
Abstract
Pleurisy and pleural effusion caused by Brucella infection are rare. However, clinicians lack an understanding of these possibilities, and the underlying disorder is easy to misdiagnose. We report a 52-year-old male farmer who was admitted to hospital with a fever, chest pain, and shortness of breath. Closed chest drainage was performed by thoracocentesis, and the concentration of adenosine deaminase (ADA) in the pleural fluid was >45 U/L. Mononuclear cells in the pleural fluid accounted for 90% of the cells, and pathology indicated a large number of lymphocytes. The clinical diagnosis was tuberculosis with tuberculous pleurisy. However, subsequent pleural fluid culture results did not support tuberculous pleurisy. The results of pleural fluid culture indicated Brucella, and the results of Brucella tiger red plate agglutination indicated a titer of 1:400 (+++). The final diagnosis was brucellosis with pneumonia and pleurisy. After 12 weeks of oral treatment, the patient underwent follow-up chest radiographs. Radiography indicated complete resolution of the hydrothorax and pneumonia, and the patient reported no discomfort. The short-term curative effect was excellent. Pleurisy associated with brucellosis should be considered a differential for pleurisy in regions where brucellosis is endemic, to minimize the risk of misdiagnosis.
Keywords
Introduction
Brucellosis is a common zoonotic disease in northern pastoral areas, such as Inner Mongolia, Qinghai, and Xinjiang, China,1,2 and one of the most common zoonotic diseases worldwide. 3 Brucella transmission routes are diverse, including the respiratory and digestive tracts, skin, and mucous membranes. 4 The clinical manifestations are nonspecific and involve multiple systems, such as bone, skeletal muscle, gastrointestinal tract, lymph nodes, and gonads. 3 The first symptoms are mainly fever and fatigue, and cases of pleural involvement are rare.1–4 Pleurisy and pleural effusion caused by Brucella infection have been reported only as individual cases globally, and to our knowledge, no large-sample-size studies have been published. The diagnosis and treatment of a case of Brucella pleurisy misdiagnosed as tuberculous pleurisy are summarized in this case report.
Case presentation
Basic information
A 52-year-old male farmer was admitted on 20 May 2022 for “fever with right chest pain for half a month, cough for 1 week”. On 5 May 2022, he developed chills and fever with no identifiable cause. His fever reached 39.0°C and responded to oral antipyretics. However, he gradually developed right-sided chest pain, and the cough and deep inspiratory chest pain worsened over time. Oral treatment at a local clinic with amoxicillin 0.5 g, three times per day for 4 days was ineffective. On 13 May 2022, cough and a small amount of white sputum appeared and was treated with traditional Chinese medicine for 7 days. The chest pain subsequently improved but persisted, with fever and cough, and he gradually developed shortness of breath. He came to our outpatient department for treatment on 20 May 2022, and chest X-ray revealed right lower lung exudative lesions and right pleural effusion. He was admitted for further diagnosis and treatment. His demeanor, appetite, and sleep were good and unaffected by his symptoms. He was in good health prior to the development of the current symptoms. He denied a history of raising and contact with livestock, there was no history of drinking raw milk, and he had eaten cooked haggis in a restaurant more than 20 days previously.
Physical examination
Physical examination revealed the following: body temperature: 36.0°C, pulse: 99 beats/minute, respiratory rate: 24 breaths/minute, and blood pressure: 106/68 mmHg. The superficial lymph nodes were not palpably swollen; however, the patient’s lips were slightly cyanotic, and his jugular veins were distended. The trachea was located centrally, right lung percussion revealed dullness, and neither dry nor wet rales were auscultated in either lung.
Diagnosis and treatment
Chest computed tomography (CT) was performed after admission (Figure 1) and revealed the following: emphysema and bullae, exudative lesions in the middle and lower lobes of the right lung, multiple fibrous septae in both lungs, and right pleural effusion. Pleural cavity ultrasonography on 20 May 2022 revealed multiple compartments within the areas of right pleural effusion.
