
Abstract
Malignant bone tumors (MBT) account for 3% to 5% of cancers in children younger than 15 years. We aimed to report the outcome of children with MBT in 10 years in Southern Iran. During the study period, 100 patients (57 Osteosarcoma, 43 Ewing sarcoma) with an M/F ratio of 1.56 and a median age of 13.8 years (3.8-17.9) were diagnosed. Metastasis occurred in 27% of patients, mostly in the first 3 months of diagnosis. The mean survival time of MBT altogether was 94.1 months (95% CI: 86.5-101.7). The 5-year overall survival and event-free survivals were 85.2% (95% CI: 74%-91.8%) and 69.2% (95% CI: 56%-79%), respectively. Metastasis was the only independent risk factor of death in our study cohort (Hazard ratio 36.7, 95% CI: 4.8-282.6, P = .001) MBT in children mostly occur in adolescent boys. About one-third of them become metastatic, which is significantly associated with poor outcomes.
Introduction
Cancer is the second most common cause of death worldwide after heart disease. Primary bone tumors are the fourth cause of death among malignant carcinomas after lung, prostate, and breast cancer and the third fetal cancer in pediatrics. 1 Malignant bone tumors (MBT) in children represent 3% to 5% of cancers in children younger than 15 years. 2 The prevalence is almost doubled (7%-8%) in adolescents between the age of 15 to 19 years. 3 The pathogenesis of cancer is multifactorial, with the interaction of environmental risk factors in a genetic predisposition. Primary bone tumors are more prevalent in children and young adolescents than in the adult population. The peak incidence of malignant bone tumors is in adolescents when the pubertal growth spurt is considered a precipitating factor. Previous exposure to radioactive waves increases the risk of malignant bone tumors. Boys are more frequently affected. It is also seen more often in the white race in a subgroup of bone tumors. Some hereditary syndromes like Li-Fraumeni syndrome, Rothmund-Thomson syndrome, and hereditary retinoblastoma are associated with a high risk of bone tumors. 4
While primary bone tumors in children are often benign, MBT causes significant mortality and morbidity among children and adolescents. The presenting symptoms of malignant bone tumors are quite variable in children making it difficult to diagnose early. 5 Pain and swelling of the involved bone are the most prevalent initial symptoms. Usually, the pain is nocturnal that is worsened by activity, and is intensified in the later stages of the disease. Other clinical presentations include detecting a palpable mass in bones, limitation of range of motion, limping, vascular and neurological deficits, dyspnea, skin changes, and pathological fractures. Fever, weight loss, and night sweating are systemic symptoms that usually occur in metastatic cases. 6
The 2 main categories of malignant bone tumors in children are Osteosarcoma and Ewing sarcoma (EWS) or primitive neuroectodermal tumor (PNET), accepted by the International Classification of Childhood Cancer (ICCC). 7 Other rare subgroups include chondrosarcoma, chordomas, malignant fibrous neoplasms, odontogenic tumors, and unspecified neoplasms. Most of these patients had a subclinical metastatic disease at the time of diagnosis of cancers, even if clinical metastasis is absent. 8
The data on the epidemiology of pediatric malignant bone tumors in Iran is scarce. A previous study in our center reported the epidemiology of musculoskeletal tumors in children and adults in 1997 to 2008. 9 This study aims to report the clinical characteristics and outcomes of children with malignant primary bone tumors in 10 years since 2008.
Methods
This cross-sectional study was performed in Amir Oncology hospital, the primary referral center of children with cancer in Shiraz, Southern Iran, in 2008 to 2018. We reviewed the medical files of 18 years old or younger patients with a confirmed diagnosis of primary malignant bone tumors, including Osteosarcoma, Ewing sarcoma or PNET, chondrosarcoma, and other rare bone tumors according to ICCC. Those with metastatic bone tumors were not included in the study. The demographic data and information about the primary tumor site, initial clinical presentations, presence, and site of metastasis and children’s outcome were recorded from their medical files. Patients were contacted on the phone to follow if they were still alive at the time of the study. In the case of a death event, the time and cause of death were recorded. The Ethics Committee of Shiraz University of Medical Sciences approved the study protocol.
Statistical Analysis
We analyzed data with Statistical Package for Social Sciences (SPSS, V22, Chicago, IL, USA). We described quantitative data with median and range, mean and standard deviation (SD), number, and percentages. The Chi-Square test was used to compare qualitative and categorical variables. The independent sample t-test compared the quantitative variables between the 2 groups. The Kaplan-Meier survival analysis was used to estimate the survival times of malignant bone tumors and its subgroups using the Log-rank test to determine the impact of different covariates on bone tumor survival. The Cox regression analysis defined the independent variables affecting survival as the hazard ratio (HR) and 95% confidence interval (CI).
