
Abstract
Objective
To measure the rate of the A2063G mutation in the Mycoplasma pneumoniae (M. pneumoniae) 23S rRNA domain V in children with pneumonia and to determine the correlation between radiographic findings and the presence of the A2063G mutation.
Methods
Patients who were hospitalized with a confirmed diagnosis of M. pneumoniae pneumonia were enrolled in this study. M. pneumoniae strains were collected for genotype analysis. Chest radiography was performed on all children prior to and following macrolide treatment. Clinical and imaging data were obtained.
Results
Of 211 patients, 195 (92.42%) harboured M. pneumoniae with the A2063G mutation. No significant differences were identified in inflammation score, chest radiography inflammation absorption grade before and after macrolide treatment, or pulmonary complications (atelectasis, hydrothorax, or pleuritis) prior to macrolide treatment when children were stratified based on the presence or absence of the A2063G mutation.
Conclusions
A high proportion of children with pneumonia harboured strains of M. pneumoniae with the A2063G mutation in the 23S rRNA domain V. However, no obvious chest radiographic features of M. pneumoniae pneumonia were associated with the A2063G variant.
Introduction
Mycoplasma pneumoniae (M. pneumoniae) is a common agent of community-acquired pneumonia in children and young adults. 1 As M. pneumoniae has no cell wall, it is intrinsically resistant to β-lactams and other antibiotics that target the cell wall. Therefore, macrolides, especially 14- and 15-membered ring macrolides, are used as first-line agents in children to avoid the potential age-related side-effects of other therapies; tetracyclines have possible adverse effects on enamel hypoplasia and bone, and quinolones may influence the growth of bone and articular cartilage. 2 However, recently increasing numbers of infections are leading to refractory or life-threatening pneumonia with pulmonary and/or extrapulmonary complications.3–5 Multiple factors including M. pneumoniae load, 6 macrolide-resistance, 7 systemic inflammatory response2,8 and mixed infection may underlie the development of severe M. pneumoniae pneumonia in patients.
Macrolide antibiotics are known to inhibit protein synthesis by binding to domain II and/or domain V of the M. pneumoniae 23S rRNA.9,10 In turn, the primary mechanism of macrolide-resistance comprises mutations in target genes.9–11 In particular, point mutations at nucleotide positions A2063, A2064, A2067 and C2617 in domain V have been identified as common mutations.10,12 M. pneumoniae, with an A-to-G or A-to-C transition at position 2063 of the 23S rRNA gene results in high resistance to 14- and 15-membered ring macrolides, whereas mutations at positions A2067 and C2617 confer lower levels of resistance.2,12 The presence of M. pneumoniae mutants has been reported to be mainly associated with persistent clinical symptoms such as fever, resulting in prolonged hospital stay.3,13 To the best of our knowledge, few studies have investigated the correlation between radiographic findings and gene mutations in M. pneumoniae pneumonia in children.
The most common radiographic findings in M. pneumoniae pneumonia consist of unilateral or bilateral areas of air-space consolidation and ground-glass opacities. However, these findings are variable and can include reticular or nodular opacities. 14 The current study examined the prevalence of the A2063G mutation in the M. pneumoniae 23S rRNA domain V in children with pneumonia and the correlation between radiographic findings and the presence of this mutation.
Patients and methods
Study population
Patients were enrolled from the Department of Respiratory Medicine, Children’s Hospital of Nanjing Medical University Nanjing, Jiangsu Province, China between 1 March 2014 and 31 May 2015. Patients were included in the study if they fulfilled the following three criteria: 14 (i) diagnosis of pneumonia based on symptoms at admission, including fever, cough, productive sputum, chest pain, dyspnoea, abnormal breathing sounds, and a new infiltrate on chest radiography that was at least segmental; (ii) acute M. pneumoniae infection was confirmed by polymerase chain reaction (PCR) and/or serology (detecting M. pneumoniae immunoglobulin M by enzyme-linked immunosorbent assay in the acute phase or M. pneumoniae antibody titres increased ≥4 times in the recovery phase); (iii) the absence of other pathogens (bacteria, respiratory syncytial virus, influenza virus, adenovirus, parainfluenza virus, Chlamydia pneumoniae, Coxiella bumetii, tuberculosis and Legionella pneumophila) and the ineffectiveness of penicillin, cephalosporin, and sulfonamide. The following patients were excluded: convalescent patients, patients with immunosuppressive illness, asthma, chronic lung disease, or other systematic disease. Chest radiography was undertaken both before and after macrolide treatment. Demographic data and chest radiography findings were noted.