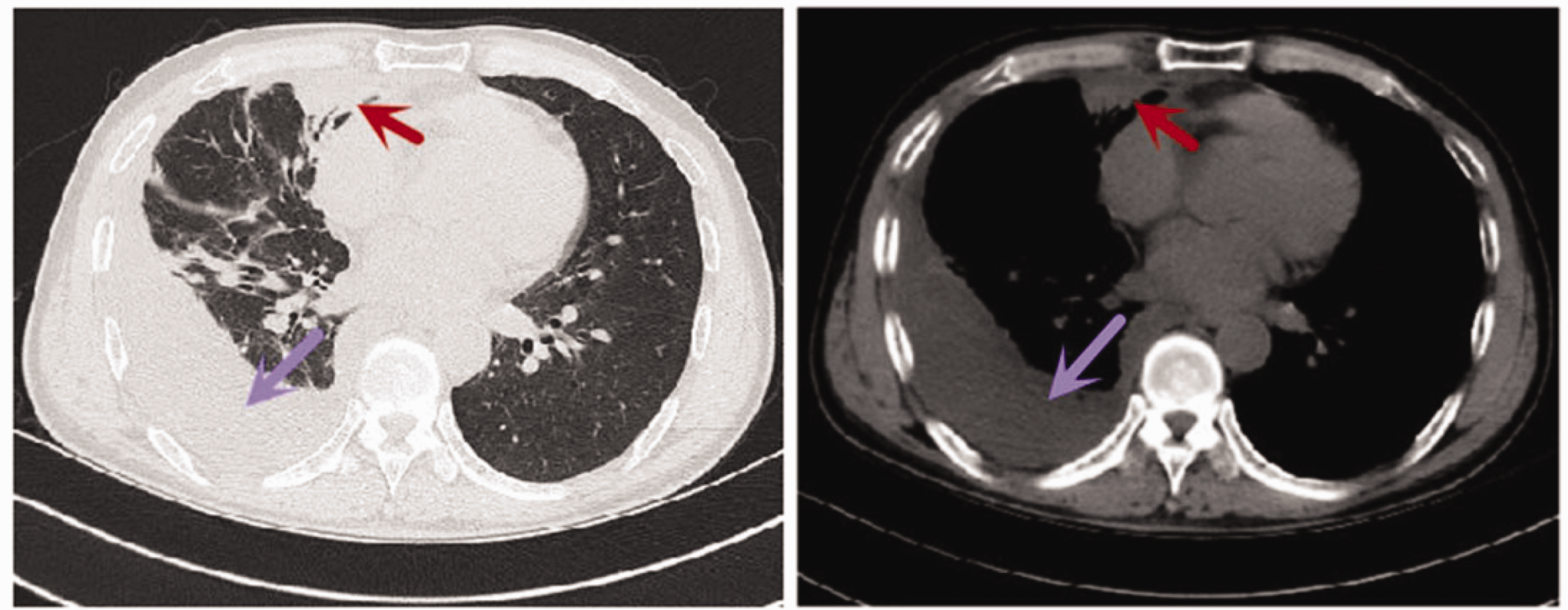
Chest computed tomography (CT) showing right pleural effusion (purple arrow), with middle lobe consolidation of the right lung (red arrow); left panel: lung; right panel: mediastinum.
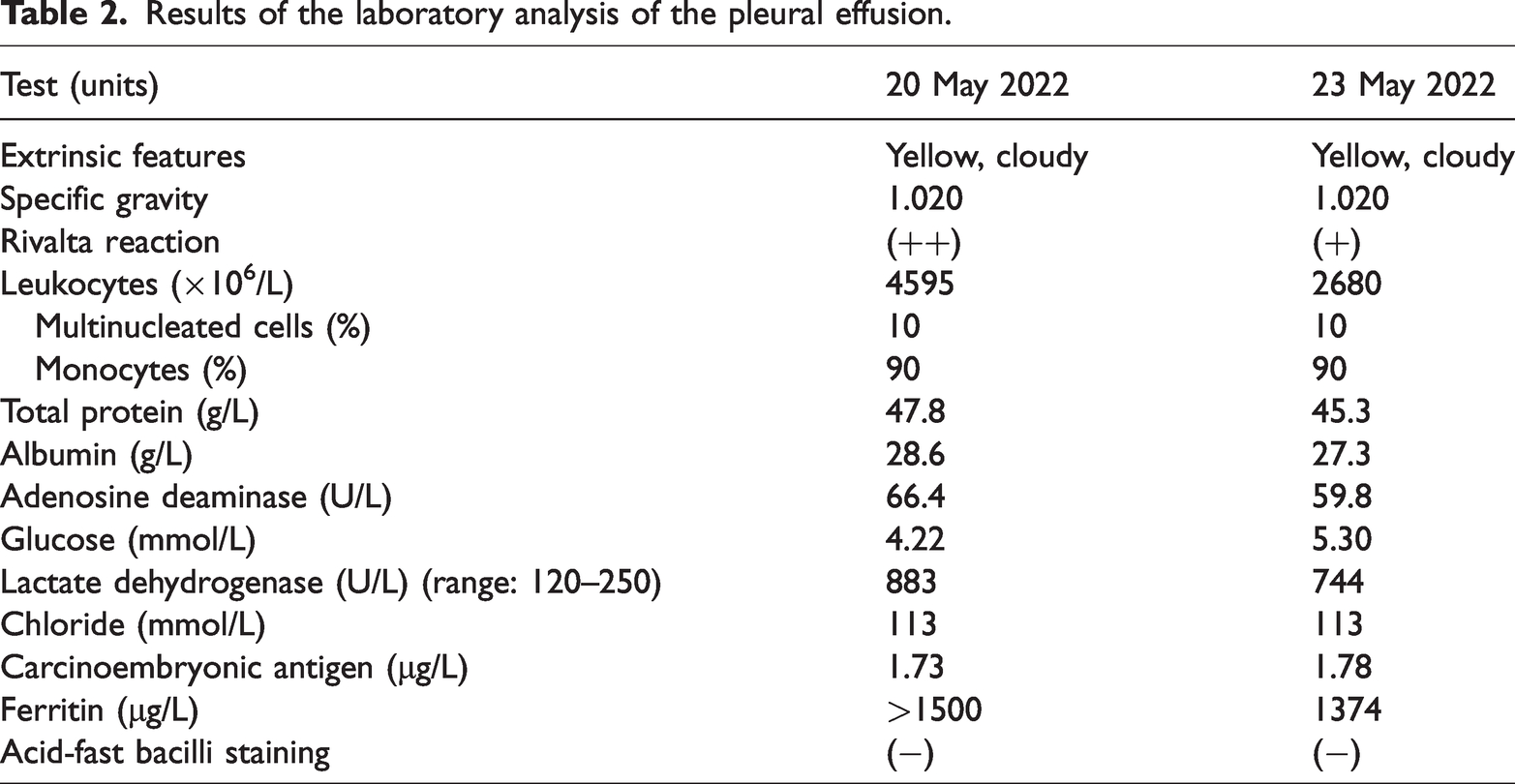
The acute onset, and the presence of chest pain and fever combined with the imaging findings and blood laboratory examination results on admission (Table 1) indicated a diagnosis of bacterial pleurisy complicated with pleural effusion and pneumonia. Ceftriaxone (3.0 g, via intravenous drip (ivgtt), once per day (qd)) and metronidazole (0.5 g, IV, every 8 hours (q8h)) were given for anti-infection, and closed drainage via thoracocentesis was performed under ultrasound guidance. A sample of the pleural effusion was submitted for cytology, bacterial culture, acid-fast bacilli staining, biochemical analysis, and routine laboratory analysis (Table 2).
The patient’s blood laboratory test results.

PaO2, partial pressure of oxygen; FiO2, fraction of inspired oxygen; SFC, spot-forming cells; PBMCs, peripheral blood mononuclear cells; “–” indicates test not performed.
Results of the laboratory analysis of the pleural effusion.
After initiating therapy, the patient’s body temperature gradually returned to normal, the shortness of breath resolved, the chest pain decreased markedly, and the cough resolved. On 23 May 2022, the cytology results revealed a large number of lymphocytes, small number of neutrophils and mesothelial cells, a very small number of eosinophils, and no tumor cells.
