
Abstract
Background: According to the World Health Organization, teenage pregnancies are high-risk due to increased risks of fetal and infant morbidity and mortality. This study compares adverse fetal outcomes between teen and adult pregnant women from rural Eastern Ethiopia. Methods: Institutional-based cross-sectional study was conducted among women visiting maternity units from surrounding rural areas. A total of 481 teenagers (13-19 years old) and 481 adults (20-34 years old) women with a singleton pregnancy were included in the study. Two hospitals and 3 health centers were selected in Eastern Hararghe Zone, Eastern Ethiopia. Comparative analysis was carried out using the log-binomial regression model to identify factors associated with adverse fetal outcomes in both categories. The results are reported in adjusted prevalence ratios with 95% confidence intervals. Results: High proportion of adverse fetal outcome was observed among teenage women than adult (34.9% vs 21%). Statistically significant difference (P < .05) in the proportion of low birth weight (21.1% vs 9.3%), preterm birth (18.7% vs 10.6%), APGAR score at 5th minute (9.3% vs 4%) were found in teenagers compared to adult women. Antenatal care attendance (APR = 0.44; 95% CI: 0.23, 0.86); eclampsia (APR = 1.96; 95% CI: 1.26, 3.06); pre-eclampsia (APR = 1.73; 95% CI: 1.12, 2.67); and wealth index (rich) (APR = 0.55; 95% CI: 0.32, 0.94) were significantly associated with adverse fetal outcomes among the teenage women. Whereas intimate partner violence (APR = 2.22; 95% CI: 1.26, 3.90); preeclampsia (APR = 3.05; 95% CI: 1.61, 5.69); antepartum hemorrhage (APR = 2.77; 95% CI: 1.73, 4.46); and hyperemesis gravderm (APR = 1.75; 95% CI: 1.09, 2.79) were significantly associated with adverse fatal outcomes among the adult women. Conclusion: teenage pregnancy is associated with a high rate of adverse fetal outcomes. Early identification and treatment of problems during antenatal follow-up should be the mainstay to avert the massive adverse fetal effects.
Background
Pregnancy during teenage remains a significant public health concern worldwide.1,2 World Health Organization considers teenage pregnancies as high-risk pregnancies, 3 as it is associated with various adverse maternal and fetal outcomes.4,5 The chance of dying from pregnancy-related causes is far higher for adolescents than older women. 6 Worldwide, 70,000 adolescent mothers die annually from complications associated with pregnancy. An estimated 1 million infants born to those teenagers die before the age of 1 year. 7
Several studies have reported that teenage pregnancy and delivery are associated with adverse neonatal outcomes such as preterm delivery,8-13 low birth weight (LBW) infants,11-16 premature babies 16 compared to older women. However, some studies showed the contrary and reported that mean birth weight and mean gestational age at delivery are not different between babies born from adolescents and adult women, 17 and no significant difference in admission to the special care unit, perinatal mortality rate, and early neonatal complications between those group. 18
The observed association between adverse birth outcomes and teenage pregnancy resulted from biological immaturity or sociodemographic environment where the pregnant women belong remains controversial; 12 indicates an increased risk associated with maternal age, pregnancy weight gains, and pre-pregnancy nutrition status with the pregnancy outcome for adolescents. 19 Inconsistent and inadequate prenatal care has also been found to be associated with adverse birth outcomes and teenage pregnancy.14,20
Some literature has reported the association of adolescent childbearing and outcomes confounded by social and environmental factors. In most societies, adolescent childbearing is related to low socio-economic status and behavioral factors such as poor education, not married, minority ethnic group, and poor prenatal care.16,21,22 These factors contribute to varying degrees to the pregnancy outcome. The debate continues the influence of socio-demographic and economic factors compared to intrinsic factors such as age, yet both are important to consider in improving the health of young women and their children.