Results
During the study period, 100 patients with primary malignant bone tumors were diagnosed in our center, which consisted of 57 patients with Osteosarcoma and 43 patients with EWS. Other rare bone tumors were not reported in our registries during the study period. The general characteristics of the study population are demonstrated in Table 1.
Demographic Characteristics of Children With Malignant Bone Tumors in Southern Iran.
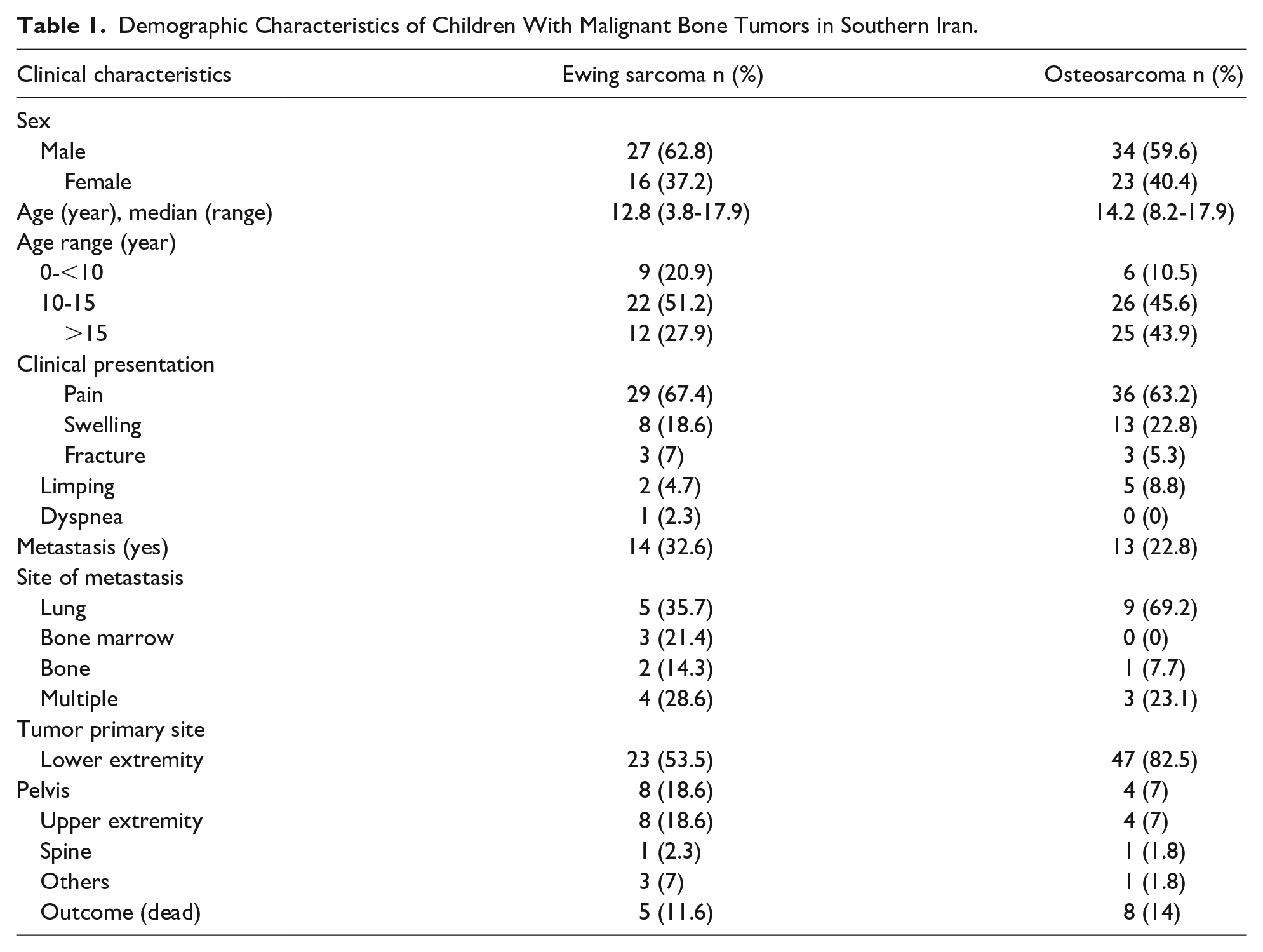
MBT had the highest prevalence in adolescent boys (M/F ratio: 1.56), mostly in ages 10 to 15 years (48%). The male predominance was more prominent in EWS than Osteosarcoma (M/F ratio of 1.69 vs 1.48). The median age of MBT altogether was 13.8 years (3.8-17.9), and 85% of them were older than 10 years. Patients with EWS were relatively younger than patients with Osteosarcoma (Table 1). Girls were generally younger at the time of initial diagnosis than boys in all MBT combined (mean difference 1.4, 95% CI: 0.1-2.7; P = .03). The difference was mostly attributed to patients with EWS (mean difference 2.4, 95% CI: 0.3-4.4; P = .026).
