
Abstract
The previous studies about association of vitamin D and neurodevelopmental status in the first 1000 days of life showed inconsistent results. This study aimed to investigate correlation between vitamin D deficiency and neurodevelopmental in 2 years old infants. A cross-sectional study was conducted in Sukabumi and Waled, West Java involving 2 years old infants born from the mothers participated in previous cohort. Total 109 infants met the criteria. Vitamin D was measured and neurodevelopmental status was assessed using ASQ-3 in each subject. Statistical analysis using Spearman’s Rank correlation and multiple regression model. 50.4% infants had vitamin D deficiency (<50 nmol/L). Neurodevelopmental status showed appropriate for age. No significant association between vitamin D level and neurodevelopmental in 2 years old infants. However, there was an association between some developmental domains and vitamin D level at birth. No correlation between vitamin D and neurodevelopmental in 2 years old infants.
Introduction
The first 1000 days of life is the cornerstone of health, growth, and optimal brain development of child. It is the period when important events occur such as increase of cell numbers (proliferation), growth and differen-tiation (complexity), myelination, and synaptogenesis (connectivity).1,2 Undetected and untreated disorders during this neurodevelopmental period will gave huge impact of the person in the future. 3 Neurodevelopmental disorders become the latest morbidity in pediatrics. Nowadays, there is an increase of the cognitive developmental disorders such as autism, hyperactivity disorders, and delay in motor skills, speech, and behavior. 4
Two main factors determining the quality of child development are genetic (intrinsic) and environmental (extrinsic). 5 Micro and macro nutrient affect the neurocognitive development in early childhood. 6 Vitamin D is one of micronutrients that improve the neurodevelopmental function especially in the first 1000 days of life. 2 Vitamin D deficiency is a recent global health problem occurring in all age groups. South East Asian Nutrition Survey (SEANUT) stated that there were 40% to 50% of 6 months to 12 years old children had vitamin D deficiency. Meanwhile, it is assumed that only 5% of Indonesian children have normal vitamin D status (≥75 nmol/L). 7
Based on in vitro and animal study, vitamin D has important role on brain development, specifically in neural pathways involving the intracellular vitamin D receptor (VDR) and its function to cytokines production, synaptic plasticity, and neurotransmission. 8 Vitamin D also plays role in differentiation of neuron, decreases of apoptosis in hippocampus (related to memory and language), neuroprotective and anti inflammation on the brain.9,10
There were inconsistent results of the previous studies regarding the association between neurodevelopmental disorders and vitamin D deficiency in the first 1000 days of life or infant period. A cohort in Indonesia studied about relationship between maternal vitamin D deficiency in early pregnancy and neurodevelopmental status in a year-old infants (3, 6, and 12 months old) showed that there was no significant difference of Ages and Stages.
Questionnaire-3 (ASQ-3) scores in all neurodevelopmental aspects for 6 and 12 months old infants, expect fine motor skills in 3 months old infants. 11 This study aimed to investigate the correlation between vitamin D deficiency and neurodevelopmental status in 2 years old infants who were participated in previous cohort.
Methods
Study Design and Subjects
This was a cross-sectional study involving infants whose mothers participated in longitudinal cohort named “Association of maternal vitamin D deficiency and infant’s neurodevelopmental status: A cohort study on vitamin D and its impact during pregnancy and childhood in Indonesia” in 2016 to 2019 period. Study population were infants form that cohort aged 2 years old in Sukabumi and Waled, West Java, Indonesia. The sample was selected by total sampling from the previous cohort.
Inclusion criteria was 2 years old infants when this study was conducted. Exclusion criteria were those who acquired chronic disease such as malignancy, tuberculosis, and congenital heart disease; had history of high risk condition of developmental disorders such as Kern icterus, convulsion, and asphyxia. From the 141 infants in the cohort, 109 infants met criteria to participate in this study, while the 32 others were loss to follow up. All the mothers of the infants involving in this study had given the consent to participate in this study.
Methods
1. Neurodevelopmental assessment
Child developmental assessment was conducted by trained study team using the Ages and Stages Questionnaire-3 (ASQ-3) that already translated into Bahasa Indonesia and had been validated. ASQ-3 had 100% sensitivity, 76% specificity, and 100% negative predictive value for detecting neurodevelopmental abnormality. 12
This tool assessed 5 developmental domains; gross motor, fine motor, communication, personal-social, and problem-solving. It consisted of total 30 questions with 6 questions in each domain. The answers for each question were scored as follows: 10 for “yes,” 5 for “sometimes,” and 0 for “No.” Then, total score of each domain was calculated. Each domain had its own cut off score: 25.17 in communication, 38.07 in gross motor, 35.16 in fine motor, 29.78 in problem-solving, and 31.54 in personal-social. The interpretation of scores were classified as normal or abnormal (suspected delay). 13
2. Vitamin D level measurement
Vitamin D level was measured by ORGENTEC 25(OH)D3/D2 ELISA (ORGENTEC Diagnostika GmbH, Mainz, Germany; Product Number, ORG 570). We classified the vitamin D status based on The Endocrine Society Clinical Practice on vitamin D. 14 Blood samples were collected from 109 subjects in local hospitals, then we isolated the serum by centrifugation and transported to Hasan Sadikin Hospital, Bandung, West Java to measure the vitamin D level. All serums were restored at −800°C freezer.