Whichever the case, many of the maternal and fetal indicators are worse for teen women compared to older women. Due to the high morbidity and mortality and poor fetal outcomes, indicators related to teenage mothers will be a good reference in determining the general women’s health status and develop effective healthcare interventions in a society. 23
In Ethiopia, adolescent women aged 15 to 19 comprise nearly a quarter of the female population and contribute to 12% of all births. 24 Despite the high percentage of births from this group, there is limited information about fetal outcomes of teenage pregnancy. Existing studies focused on all clients visiting major hospitals in cities and towns, and most importantly, those studies used retrospective clinical data recorded, which are mostly incomplete and not well documented25-27 Women visiting rural hospitals and health centers, and most importantly, rural women are largely forgotten. Despite there is no difference in the type of perinatal care given for teen and adult women as in our setting, it is essential to assess whether there is an increased risk of adverse fetal outcomes among teen pregnant women compared to the adult one. Therefore, this study aimed to investigate adverse fetal outcomes among teen and adult pregnant women in rural Eastern Ethiopia.
Materials and Methods
Study Design and Population
An institutional-based comparative cross-sectional study was conducted among rural teen (13-19 years old) and adult (20-34 years old) pregnant women with singleton pregnancies seeking maternity care in Hiwot Fana Specialized University Hospital in Harar and Haramaya Hospital, Kersa, Weter and Langay Health Centers, in Eastern Hararghe, Oromia, Eastern Ethiopia from January to May, 2020. Women with a history of a medical condition before the current pregnancy (e.g., any cardiac, autoimmune disease or endocrine disorder, hypertension, diabetes mellitus) were excluded from the study.
We included all rural women from the East Hararge area who came for labor and delivery services in those selected health facilities. Three health centers and 2 hospitals were selected based on the referral chain that the zone health system follows.
Sample size for this study was calculated using double population proportion formula, 28 using the following assumption: two-sided 95% CI, 80% power, the ratio of teenage to adult women of 1 to 1, and a non-response rate of 5%. Utilizing previously conducted studies,25,29-32 the proportions of maternal and fetal outcomes among teenagers and adult were selected, the variable which resulted in the highest sample size was used. Consequently, episiotomy from a study conducted in Cameroon 29 resulted in a final sample size of 962 women (481 teenagers and 481 adult women). The total sample has been proportionally allocated to the 5 health facilities based on their previous year’s client flow.
Data Collection
Data were collected using a structured questionnaire adapted by reviewing related published reports on teenage pregnancy and an Ethiopian Demographic and Health Survey (EDHS) document.30,32-36 Trained BSc and MSc midwives participated in data collection and supervision. Training on content, how to collect data and how to deal with ethical issues at the time of data collection was given to data collectors and supervisors.
Pretest was done to check the applicability of material in a different health facility, and necessary adjustments were made to suit the context. Fieldwork manual and ethical issue manual were provided for data collectors and supervisors while administering the data collection. The collected data were checked for completeness daily.
Study participants were assessed for eligibility (women free from any medical disorder before their current pregnancy and singleton pregnancy) and recruited after they were admitted to the maternity ward for labor and delivery at selected health facilities. Women who fulfilled the criteria were interviewed and followed until discharged from health facilities.
Variables and Measurements
In this study, the adverse fetal outcome were the main outcome variables. It was defined as the occurrence of one or more of the following fetal outcomes: LBW (delivery of a live infant whose birth weight was less than 2500 g),37,38 preterm (babies born alive before 37 weeks of pregnancy are completed), 39 low Apgar score at 5 minutes (less than 7), neonatal death (death of a live birth within 28 days), 12 stillbirth (fetal death at or after 28 weeks gestation). 29 The wealth index was generated using 26 variables. The principal component analysis (PCA) method was used to calculate the distribution of wealth using the following variables: number of animals owned (ox, cow, horse, donkey, sheep, goat, chickens), owner and size of farmland, owner house, household characteristics, household facilities and infrastructure like electricity, toilet, phone, refrigerator, radio, TV, bed, watch, car. Seven components whose eigenvalue was greater than 1 was selected. Finally, the components were categorized into 5 quantiles with the lowest score representing the very poor as 1, poor as 2, medium as 3, rich as 4, and very rich as 5.
Data Management and Analysis
Throughout the data collection period, the data were checked daily. The data were double entered and cleaned using EpiData version 3.1 and analyzed using Stata version 14 statistical software. Descriptive statistic like frequency tables for categorical variables, mean, standard deviation (SD) for continuous variables, and proportion with 95% confidence interval (categorical variables) were used to represent the data. Chi-square test was used to compare categorical data between teenagers and adult women. Log-binomial regression model was used to identify the factors associated with adverse fetal outcomes in both teenagers and adult women. In bivariate analysis, the explanatory variables with a P-value ≤0.25 were considered as a candidate for multivariable analysis and adjusted prevalence ratio (APR) was estimated at 95% CI and P-value <0.05 in multivariate analysis was used to state statistical significance. Before the final model, the explanatory variables were checked for multi-collinearity using the correlation matrix for the regression coefficient and standard errors. Model fitness was assessed using Hosmer and Lemeshow goodness-of-fit tests.