Long bones of the lower extremity (femur, tibia) were the most frequent primary tumor sites, especially in Osteosarcoma. They were followed by pelvis and shoulder in Ewing sarcoma and pelvis, humerus, and fibula in Osteosarcoma (Figure 1). Most patients declared that pain and swelling were the most common clinical presentations.

Prevalence of malignant bone tumors by site of presentation.
Patients with EWS experienced slightly more metastasis events than Osteosarcoma, but the difference was not statistically significant (32.6% vs 22.8%, P = .28). Lung was the most common site of metastasis in both groups, especially in Osteosarcoma. Most metastasis events (17 out of 27, 63%) occurred in the first 3 months after diagnosis (78% in EWS and 53% in Osteosarcoma).
We encountered 13 death events in our study population, including 5 deaths (11.6%) in EWS and 8 deaths (14%) in patients with Osteosarcoma (P = .72). Patients with EWS died of their illness very sooner than patients with Osteosarcoma. All deaths occurred in the first year of diagnosis in EWS, while 37.5% of deaths in children with Osteosarcoma occurred more than a year since diagnosis.
Figure 2 demonstrates the Kaplan-Meier survival curve of patients with MBT. The mean survival time for bone tumors altogether was 94.1 months (95% CI: 86.5-101.7), which was longer in EWS (96.1 months, 95% CI: 86.2-105.9) compared to Osteosarcoma (91.3 months, 95% CI: 79.9-102.7), but the difference was not significantly different (P = .68). The 5-year overall survival (OS) for MBT altogether was 85.2% (95% CI: 74%-91.8%), which was slightly higher in Ewing sarcoma than Osteosarcoma (88.2% [95% CI: 74%-95%] vs 83.3% [95% CI: 66%-92%]). The mean of event-free survival (EFS) time for MBT altogether was 81 months (95% CI: 72.1-90.0), which was not significantly different between the 2 groups of patients (P = .58). The 5-year EFS was 69.2% (95% CI: 56%-79%) in MBT altogether, which was similar in both subgroups (69% [95% CI: 50%-82%] in Osteosarcoma and 68.1% [95% CI: 47%-82%] in EWS).

Kaplan-Meier survival curve of children with primary malignant bone tumors.
Table 2 shows the impact of different covariates on the survival of children affected by bone tumors. Among different variables tested, including gender, age, the extent of disease, and tumor location, metastasis was the only variable that significantly lowered the survival rate (P < .001) (Figure 3). The Cox regression analysis confirmed that metastatic MBT increased the risk of death by about 40 times (Hazard ratio 39.8 [95% CI: 5.1-308.8], P < .001) (Table 3).
Univariate Analysis of the Impact of Different Variables on the Survival of Children With Malignant Bone Tumors.

In patients with Ewing sarcoma, no statistics were computed because no death event occurred in the non-metastatic group.
Cox Regression Model of Independent Variables Associated With Survival in Children With Malignant Bone Tumors.


Kaplan-Meier survival curve of patients with primary malignant bone tumor with and without metastasis.
Discussion
Primary malignant bone tumors are rare in children. Therefore, the data on the clinical course and outcome of this group of tumors is limited. We reported one of the largest studies in our region in a cohort of 100 children with MBT who were followed for a median follow up time of 2.6 years (0.3-9.1). Osteosarcoma was the most common MBT, which was found in 57% of cases. It is similar to many other reports from other centers (range 46.6%-59.5%).2,4,9-12 The boys were more frequently affected in all MBT, particularly in EWS. The male predominance of MBT, and EWS in particular, was reported in most other reports,2,11,13 while some reported an equal frequency in both genders. 10
Nearly half of our patients with MBT were adolescents with the age range of 10 to 15 years. It is the time when most children experience their pubertal growth spurt. Cotterill et al 14 previously delineated the association of bone tumors with rapid bone growth. They showed that patients with Osteosarcoma were generally taller than their age-sex-matched healthy controls. Also, patients with EWS younger than 15 years were significantly taller than the general population. Besides, those with Osteosarcoma of lower limbs were taller than those with tumors at other sites. As bones of lower limbs contribute more to the growth spurt than upper limbs, it is not unusual that taller adolescent boys during their pubertal growth spurts are very prone to MBT of lower extremities.
