
Abstract
Ewing’s sarcoma/primitive neuroectodermal tumor is rare and aggressive with a poor prognosis. Intraabdominal metastases are an uncommon condition. Metastasis in the lesser sac is an exceptional occurrence. To the best of our knowledge, this location has not been described previously. We report a case of a 15-year-old patient treated for Ewing’s sarcoma of the left arm 6 years back. She had developed a suspicious mass in the lesser sac 6 years following her primary tumor. The histopathologic exam revealed a tumor with “small round cells” that were positive for CD99, confirming the relapse of Ewing’s sarcoma. The relapse was successfully managed with chemotherapy and surgery. Intraabdominal, extraintestinal masses in patients treated previously for Ewing’s sarcoma should be considered as Ewing’s sarcoma relapse in the differential diagnosis. We fully describe the management of this atypical relapse, with different components of clinical, radiological, and histological findings.
Introduction
Ewing Sarcoma Family of Tumors (ESFT) are mainly aggressive bone sarcomas and can also occur in soft tissues. 1 It is an entity of small, blue, round cell neoplasms of neuroectodermal origin, comprising classical Ewing’s sarcoma (ES), primitive neuroectodermal tumors, and chest wall Askin tumors. 2 These sarcomas have high metastasizing potential. The lung, pleura, and other bones are the most common metastatic sites. 3 Thanks to multidisciplinary treatment, we have observed an increased survival. On the contrary, we have also detected more various other unusual metastatic sites such as the stomach, pancreas, small bowel, ovary, and brain.4–8
Metastatic Ewing’s sarcoma is primarily a severe systemic disease presenting as a diverse spectrum ranging from localized metastases to broadly a disseminated multiorgan disease with varied outcomes. With a single metastasis, the paucity of randomized evidence makes the management further challenging. 9
Despite aggressive chemotherapy and local therapy, the outcome of patients with upfront metastasis is poor with a long-term cure in 20%–30% of patients. 10 A meticulous selection of patients with metastatic disease can help salvage patients with aggressive systemic and local treatment. 11
In this report, we present the successful case management of a 15-year-old female with ES of the left arm that metastasized to the lesser sac 6 years after the initial diagnosis with a local recurrence, and without other sites or organ involvement. To the best of our knowledge, there are no reports of this unusual metastatic site of ES in the lesser sac.
Case report
A 15-year-old patient has been treated for bone ES of the left humerus at another facility. The chest computed tomography (CT)-scan, bone scintigraphy, and osteomedullary biopsy were negative. She had neoadjuvant chemotherapy based on six cycles of Vincristine, Ifosfamide, Doxorubicin, and Etoposide (VIDE). She had a tumor resection with reconstruction by cement. The anatomic pathology examination of the operative part concluded that there was no viable tumor outbreak with clear margins. The patient underwent adjuvant chemotherapy made of eight cycles of Vincristine, Adriamycin, and Cyclophosphamide (VAC).
The patient did not show up for 6 years.
Six years later, she consulted our institution for relapse in her left arm. The full workup based on CT scan showed a lytic tumor process of the first rib that invades the upper mediation, ensheathed the brachio-cephalic arterial trunk, and compresses the upper vena cava. We discovered on the CT scan a voluminous retro-gastric tumor process of 12 × 8 cm compressing the stomach, the tail of the pancreas, and the splenic vessels. The patient had no abdominal symptoms. Esophagogastroduodenoscopy was normal. A core biopsy was performed for both chest and abdominal lesions. The anatomic pathology examination concluded a relapse of her ES for both the sites (Figure 1). The fusion gene such as EWS-FLI-1, EWS-ERG, EWS-ETV1, and EWS-FEV was not performed in our institution due to the lack of materials. The diagnosis of ES was based on histopathology and immunohistochemistry. The multidisciplinary committee (MDC) recommended starting with chemotherapy. She received six cycles of Etoposide, Ifosfamide, and Cisplatin (VIP). Abdominal magnetic resonance imaging (MRI) was performed following chemotherapy treatment. MRI showed a retro-gastric mass that measured 4.41 × 1.51 cm in its greatest axis. This mass was in a hyposignal T1 and T2 with non-gadolinium-enhancing (Figures 2 and 3). These findings invoked a fibrous lesion. However, the local recurrence did not show any clinical response. The MDC decided to operate on the patient because of the persistence of the mass and the single character of the metastasis.