The study protocol was approved by the Ethics Committee of the Children’s Hospital of Nanjing Medical University and written informed consent was obtained from at least one parent/guardian of each patient included.
Study methods
Nasopharyngeal aspirates were collected at admission and assayed for M. pneumoniae DNA copy number using the M. pneumoniae DNA PCR kit (ACON Biotech Co., Ltd, Hangzhou, China). The 23S rRNA domain V was amplified by nested PCR as described previously. 15 Amplification products were then shipped at 4℃ within 2 days for sequencing at Yingweijie, Shanghai, China. Finally, DNA sequences were compared using BLAST® to the M. pneumoniae strain M129 (ATCC 29342). 16 Patients were treated with 10 mg/kg per day azithromycin by oral administration or intravenous infusion for the first 3 days, after which patients did not receive treatment for the next 4 days. Finally, patients received a second 3-day treatment with 10 mg/kg per day azithromycin or with 30 mg/kg per day erythromycin by intravenous infusion. The course of macrolide treatment was approximately 1–3 weeks before the clinical symptoms improved and radiographic inflammation was absorbed. Tetracyclines and quinolones were not permitted to avoid possible adverse reactions. According to clinical manifestations, some drugs were selectively used, such as expectorants, cough medicine, inhaled corticosteroid, bronchodilators and immune modulators (corticosteroid and/or intravenous immunoglobulin). Clinical data were collected from medical records including sex, age, febrile days prior to macrolide treatment, immune modulator use, and chest radiography results prior to and after macrolide treatment.
Chest radiography scoring
Pneumonia radiographic inflammation evaluation questionnaire. 17

Pneumonia radiological inflammatory absorption questionnaire. 18

Grade evaluation was taken as the highest grade in the six lung fields. Total score evaluation was calculated as the difference between radiographic inflammation scores prior to and following treatment/radiographic inflammation scores prior to treatment × 100%.
Statistical analyses
All statistical analyses were performed using the IBM SPSS® statistical package, version 20.0 (IBM, Armonk, NY, USA) for Windows®. Data are presented as mean ± SD. For data with a skewed distribution, median values and range are reported. Student’s t-test was used to compare continuous variables, whereas χ2-test and Fisher’s exact test were used for categorical variables. The linear correlation was determined between two variables. A P-value < 0.01 was considered statistically significant.
Results
A total of 211 children were enrolled in the current study, of whom 108 (51.18%) were male and 103 (48.82%) were female. The median age was 4.8 years. Chest radiography was performed on all children prior to and after macrolide treatment.
Regarding the M. pneumoniae 23S rRNA genotypes, of the 211 study patients, 195 (92.42%) harboured the A2063G mutation in the M. pneumoniae 23S rRNA domain V, whereas the remaining 16 (7.58%) patients had no mutation. The children were stratified into two groups based on the presence or absence of the A2063G mutation. The mean age among the children infected with mutated M. pneumoniae was 4.789 years (98 males, 97 females) and was 4.974 years in the remaining patients (10 males, six females) infected with non-mutated strains. No significant differences were identified in age or sex distribution between the two groups.
Clinical characteristics of children infected with mutated and non-mutated Mycoplasma pneumoniae strains.

Data presented as mean ± SD or n of patients.
No significant between-group differences (P-value ≥ 0.01); Student’s t-test was used to compare continuous variables, χ2-test and Fisher’s exact test were used for categorical variables.
Radiographic inflammatory absorption grade prior to and after treatment in children infected with mutated and non-mutated Mycoplasma pneumoniae strains.