Study Variables and Statistical Analysis
Variables in this study are vitamin D level and neurodevelopmental status. Covariates of this study were maternal education level, maternal occupation, birth weight, parenting styles, nutrient adequacy level, maternal vitamin D status, and vitamin D status at birth. The correlation between vitamin D level and neurodevelopmental status was analyzed using Spearman’s Rank correlations (5% risk of type I error and 20% of type II error rate). The coefficient (r) .3 or higher was considered as cut off point, hints at a weak positive correlation. The covariates (P value <.25) were analyzed by using multiple regression model. Statistical analysis was conducted using SPSS version 20.0.
Results
Demographics
A total of 109 aged 2 years old participated in this study. Characteristics of subjects were anthropometric status (weight/height and height/age), nutrient adequacy level, birth weight, gestational age, maternal age, maternal education level, maternal occupation, parity, maternal vitamin D level, vitamin D level at birth, and parenting styles. Mean value of subjects’ age was 25.9 months old; the oldest was 29 months old, and the youngest was 23 months old. The ratio of girls:boys was 55%:40%. The retailed demographics data was described in Table 1.
General Characteristics of the Infants (n = 109).

Vitamin D Level and Neurodevelopmental Status
The overall median and mean of 25(OH) vitamin D level was 47.2 and 50.7 nmol/L. Most infants were classified as vitamin D deficiency (50.4%). Only 14 infants had normal vitamin D level (12.8%). The results of child developmental assessment using ASQ-3 showed that most of the developmental domains were appropriate for the age except fine motor domain (see Table 1).
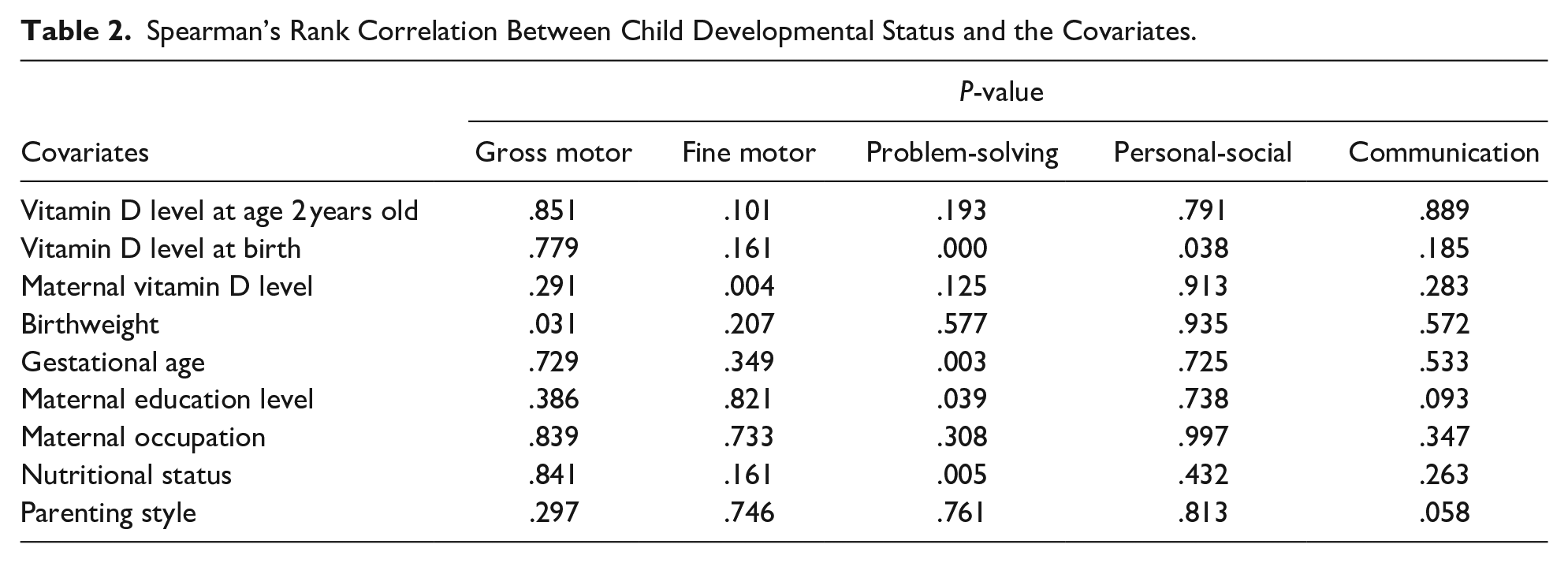
There was no significant correlation between vitamin D level and developmental status for 2 years old infants (P value >.05). However, there was a significant association between the covariates: vitamin D level at birth with problem-solving and personal-social; maternal vitamin D with fine motor; birth weight with gross motor; gestational age, maternal education level, and nutrient adequacy level with problem-solving (see Table 2).