On 24 May 2022, considering the pleural fluid adenosine deaminase (ADA) concentration of >45 U/L, tuberculosis infection T cell test result of 61 (reference ≤11) spot-forming cells (SFCs)/2.5 × 105 peripheral blood mononuclear cells (PBMCs), positive tuberculin test result, elevated erythrocyte sedimentation rate (ESR), 90% mononuclear cells and a large number of lymphocytes in the pleural fluid, tuberculosis and tuberculosis pleuritis were considered likely. Therefore, the patient was transferred to an infectious disease hospital for further diagnosis and treatment. However, on 27 May 2022, the pleural fluid culture results were available and indicated the presence of Brucella. We immediately contacted the patient by telephone to relay the result, and we informed the patient’s attending physician at the infectious disease hospital. On 30 May 2022, the tiger red plate agglutination test results showed a titer of 1:400 (+ + +). Therefore, the diagnosis was brucellosis pneumonia with brucellosis pleurisy, and the patient was treated with rifampicin (600 mg, qd, orally (PO)) and doxycycline (0.1 g, every 12 hours (BID), PO). After 12 weeks of oral treatment, follow-up chest X-ray at a local hospital indicated that the pleural effusion and pneumonia had resolved completely, and the patient reported no discomfort. The short-term curative effect was excellent To date, the patient has reported no renewed discomfort and no recurrence of the disease, by telephone follow-up.