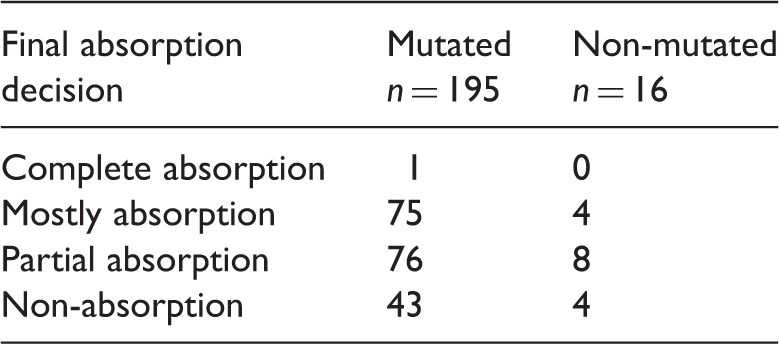
Data presented as n of patients.
No significant between-group differences (P-value ≥ 0.01); χ2-test.
Radiographic pulmonary complications in children infected with mutated and non-mutated Mycoplasma pneumoniae strains.

Data presented as n of patients.
No significant between-group differences (P-value ≥ 0.01); χ2-test.
Score of radiographic inflammation in children infected with mutated and non-mutated Mycoplasma pneumoniae strains stratified according to the use of immune modulators.
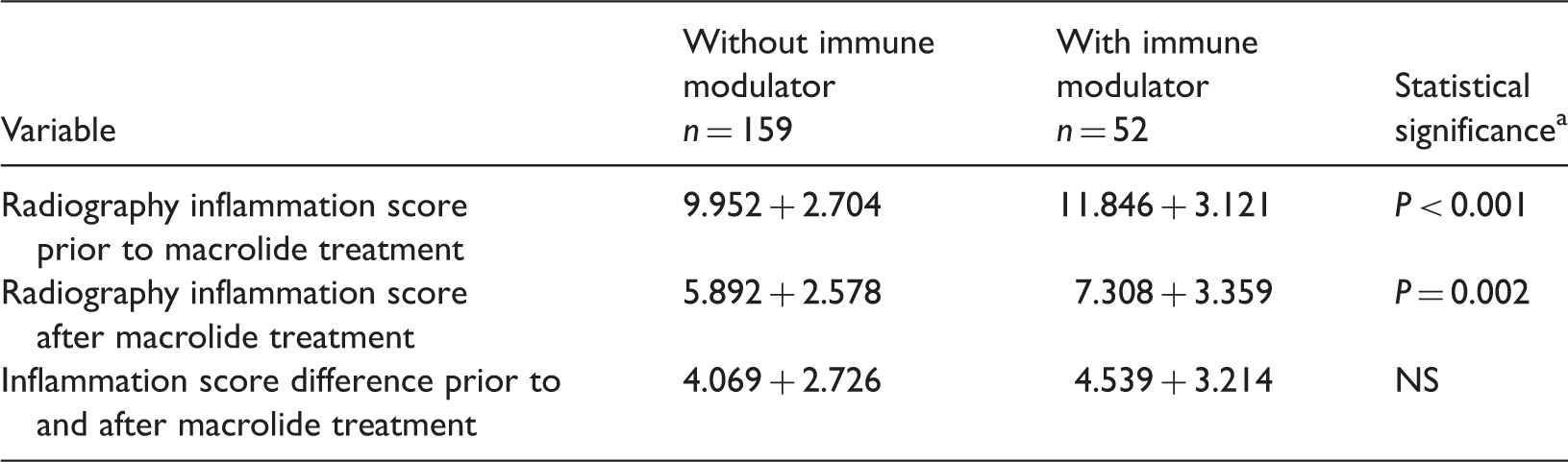
Data presented as mean ± SD.
Student’s t-test.
NS, no significant between-group difference (P-value ≥ 0.01).