Spearman’s Rank Correlation Between Child Developmental Status and the Covariates.
Multiple linear regression model was used to analyze the correlation of bivariable factors (P value <.25) such as birth weight, nutrient adequacy level, gestational age, maternal education level, maternal vitamin D level, and vitamin D level at birth (see Table 3). There was a significant association between: gross motor with birth weight; personal-social and communication with vitamin D level at birth. A negative correlation were found between fine motor with vitamin D level at age 2 years old and maternal vitamin D status, whereas it showed a positive correlation between fine motor with nutritional status. Problem solving with vitamin D level at birth and nutrient adequacy level were significantly associated in contrast to maternal education level.
Factors Affecting Child Developmental Status (ASQ-3) on Multiple Regression Model.

Discussion
Calcifediol known as 25(OH) vitamin D is the main metabolite form of vitamin D found in the circulation, so it considered as the best indicator of vitamin D status. 15 There are definite practical guidelines to define the vitamin D status based on The US Endocrine Society Clinical Practice Guidelines which defined vitamin D deficiency as a 25(OH)D <50 nmol/L (<20 ng/mL), insufficiency as 52.5 to 72.5 nmol/L (21 to 29 ng/mL), and sufficient as >72.5 nmol/L. 2 SEANUT defined vitamin D status deficiency as below 25 nmol/L and insufficiency as below 50 nmol/L. 7
A study in India stated that million people in all age groups and gender have vitamin D deficiency in spite of sun exposure. 16 Similar with SEANUT study, the vitamin D status of the subjects in this study showed only 12.8% had vitamin D sufficiency, 50.5%, had vitamin D deficiency, and 36.7% had vitamin D insufficiency. Mean vitamin D level in girls (47.2 nmol/L) were lower than in boys. This condition also found in SEANUT study that stated girls’ vitamin D level was lower than boys. 8 On the contrary, the study in England showed vitamin D deficiency occurred in boys under age 5 more than in girls. 17
Regarding the vitamin D level and neurodevelopmental status in children, a cross-sectional study conducted in Mesir reported school-aged children whose vitamin D level were 37.5 to 77.5 nmol/L had better neurodevelopmental status than children with below level 27.5 nmol/L. 18 Another study also stated children at age 16 to 18 months whose severe vitamin D deficiency were at much greater risk of mental illnesses and psychomotor development. 19 This study showed there was no significant association between vitamin D level and neurodevelopmental status in infants at age 2 years old. This results also supported by previous study in India that also showed no correlation of vitamin D deficiency in children at age 12 to 36 months and its cognitive developmental status. 20 In addition, case control study in USA also stated that there was no association between vitamin D deficiency and neurodevelopmental status.21,22
Our study found the correlation between some neurodevelopmental domains: problem-solving, personal-social, and communication and vitamin D status at birth by using multiple linear regression model. These results were supported by 2 previous studies in America and Australia that showed a positive correlation between vitamin D level in umbilical cord blood and neurocognitive development at age 7 and language skill at age 18 months and 4 years old.21,23
Vitamin D known has important roles of neurogenesis in neural pathways.5,24 There is a link between vitamin D deficiency and neurodevelopmental status by discovering vitamin D receptor (VDR) on animal testing research. That explained there was a certain roles of VDR, found in neuroepithelium, during neurogenesis and as neuroprotection for neural stem cells in subventricular zone. Recent study found there was expression genes of VDR in specific brain areas: temporal lobe, cingulata, thalamus, cerebellum, amygdala, and hippocampus (related to memory and language).9,10,25
The effects of vitamin D on the nervous system can be explained by some mechanisms. First mechanism is prevention of oxidative stress; vitamin D is an antioxidant which controls the process of detoxification in the brain by regulating the activity of glutamyl-transpeptidase to stimulate the synthesis of glutathione. Glutathione is antioxidant protecting oligodendrocytes and neural pathway’s integrity. A study proved pre-treatment with vitamin D can decrease signal glutamate-mediated cell death in cortical, hippocampus, and mesenphalic neurons. Second mechanism is regulation of neurotrophic factors. Vitamin D regulated expression of neuron growth factor (NGF), neurotrphin-3 (NT-3), neurotrophin-4 (NT-4) and glial cell derived neurotrophic factors (GDNF) play roles in neuron differentiation and maturation. NGF acts on growth, protection, and regulating normal fuction septohippocampal pathways in which is significant to learning and memory. Third mechanism is calcium balance by regulating the expression of calcium binding proteins and L-type voltage sensitive calcium channels which have important roles in intracellular calcium binding. Last mechanism is a neuroprotector which has roles in inflammation process. Vitamin D protects the brain from inflammation-induced neurodegenerative by inhibiting TNF-α, IL-6, and NO, preventing lipid peroxidation, and apoptosis. Therefore, vitamin D status during neurodevelopmental period will impact on future’s child development.26-29
