared to that reported in the series including all forms of pulmonary tuberculosis, 14 with an active role in HIV infection.
Conclusion
Ultimately, TP is a rare entity in comparison to other clinical forms of pulmonary tuberculosis. However, in our countries where the prevalence of HIV infection is high, TP should systematically be raised for discussion in a child under 5 years of age, with a tubercolosis contact history, a little noisiness of the clinical picture contrasting with the severity of the radiographic damages, and the accelerated erythrocyte sedimentation rate.
Author Contributions
ERN: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JRMB: Contributed to analysis and interpretation; critically revised manuscript; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SVMM: Contributed to analysis; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
GM: Critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.