The 5-year OS and EFS in our patients with MBT were 85% and 69%, respectively. The survival probability was similar in patients with Osteosarcoma and EWS. Most previous studies reported a much lower 5-year OS both in children with Osteosarcoma (31.7%-72.6%) and EWS (19%-70%).2,15-23 Approximately 30% of our patients with MBT experienced metastasis. More than 60% of metastases occurred in the first 3 months from diagnosis and were associated with higher mortality. It was the only independent risk factor of mortality in our patients and increased the risk of death by more than 36 times. Many other reports reinforced that disseminated disease significantly reduced the survival rate.24-27 We did not find any association between age, gender, and tumor location and OS in our patients with MBT.
Several factors may affect prognosis in patients with MBT. The results of a large cohort study in the European and American Osteosarcoma Study (EURAMOS-1) on more than 2000 patients with Osteosarcoma revealed that metastatic disease, tumor location in the axial skeleton or proximal femur/humerus, male gender, being an adult or adolescent rather than a child, large tumor volume, and chondroblastic histology were associated with a more inferior EFS and OS. 17 Additionally, pathologic fracture adversely affected 5-year OS in adult patients with Osteosarcoma of extremities in a large cohort of patients registered in the Cooperative Osteosarcoma Study Group (COSS). 28 The surgical methods (limb salvage surgery vs amputation) seems to produce comparable outcomes regarding local control, but higher 5-year OS in patients undergoing limb salvage surgery. 29
A large retrospective cohort study utilizing data from the National Cancer Institute Surveillance Epidemiology and End Results (SEER) to define prognostic groups in patients with EWS revealed that patients older than 18 years with metastatic disease had the worst prognosis. On the other hand, the best prognosis was reported in children with localized disease outside the pelvis (5-year OS 79%, 5-year EFS 72%). 30 Tumor size, response to chemotherapy, time to diagnosis, surgical resection, and radiotherapy were also associated with outcome in some other reports.15,25,31,32
Treatment of MBT is primarily based on surgical resection of the primary tumor and neo-adjuvant chemotherapy. The primary tumor site’s surgical resection reduced overall mortality even in those with metastatic tumors at presentation. 31 Neo-adjuvant chemotherapy was not proven superior to adjuvant chemotherapy 33 however, it may facilitate tumor resection and allows assessment of tumor response to pre-op chemotherapy. 34 An extensive survey on patients with metastatic MBT at presentation showed that radiotherapy improved OS in patients with Ewing sarcoma but not those with Osteosarcoma. 31
Similarly, another study emphasized that radiation predicted worse outcome in Osteosarcoma, but was associated with a 24% improved OS and EFS in patients with Ewing sarcoma. 25 Generally, Osteosarcoma is considered a radioresistant tumor. However, in cases with unresectable tumors, particularly in axial sites or palliative care in symptomatic metastatic lesions, radiation can be used as an adjuvant treatment. 35
Given the relatively high rate of metastasis in patients with MBT, which leads to a dismal prognosis despite multimodal treatments, a timely diagnosis may guarantee a better outcome. Pain and swelling are the 2 most common symptoms of MBT, which are easily ignored since they are attributed to physical injuries that frequently happen in the teenage group. Limping is another prominent symptom that should be thoroughly evaluated. Though it is most often due to benign processes such as infections, inflammatory conditions, trauma, and overuse injuries, malignancies should be taken into account, especially when it takes too long to recover or other associated symptoms are present. 36
Our study faced some limitations. We did not have access to most patients’ operational data, including tumor volume and post-chemotherapy tumor necrosis. Therefore, their impact on the outcome of patients was not clear. Besides, we did not compare different treatment modalities to know which one has the best results in terms of OS and EFS. Moreover, due to small numbers of death events in our study cohort, the survival analysis results were not robust. Further multicenter studies with larger sample size and longer follow-up are needed to draw firm conclusions.
Conclusion
MBT occurs mostly in children around puberty. About one-third of them become metastatic even at presentation or during their treatment course. Metastasis adversely affects the outcome and is associated with a dismal prognosis.
Footnotes
Acknowledgements
We would like to thank the Vice-Chancellor of Research and Technology of the Shiraz University of Medical Sciences for its financial support. The study was relevant to the thesis of A. Sarfaraz with project No. 12272.
Author Contributions
M. Bordbar contributed to the study design, conception, and reviewing the manuscript. A. Sarfaraz have done data collection and drafting the manuscript. S. Haghpanah have done analysis and interpretation of data and editing the manuscript. O. Zekavat and S. Zareifar have data collection and editing the manuscript. T. Zarei have done drafting the paper, performed the research, and edited the final version. All author reads an approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.