The most critical and rapid human brain development period are at the end of third trimester of pregnancy and the first 1000 days of life. 3 Neurogenesis in hippocampus indicates higher cortical functions (prefrontal cortex area) developing rapidly at the peak time of 1 to 5 years old. 30 Vitamin D involves in neuronal migration and stimulation of the neurotransmitter synthesis. 24 Despite there was a time difference to observe the best time to find the effect of vitamin D towards child developmental status, it will cause a difference results between serum vitamin D level at birth and at age of 2 years old related to child developmental status. It was solely because of myelination and synaptogenesis, proving brain especially in prefrontal cortex area continues to grow and develop through late adolescence, and vitamin D took a part of the process. 31
There was no relation between Vitamin D deficiency status in the first 1000 days of life and neurodevelopmental status during childhood period. On the other hand, poor neurodevelopmental status in the first 1000 days of life was proven to be connected until school-aged period. A cohort study conducted to 1000 North Indian children at 6 to 9 years of age showed poor vitamin D status was not associated with any of impaired cognitive outcomes and linear growth. 32
Our results showed the majority neurodevelopmental domains in 2 years old infants were appropriate for the age, except for fine motor score which showed negative correlation with vitamin D level. Small size of study samples, vitamin D level and child developmental measurement errors could become the limitation of our findings.
Our findings showed the majority of maternal occupation were housewives with low education background. Therefore, vitamin D supplementation as standard therapy may be not easy to be implemented due to the expensive price. According to the study in Indonesia, sun exposure on 18,59% of body surface area for 37,5 minutes per day, with the best time of sun exposure UVB was between 10.00 am to 1.00 pm, was an alternative method to fulfil the daily vitamin D needs. 33
Limitation to this study was the lack of information about factors affecting vitamin D level such as the duration and clothes wearing during the day time of sun exposure. Moreover, there was a different laboratory test methods which might stated different interpretation of vitamin D status. Besides, we collected nutritional status based on 24-hours dietary recall, we could not calculate vitamin D contained food. The advantage of this study was the sample & data could be collected from well conducted study (previous cohort). Our findings also included the parenting aspect providing children’s physical activity data and 24-hours dietary recall in order to measure vitamin D nutrient consumption.
Conclusion
There is no significant association between vitamin D status in 2 years old infant and neurodevelopmental status (P value >0.05). Meanwhile, there is an association between some child developmental domains such as problem-solving, social personal, and communication with vitamin D status at birth.
Further research is needed to analyze the comprehensive neurodevelopmental assessments such as BINS or intelligence quotient (IQ) test based on appropriate age, expecting different results. The bigger sample size is considered to be collected in order to find a significant association between factors impacting vitamin D status: sun exposure and rich vitamin D food with. In addition, further randomized clinical trial is needed to get a consideration in order to evaluate the efficacy of vitamin D toward neurodevelopmental status and to find the optimal dose and duration of time administration vitamin D.
Footnotes
Acknowledgements
We express our gratitude to Abdurachman Sukadi, Sri Endah Rahayuningsih, and Rd. Reni Ghrahani for all their input and correction so that this research can be conducted, to field researches of Midwives Academic Study, Bunga Mars for their faithful efforts in this study, and also to Hadyana Sukandar for statistical analysis support. Many thanks to all the staff at the Waled and Sukabumi Health Office and Primary Health Centers for their contribution so this study can be performed in these cities.
Author Contributions
Dhamayanti M, contributed to conception and designinterpretation of data, critically revised manuscript, gave final approval.
Risan NA, contributed to acquisition, critically revised the manuscript, gave final approval.
Djuwita F, contributed to acquisition, drafted manuscript, gave final approval.
Gumilang L, contributed to acquisition, gave final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant-in-aid from Universitas Padjadjaran.