Discussion
Brucellosis is caused by infection with Brucella bacteria. Clinical manifestations vary and may persist for a few days or possibly, years. 3 Treatment is often delayed because of misdiagnosis. 5 There are approximately half a million new infections reported worldwide each year, 6 with a large number of livestock infections, which has a large economic impact. A main route of Brucella infection in the respiratory system is aerosol transmission,7,8 and subsequent blood transmission may be the most important route of lung infection.8–10 A meta-analysis of 503 Chinese brucellosis patients by Zheng et al found that 13% of the patients had concurrent respiratory symptoms, including cough, pneumonia, bronchopneumonia, pleural effusion, respiratory failure, and pulmonary embolism; however, only three patients (0.6%) had pleurisy-related chest pain. 11 Solera et al reported that approximately 6.9% of patients had respiratory involvement in brucellosis and approximately 2.3% developed pleurisy-related chest pain. 10 Brucella pleurisy has a low incidence and is easy to misdiagnose. 12
Analysis of pleural fluid in Brucella pleurisy has shown that exudative effusion is accompanied by high ADA concentrations, low glucose concentrations, and the fluid contains predominantly lymphocytes, similar to tuberculous pleurisy, which makes distinguishing the two conditions difficult. 13 A large literature review found that the dominant cell type in pleural effusion caused by Brucella pleuritis was mononuclear cells, 14 and ADA concentrations were increased compared with normal concentrations12,15,16. In some patients, the ADA concentration was >45 U/L.13,17 Generally, ADA concentrations >40 U/L are considered to indicate tuberculous pleurisy. 18 Therefore, it is easy to misdiagnose tuberculous pleural effusion in patients with brucellosis pleurisy if the ADA concentration is >45 U/L.
In the present case, analysis of the pleural effusion indicated exudation comprising 90% mononuclear cells, ADA concentration in both measurements >45 U/L, high levels of tuberculous T cells, positive tuberculin test result, and rapid increase in the ESR, all of which indicated tuberculous pleural effusion. Additionally, the patient had no history of raising livestock or contact with livestock, no history of ingesting raw milk, and reported only one episode of eating cooked mutton, which did not easily indicate Brucella infection. Therefore, our patient and similar patients are prone to misdiagnosis, incorrect treatment, and delayed diagnosis.
Both antibiotics and the course of treatment differ greatly between brucellosis and tuberculosis. Antibiotics for brucellosis are usually a combination of two antimicrobials, and the most commonly used antibiotic regimen is doxycycline combined with rifampicin for 6 weeks. 19 The combinations of other antibiotics or chemotherapeutics are also used in the treatment of brucellosis, such as fluoroquinolones or cotrimoxazole with rifampicin, doxycycline-streptomycin, and doxycycline-rifampicin. 19 The standard treatment for tuberculosis comprises 2 months of quadruple therapy with isoniazid, rifampicin, ethambutol, and pyrazinamide, followed directly by 4 months of rifampicin and isoniazid. 20 Extrapulmonary and disseminated forms of tuberculosis sometimes require longer treatment, especially for disseminated tuberculosis, and treatment should be tailored to the course of the disease. 20 Brucellosis treated as tuberculosis leads to inappropriate antibiotic use and a long course of treatment.
In conclusion, brucellosis pleurisy should be considered a differential diagnosis in cases of pleurisy to minimize the misdiagnosis rate and inappropriate antibiotic use in areas with a high prevalence of brucellosis. The reporting of this study conforms to the CARE guidelines. 21
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231187952 - Supplemental material for Brucella pleuritis misdiagnosed as tuberculous pleuritis: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605231187952 for Brucella pleuritis misdiagnosed as tuberculous pleuritis: a case report by Yong Yang, Ke-Liang Liu, Rui Zhao and Xiao-Yue Chang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231187952 - Supplemental material for Brucella pleuritis misdiagnosed as tuberculous pleuritis: a case report
Supplemental material, sj-pdf-2-imr-10.1177_03000605231187952 for Brucella pleuritis misdiagnosed as tuberculous pleuritis: a case report by Yong Yang, Ke-Liang Liu, Rui Zhao and Xiao-Yue Chang in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605231187952 - Supplemental material for Brucella pleuritis misdiagnosed as tuberculous pleuritis: a case report
Supplemental material, sj-pdf-3-imr-10.1177_03000605231187952 for Brucella pleuritis misdiagnosed as tuberculous pleuritis: a case report by Yong Yang, Ke-Liang Liu, Rui Zhao and Xiao-Yue Chang in Journal of International Medical Research
Footnotes
Author contributions
Ke-Liang Liu and Rui Zhao collected the clinical data. Yong Yang and Xiao-Yue Chang wrote and revised the manuscript.
Data availability statement
Data can be obtained from the corresponding author upon request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
Written informed consent was obtained from the patient for treatment and for the publication of this case report. The manuscript has been reviewed and approved for publication by the Research Department of Baotou Central Hospital (approval number: KYLL2022(伦)015).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.