Ethical Consideration
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (Ref.no. IHRERC/106/2020) at the College of Health and Medical Sciences, Haramaya University. Informed written consent was obtained from the study participants.
Results
Characteristics of Study Participants
Nine hundred sixty-two women were included in this analysis. The mean age for teenagers and adult women were 18 (±04) and 26 (±0.18) years, respectively. Among the participants, 301 (62.6%) teenage and 241 (50.1%) adult women attended school. The majority, 461 (95.8%) of the teenagers and 558 (95.2%) of the adult women were Oromo in ethnicity. Most of the study participants, 457 (95%) of teenagers and 475 (98.7%) of adult women were married. Almost two-thirds of teenagers (65.5%) and over half (59.7%) of adults were housewives (Table 1).
Characteristics of Study Participants, Eastern Ethiopia, 2020 (n = 962).
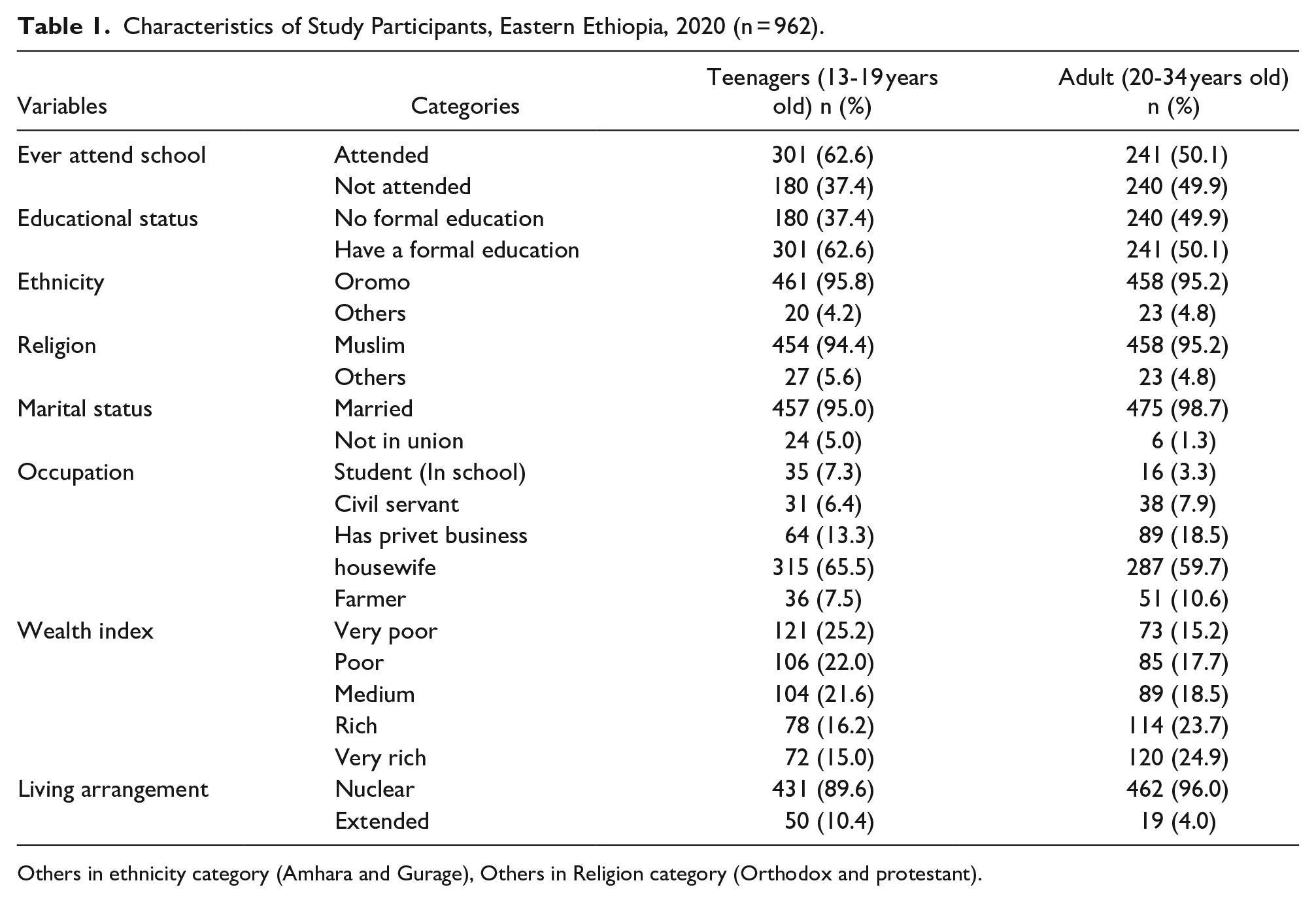
Others in ethnicity category (Amhara and Gurage), Others in Religion category (Orthodox and protestant).