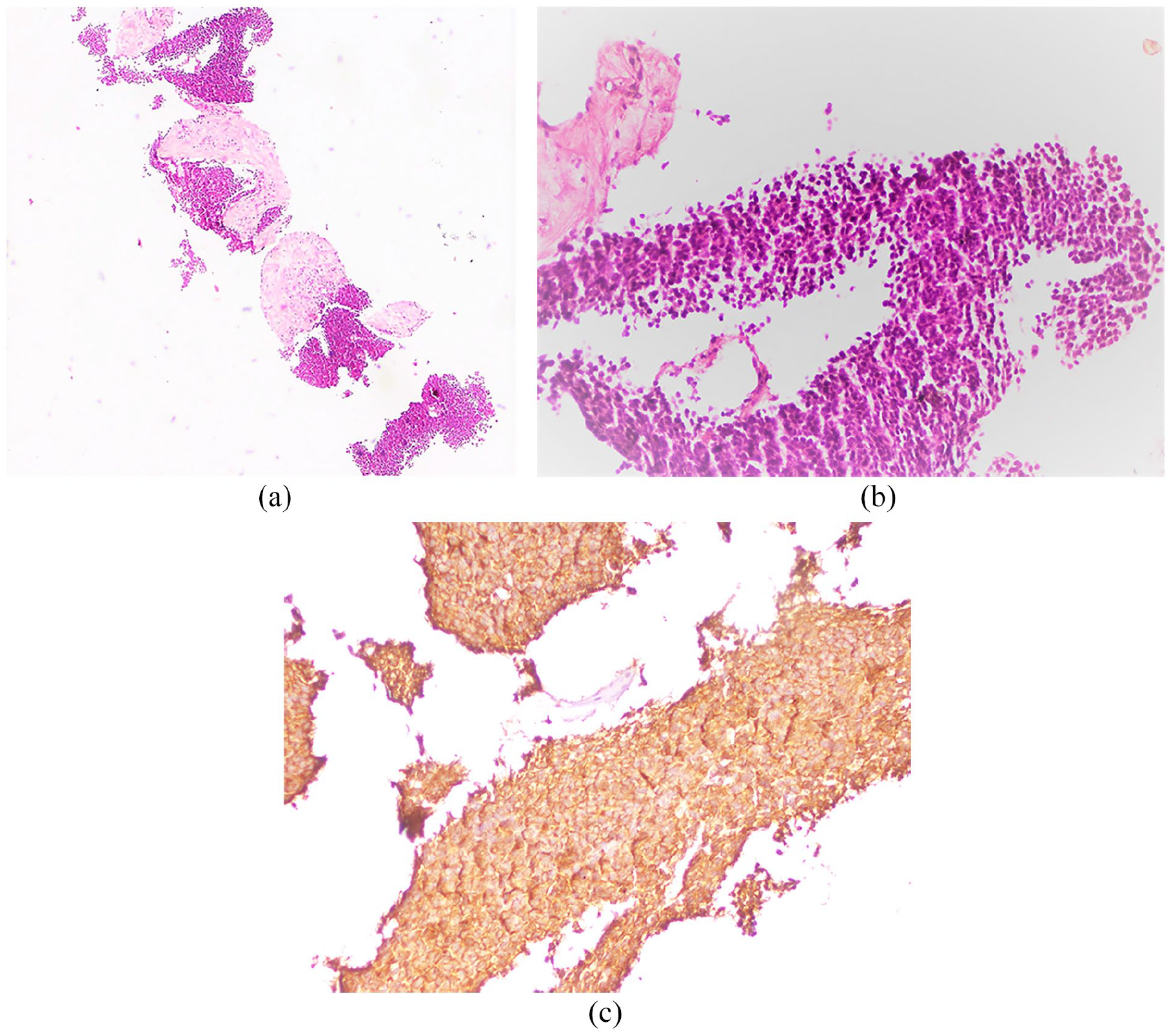
(a) Magnification in hematoxylin–eosin staining × 10: retro-gastric mass biopsy: tumor proliferation with small round cells arranged in diffuse layers, separated by thick fibrous spans; (b) magnification in hematoxylin–eosin staining × 40: small tumor cells with a high cytoplasmic ratio, the nuclei are hyperchromatic with some mitosis patterns, the cytoplasm is sparsely abundant; (c) CD 99 positivity in tumor cells (magnification ×40).