Discussion
Mycoplasma pneumoniae represents a common agent of acute respiratory infections, exhibiting various clinical manifestations and involving multiple systems. Although M. pneumoniae infection is considered self-limiting, an increasing number of recent cases have progressed to severe, life-threatening pneumonia.1,3 In addition, the extensive use of macrolides as first-line therapeutics for children has fuelled worldwide macrolide resistance, especially in East Asia. 6 It is currently believed that genetic mutations in the domains targeted by macrolides result in the resistance and numerous studies have focused on the associations between clinical characteristics and the genetic mutations.3,10,14 However, to the best of our knowledge, few reports have explored the chest radiographic findings of M. pneumoniae pneumonia upon infection by the A2063G mutated strain.
Mycoplasma pneumoniae pneumonia exhibits diverse chest radiographic manifestations that have been classified into four types: (a) sheet or patchy infiltration similar to that of lobular pneumonia; (b) interstitial changes similar to viral pneumonia; (c) segmental or lobar infiltration similar to bacterial pneumonia; and (d) hilar node enlargement.13,18 Therefore, it is difficult to distinguish the pneumonia resulting from infection by M. pneumoniae from that arising from other pathogens. In the present study, there were no statistical differences between the two groups stratified by the presence or absence of the A2063G mutation in the chest radiological inflammation scores prior to and after macrolide treatment, the difference in these scores, the inflammatory absorption grade prior to and following treatment, or in chest radiological pulmonary complications prior to treatment. As a consequence, it was difficult to determine from the chest radiographs alone whether the infecting M. pneumoniae strain carried the A2063G mutation or to judge whether the pathogen was resistant to macrolide. The rate of immune modulator use was similar between the mutated (49/195 [25.13%]) and non-mutated groups (3/16 [18.75%]). The children treated with immune modulators had significantly higher chest radiography inflammation scores prior to macrolide treatment than those not treated with immune modulators. It might be that immune modulators reduce effusion and promote the absorption of pulmonary inflammation.
The pathogenic mechanism of M. pneumoniae is considered to include adhesion to respiratory epithelial cells, resistance to clearing and phagocytosis, cytotoxic effects caused by oxidative stress, community-acquired respiratory distress syndrome toxin, and M. pneumoniae-derived lipopeptides.19–22 Although increasing evidence suggests that the host immune response represents an important cause of inflammatory injury to the lung and other systems, 8 these pathogenic mechanisms are clearly irrelevant as macrolide targets, which might explain the lack of an observed relationship between chest radiography inflammation scores prior to treatment and A2063G mutation. However, no significant differences were observed in the chest radiographic inflammatory absorption grade prior to and after macrolide treatment between patients carrying mutated or non-mutated strains, or in the difference of inflammation scores after treatment. A possible explanation might be due to the host immune response after M. pneumoniae infection whereby the macrolide might have exerted an immunomodulatory function that provided additional benefits of the treatment.
In conclusion, the infecting M. pneumoniae strain in 195 of 211 (92.42%) patients in the current study was found to harbour the A2063G mutation in the 23S rRNA domain V. The A2063G mutation was determined to have no effect on the chest radiographic inflammation scores prior to and after macrolide treatment, their difference, the inflammatory absorption grade before and after macrolide treatment, or in the chest radiographic pulmonary complications occurring prior to treatment. This present study confirms that in the clinic, early chest radiographs will likely contribute to the diagnosis of M. pneumoniae pneumonia, but will not help to determine if the infected M. pneumoniae strain has the A2063G mutation. Immune modulators should be used early in severe pulmonary inflammation because they effectively alleviate the inflammatory reaction. In addition, these current findings support the continued use of macrolides as the first-line treatment of choice for paediatric patients with M. pneumoniae pneumonia owing to their potential immunomodulatory function and the age-related side-effects of other therapies.
Footnotes
Author contributions
Huan Deng and Jun Rui contributed equally to the work as the first authors. Huan Deng and Jun Rui participated in the design of the study, sample preparation, gene amplification and sequence alignment. Huan Deng wrote and submitted the manuscript. Feng Liu conceived of the study, participated in its design and helped to draft the manuscript. Deyu Zhao participated in the design of the study. All authors read and approved the final manuscript.
Acknowledgements
The authors wish to thank everyone who helped with this study.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This study was supported by grants from the National Natural Science Foundation of China (no. 81370132; Deyu Zhao) and the Nanjing Medical Science and Technique Development Foundation, Nanjing, China (Feng Liu).