Obstetrics Characteristics of Study Participants
Fewer teenagers had antenatal follow-up compared to adults, 313 (65.1%) versus 359 (74.6%) for the current pregnancy respectively. Over half, 296 (61.5%) teenagers and 333 (69%) adults, took iron/folic acid during antenatal care visits. Only 87 (18.1%) of teenagers and 131 (27.2%) of adults chewed khat during the current pregnancy (Table 2).
Obstetric Characteristics of Study Participants, Eastern Ethiopia, 2020.

Characteristics of Newborn
Ninety (18.9%) and 51 (10.6%) of teenagers and adult women had preterm delivery, respectively. Most of the fetal presentations were cephalic, 461 (95.8%) teenage and 439 (91.2%) adult women. Over half, 291 (60.2%) of newborn babies among teenagers and 282 (58.6%) among adult women were male. There were 21 (4.4%) stillbirths in teenagers and 28 (5.8%) among adults. Additionally, 8 (1.7%) and 10 (2.1%) neonatal deaths occurred among teenagers and adults, respectively. Seventy-one (15.4%) of newborn babies from teenagers and 45 (9.9%) from adult women were admitted to the neonatal intensive care unit (NICU), about half (50.7%) of teenage babies were admitted because of asphyxia followed by prematurity 18 (25.4%) and 12 (33.3%) of adult babies were admitted because of prematurity followed by infection 12 (26.7%) (Table 3).
Characteristics of Newborn Included in the Study, Eastern Ethiopia, 2020.
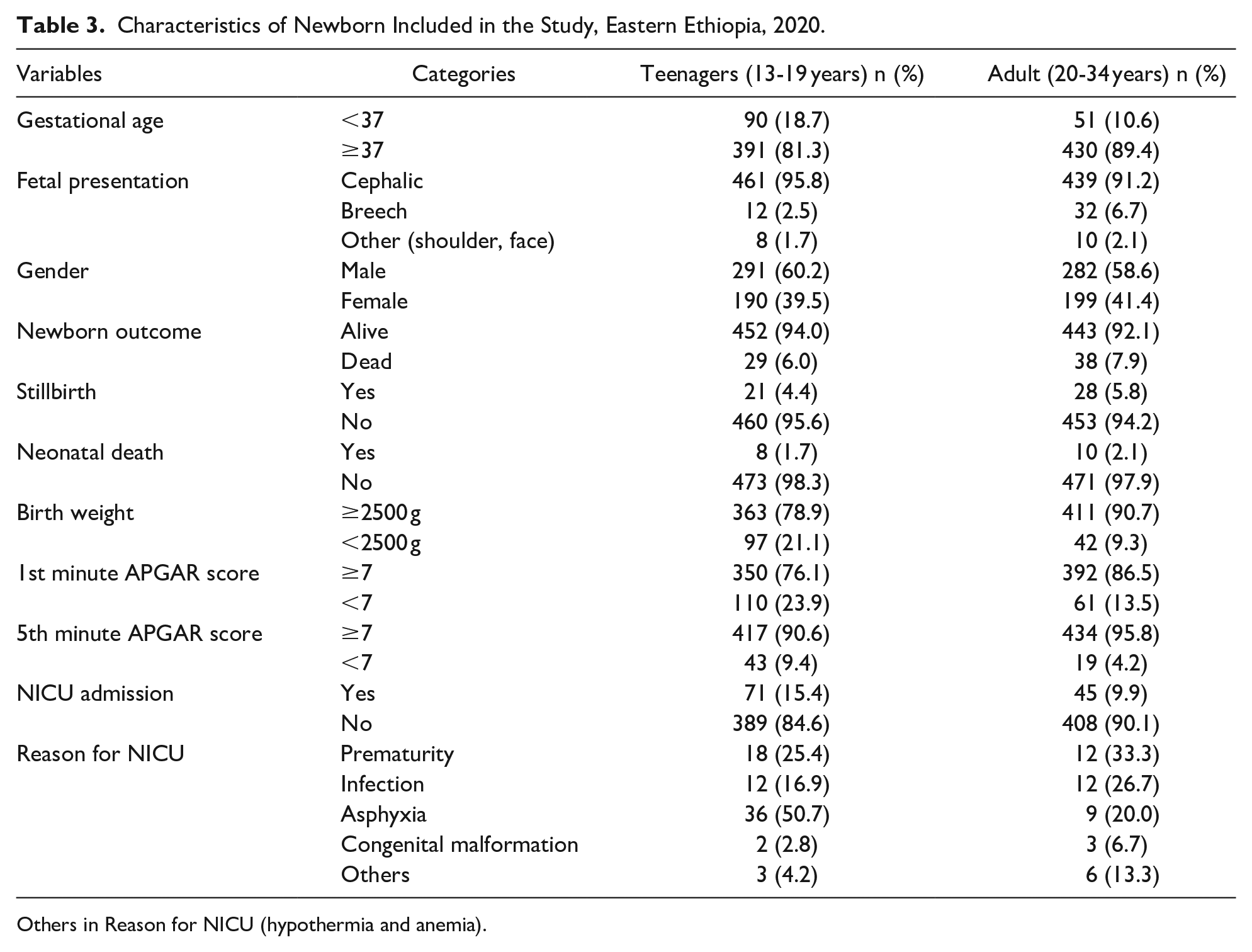
Others in Reason for NICU (hypothermia and anemia).
Adverse Fetal Outcomes among Babies from Teen and Adult Women
Ninety-seven (21.1%) of the teenage women delivered low birth weight babies compared with 42 (9.3%) of adult women, (P ≤ .001). There were 90 (18.7%) preterm babies born to teenage women compared with 51 (10.6%) adult women (P ≤ .001). The 5 minute Apgar scores were less than 7 in 43 (9.3%) babies born