MRI T1 sequence, axial cut: (a) retro gastric mass in contact with the tail of the pancreas in distinctly hyposignal T1 and measuring 4.41 × 1.51 cm in its greatest diameter; (b) MRI T1 Fat-Sat sequence, axial cut: retro-gastric mass in contact with the tail of the pancreas presents an intermediate signal; (c) MRI T1 Fat-Sat Gadolinium, axial cut: spiculated fibrous mass with a transverse thickening at the gastric post side, this mass presents a peripheral enhancing.

Axial cut: retro-gastric mass in contact with the tail of the pancreas in distinctly hyposignal T2.
The patient underwent a median exploratory laparotomy. The tumor was located in the lesser sac and abutted the splenic hilum to the left and the posterior wall of the stomach anteriorly. The tumor was closely tied to the pancreatic tissue. We performed an excision of the tumor with distal pancreatectomy and splenectomy (Figure 4). Her postoperative recovery was uneventful. The anatomic pathology examination concluded a complete therapeutic effect within the resected mass (Figure 5). All the margins were free. The surgical margin was R0 according to the R classification. The patient was subsequently referred to a cardiothoracic surgery to operate the coastal mass.
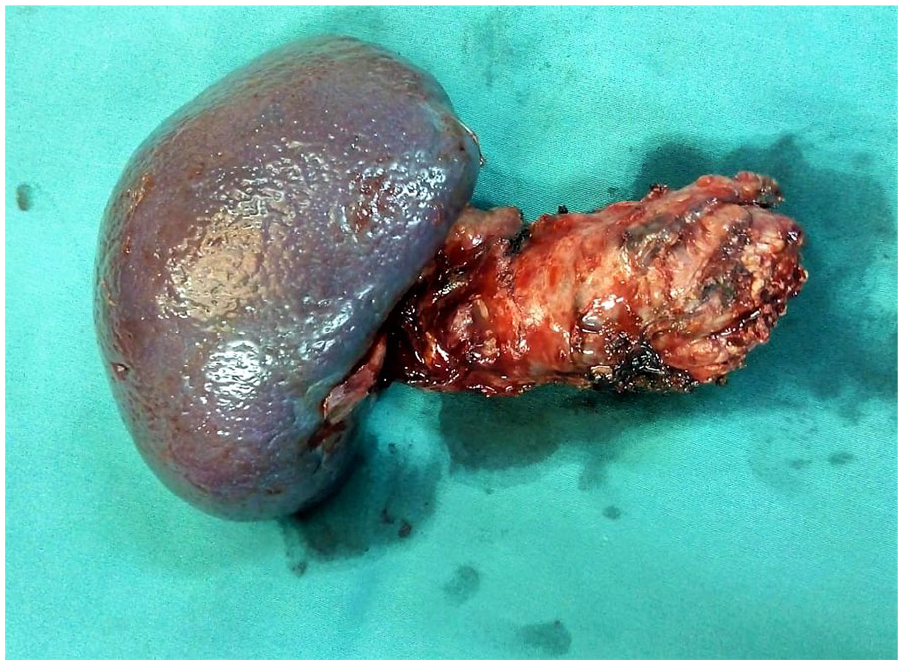
Specimen of caudal splenopancreatectomy, showing the tail of pancreas and the spleen resected in monobloc.

Magnification in hematoxylin–eosin staining × 20: (a) fibro-hemorrhagic areas of the peripancreatic parenchyma without detectable tumor residue. Magnification in hematoxylin–eosin staining × 20; (b) deposition of hemosiderin in a mononuclear inflammatory infiltrate. Magnification in hematoxylin–eosin staining × 20; (c) extensive hemorrhagic areas in the presence of ectatic vessels in a fibrous stroma. Magnification in hematoxylin–eosin staining × 20; and (d) no evidence of tumor proliferation in the pancreatic and peripancreatic parenchyma.