to teenage women compared with 19 (4%) babies born to adult women (P = .002). Twenty-one (4.4%) of stillbirth babies born from teenage women compared with 28 (5.8%) of adult women (P = .305). Eight (1.7%) neonatal deaths occurred in babies born from teenagers compared with 10 (2%) in babies from adult women (P = .634). One hundred sixty-eight (34.9%) of the total adverse fetal outcome occurred in teenage women compared with 101 (21%) to adult women (P ≤ .001) (Table 4). A higher proportion of teenagers compared to adult women had adverse fetal outcome (34.9% vs 21%). Thirteen percent of newborn babies of teenage women had 2 or more adverse fetal outcomes compared with 6% in adult women (Figure 1).
Comparison of Adverse Fetal Outcomes Among Study Participants, Eastern Ethiopia, 2020.


The occurrence of adverse fetal outcomes among participants, Eastern Ethiopia, 2020.
Factors Associated with Adverse Fetal Outcome
In the multivariable analysis, antenatal care attendance decreases the prevalence ratio of adverse fetal outcome by 56% among teenage women (APR = 0.44; 95% CI: 0.23, 0.86) but failed to show statistical significance association in adult women (APR = 0.61; 95% CI: 037, 1.01). The prevalence ratio of adverse fetal outcome was 1.96 times higher in teenage women who had eclampsia compared to those who had no eclampsia (APR = 1.96; 95% CI: 1.26, 3.06), however, there was no association in crude analysis for adult women. Also, the prevalence ratio of adverse fetal outcome was 1.73 times more in teenage women with preeclampsia compared to those without preeclampsia (APR = 1.73; 95% CI: 1.12, 2.67). Preeclampsia also shows an association in adult women. Adult women who had preeclampsia were 3.05 times more likely to have had an adverse fetal outcome compared to those without preeclampsia. (APR = 3.05; 95% CI: 1.61, 5.69).
The prevalence ratio of adverse fetal outcome decreases by 45% in teenagers whose economic status was rich than very poor (APR = 0.55; 95% CI: 0.32, 0.94), in adult women no association was seen in crude analysis. The prevalence ratio of adverse fetal outcome was 2.22 times higher in adult women who had exposure to intimate partner violence during pregnancy (APR = 2.22; 95% CI: 1.26, 3.90). No association was observed in adjusted analysis for teenage women (APR = 1.39; 95% CI: 0.99, 1.96). The prevalence ratio of adverse fetal outcome was 2.77 times higher in adult women who had antepartum hemorrhage (APH) during pregnancy compared to those who had no bleeding (APR = 2.77; 95% CI: 1.73, 4.46). However, no association was found in teenage women through adjusted analysis (APR = 1.13; 95% CI: 0.54, 2.36). The prevalence ratio of adverse fetal outcome among adults with hyperemesis gravidarum during pregnancy was 1.75 times higher than those without (APR = 1.75; 95% CI: 1.09, 2.79). In teenage women no association was seen in crude analysis. Tables (5 and 6).
Regression Analysis on Selected Characteristics of Respondent by Adverse Fetal Outcomes Among Teenage Participants, Eastern Ethiopia, 2020.

P < .05.**P < .01. ***P < .001.
Regression Analysis on Selected Characteristics of Respondent by Adverse Fetal Outcomes Among Adult Participants, Eastern Ethiopia, 2020.
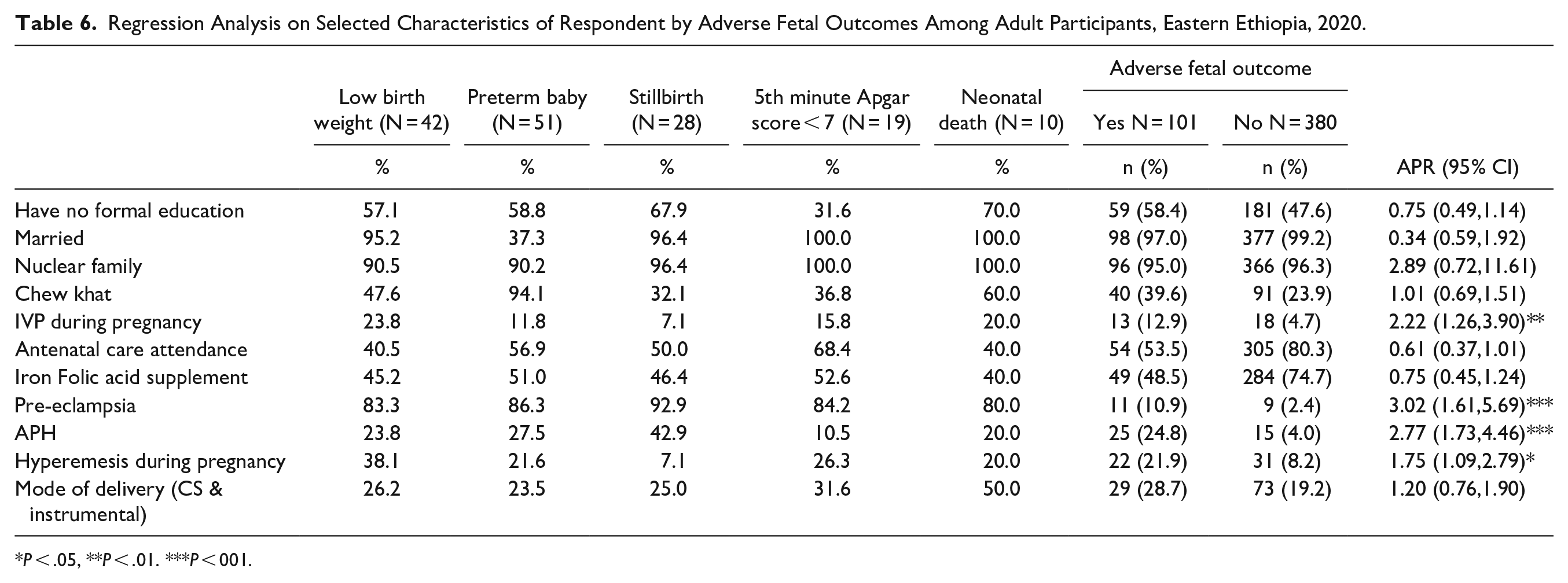
P < .05, **P < .01. ***P < 001.