She underwent a wide resection of the local recurrence. The histological exam showed the features of viable ES, with necrosis. The necrosis rate was estimated greater than 50%. The margins were free. Adjuvant radiotherapy was performed at the local recurrence site at the dose of 50 Gy.
The patient is doing well after 21 months of regular follow-up.
Discussion
ES is one of the most frequent malignant bone tumors in children and young adults, responsible for 10%–15% of all primary bone tumors and 3% of pediatric malignant tumors.12,13 The fusion of the EWS gene (EWSR1) with different members of the ETS Gene family (FLI1, ERG, ETV1, ETV4, and FEV) on chromosome 22q12 is characteristic of ES.14,15
Many chromosomal rearrangements are possible, which generates distinct sarcoma entities. The biological consequence of these different genetic relations remains unclear. 16 Lungs, bone, and bone marrow are the most common sites of metastasis. 3 Other uncommon sites have been reported such as the liver, brain, and spleen. 17 In this reported case, we presented an unusual relapse site: the lesser sac. This site had not been documented previously as a metastatic site, but it was reported by Rao et al. 18 as a primary site of ES.
The radiological features for both primary tumor and metastasis are nonspecific and do not differ from any other mesenchymal tumor. The diagnosis was completed on histopathological examination. Based on the imaging procedure used in the primary workup, the head-to-toe positron emission tomography scan (PET) and/or bone scan may be used for restaging. 19
A recent study by Palmerini et al. 20 that involved patients treated with neoadjuvant chemotherapy for localized ES and osteosarcoma found that FDG PET scan is a valuable and noninvasive method for recognizing patients that are more likely to be chemotherapy-resistant.
In the presented case, PET scan can be useful to distinguish between fibrosis and persistent mass.
The mechanisms of metastasis are complex. 21 Some research defends the molecular mechanism that elicits pro-migratory and invasive signaling cascades. 22 Others stipulate that tumor cells can live in a nonproliferating dormant state without visible clinical progression. 21 These findings are supported by clinical observations of late relapses (over 10 years). 23 More genetic research of intraabdominal metastasis is required to fully understand its different genetic mechanisms.
Refractory or recurrent ES occurs (local and/or distant) in 30%–40% of patients with often poor prognoses.24,25 The long-term survival is 22%–24% for limited localized relapse and it is even lower for patients with distant relapse. 26 Metastases that occur in uncommon sites (brain, liver, spleen) were associated with a worse prognosis. 17
The occurrence of ES metastasis in the lesser sac is unusual. In the presented case, VIP chemotherapy has proven to be effective with a complete histological response. Given the uncertainty of complete response to the chemotherapy and the lack of standardization, we opted in the presented case to operate the metastatic site first.
To date, no standard chemotherapy treatment (with or without radiotherapy) has been established in such a setting. In retrospective or Phase II studies, several combinations of agents have demonstrated interesting responses, such as topotecan plus cyclophosphamide, temozolomide plus irinotecan, gemcitabine plus docetaxel, and high-dose ifosfamide.27–30
In the reported case, contrary to the local recurrence site, we observed a complete histological response in the metastatic site (lesser sac) after chemotherapy. These findings lead to wonder about the molecular pathway of this pathology. Further studies are needed to understand the difference in behavior between the original tumor and its metastasis.
This report illustrates a rare localization of ES recurrence. Furthermore, this metastasis was resected successfully. That leads to consider surgery in patients with resectable metastasis to improve survival.
All patients with recurrent and metastatic disease should be considered for clinical trials according to the “NCCN bone cancer 2019” recommendations. 31
Conclusion
ES metastasis in the lesser sac is extremely rare. No big-scale randomized clinical trials have been done for unusual metastatic sites, given the rarity of the disease.
The treatment of such unusual metastasis remains noncodified. The therapeutic strategy has been extrapolated from the treatment of ES metastases. Surgery is to be considered in the case of isolated metastasis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written consent was obtained from the legal representative of the patients for their de-identified information to be published in this article.