Discussion
The prevalence of adverse fetal outcome among teen women was 34.9% compared to 21% among adult women. The proportion of low birth weight, preterm baby, and lower Apgar scores at 5 minutes were higher in teenagers compared to adult women. The prevalence of adverse fetal outcome was low among teenagers who attended antenatal care and in the rich wealth index, while adverse fetal outcome prevalence was high among teenagers who had eclampsia and pre-eclampsia. Intimate partner violence (IPV), pre-eclampsia, antepartum hemorrhage (APH), and hyperemesis gravidarum were identified as factors associated with adverse fetal outcomes among adult women.
In this study, 21% versus 9.3% of low birthweight babies delivered from teen and adult women, respectively. This finding is in line with other studies in Northern Ethiopia, 27 Cameroon, 30 and a multicounty study by World Health Organization in 29 countries in Africa, Latin America, Asia, and the Middle East revealed comparable results. 40 This might be due to low socio-economic status, and anatomical immaturity. Also, teenagers themselves are in a state of continued growth, in addition to the added requirements of pregnancy, could contend with the developing fetus for nutrients.
This study revealed that 18.7% versus 10.6% of premature babies delivered from teenagers and adult women, respectively. This finding agrees with a previous study from India 10 and a study by Mombo-Ngoma et al 41 in 4 Sub-Saharan African countries. The mechanisms by which teenage pregnancy contributes to preterm birth could be attributed to the immaturity of cervical blood supply stimulates prostaglandin production that could lead to preterm birth. 12 Additionally, small uterine volume and short cervix (<25 mm) are more common in younger mothers, leading to preterm delivery. 42 Furthermore, young mothers are emotionally unstable due to several reasons including socio-economic problems, living under poor social circumstances which might be responsible for increasing the risk of preterm labor.27,43
The Apgar score is a key component in the early evaluation of infant health to monitor the physical condition of newborns. In the present study, it was found that the 5-minute Apgar scores were less than 7 in 9.3% of babies born to teenage women compared with 4% of babies born to adult women. This finding is in line with another study in Cameroon. 30 Our study results found no statistically significant difference observed between teenage and adult women regarding stillbirth which is consistent with studies from Zambia 44 and Cameroon. 29 And also in line with another study, 30 neonatal death showed no significant difference between the 2 group.
ANC promotes the health of pregnant women and is strongly associated with better maternal and neonatal outcomes.45,46 The prevalence ratio of adverse fetal outcome decreases in teenage women who attended antenatal care. This finding is in line with previous study conducted in Ethiopia that found antenatal care attendance decreases the odds of low birth weight and preterm baby. 32 This study shows 34.9% of teens and 25.4% of adult women did not attend antenatal care, consistent with this finding are studies from Turkey, 47 and Thailand, 48 indicating fewer antenatal care visits among adolescent than adult women. The difference in educational status between adult and teenage women might contribute to this. 46 Education increases women’s autonomy, builds confidence, and promotes the capability to make decisions. 49 A significant number of adolescents in Sub-Saharan Africa do not access to maternity services and use them during pregnancy especially in rural areas. 50
Maternal health problems during pregnancy, like hypertensive disorder is implicated with the occurrence of adverse birth outcomes. 51 This study found the prevalence ratio of adverse fetal outcome increases among women with pre-eclampsia and eclampsia. This is in agreement with previous studies from Ethiopia where pre-eclampsia increases the risk of delivering premature babies. 32 This was also found in Brazil 52 and Uganda. 53 Hypertensive disorders of pregnancy complicate around 6% of all pregnancies in Ethiopia and are one of the common causes of perinatal and maternal morbidity and mortality. 54 Reduced placental perfusion leads to a reduction in the blood supply of oxygen and nutrients required for fetal growth and well-being. 55
Socio-economic disadvantage has been repeatedly linked with poor teenage pregnancy outcomes. 56 This study found that adverse fetal outcomes were significantly lower in teenage women in rich wealth status compared to those in very poor wealth status. Congruent to this study, a review was done in Canada that also found low socio-economic status as an indicator for poor pregnancy outcome in adolescent mothers. 57 Another study in the same country indicated the odds of adverse pregnancy outcomes were high in rural pregnant adolescents with low socio-economic status. 58
Our study found that intimate partner violence (IVP) during pregnancy was significantly associated with adverse birth outcomes in adult women. This finding is in line with other studies from Ethiopia 59 and Nigeria 60 which supports the finding that IVP during pregnancy increased the risks of preterm birth (PTB) and low birth weight (LBW). IPV during pregnancy affects both the women and the growing fetus. Direct trauma to the pregnant women and the physiological effects of stress may affect fetal growth and development. 61 IPV may lead to chronic psychological stress and raise stress hormone levels like cortisol that may hinder the body’s immune function, which may be associated with an increased risk of preterm labor. 62 It is essential to screen, advise, treat and provide clinical follow-up for suspected or abused pregnant women. Also, the health care worker must warn couples during antenatal care follow-up about the possibility of IPV exposure and stress to the fetus.
Newborn fetal health and maternal health are closely linked. Poor fetal outcome is highly associated with poor maternal health during pregnancy. As shown in this study, adult women with antepartum hemorrhage (APH) had an increased risk of adverse fetal outcomes. In agreement with our study, other studies have reported an association between APH and preterm delivery, low birth weight, and stillbirth, 63 and preterm delivery. 64 Repeated small antepartum placental hemorrhages causing chronic placental insufficiency may result in low-birth-weight babies, fetal growth restriction, and preterm labor. 65 Appropriate treatment of expectant women with APH may minimize perinatal morbidity and mortality.
This study found the odds of adverse fetal outcomes was increased among women who had hyperemesis gravidarum (HG) during pregnancy. A systematic review conducted in the Netherlands indicated adverse fetal outcomes such as pre-term deliveries and low birthweight neonates associated with women with HG. 66 Also, a study conducted in Nepal showed the association of preterm babies and HG. 67 HG has different physiological consequences for the mother, such as dehydration, electrolyte imbalances, and severe loss of weight, as well as concern about the effects of babies. 68
The primary nature of the data used in this analysis and the inclusion of outcomes including stillbirths and neonatal deaths significantly improves the comprehensiveness of the study for the health facility delivery as opposed to other studies focusing only on few outcomes. It also followed neonates until discharged from the health facility. Yet, as the study focused on women who visited health facilities for maternity care, it might suffer from selection bias which readers are advised to note. Furthermore, we did not assess the health facilities’ factors. We recommend future research including those factors.
Conclusion
The proportion of adverse fetal outcomes is higher among teens compared to adult women. Low birth weight, preterm baby, and lower 5-minute Apgar score were more common among teenage pregnant women. Antenatal care attendance and being among the rich family decreases the adverse fetal outcome while, pre-eclampsia and eclampsia were positively associated with adverse fetal outcomes among teen women. Intimate partner violence, pre-eclampsia, ante partum hemorrhage, and hyperemesis gravidarum were positively associated with adverse fetal outcome among adult women.
To minimize the high rate of fetal and newborn morbidity and mortality among babies born from teen women, addressing the sexual and reproductive health needs is crucial. This study recommends the need to strengthen maternal health services and to improve the quality of antenatal care and subsequently increasing in service use by teen pregnant women. Improving compliance with prenatal care to decrease adverse outcomes is an important part of improving reproductive healthcare. The health care providers should identify and treat pregnant women suffering from intimate partner violence. Early screening and treatment of pregnant women with those identified pregnancies related problems, during antenatal care, labor and childbirth are strongly recommended.
Footnotes
Acknowledgements
We would like to acknowledge Haramaya University for financial support. We also thank all study respondents for their voluntary participation. We extend our gratitude for Dr Tara Wilfong for her valuable comments and language edition as well as the study participants and data collectors for their generous cooperation.
Author Contributions
All authors made a substantial contribution to the conception, design, acquisition, and interpretation of data. All authors have revised the article critically for important intellectual content. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclose receipt of financial support from Haramaya University, Ethiopia. The funder has no role in designing the study and collection, analysis, and interpretation of data and in writing the manuscript.
Availability of Data and Materials
All data related to this study are presented in this manuscript. The dataset of this article is available from the authors upon reasonable request.