
Abstract
Objective
There are currently no studies on the role of vitamin D receptor (VDR) levels as a cause of or risk factor for sepsis. We aimed to establish the association between VDR levels and 28-day mortality in critically ill patients with sepsis.
Methods
This prospective cross-sectional observational study included 148 patients diagnosed with sepsis who were treated in the intensive care unit. We measured VDR levels, laboratory characteristics, and health scores and related them to survival.
Results
The 148 patients included 96 survivors and 52 non-survivors, with VDR levels of 1.92 and 1.36 ng/mL, respectively. Baseline VDR was a significant predictor of 28-day mortality, with an area under the curve of 0.778. A low VDR level was significantly associated with lower overall survival in patients with sepsis according to Kaplan–Meier curve analysis. VDR levels were also negatively correlated with lactate, C-reactive protein, acute physiological and clinical health evaluation (APACHE) II and sequential organ failure assessment (SOFA) scores, and disease severity.
Conclusions
VDR levels were associated with high 28-day mortality and negatively correlated with lactate, C-reactive protein, APACHE II and SOFA scores, and disease severity in patients with sepsis. VDR levels can predict poor outcomes in patients with sepsis.
Introduction
Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. 1 Sepsis can lead to septic shock, multi-organ dysfunction syndrome, multi-organ failure, and even death. Extensive research is being conducted to understand the pathophysiology, risk factors, treatment, and management strategies of sepsis to prevent its serious sequelae. The main strategies for the prevention and treatment of sepsis and its complications include glycemic control, use of broad-spectrum antibiotics, control of the source of infection, use of ventilatory support, and use of corticosteroids and vasopressor support. 2
Vitamin D plays a vital role in the human body and vitamin D receptors (VDRs) have been discovered in most types of immune cells, including activated CD4 and CD8 T cells, B cells, neutrophils, macrophages, and dendritic cells. 3 Previous studies found that 1,25-vitamin D targeted the tumor necrosis factor pathway to suppress inflammatory bowel disease in an experimental model, and increased the vasoconstrictor response to noradrenaline and angiotensin 2. 4 , 5 Vitamin D levels are associated with the risk of sepsis. Jeng et al. 6 showed that vitamin D insufficiency was present in 100% of critically ill patients with sepsis, 92% of critically ill patients without sepsis, and 66.5% of healthy controls. Recent evidence has also shown that vitamin D can enhance the function of the innate immune system by stimulating the formation of the cathelicidin antimicrobial peptide, indicating critical roles in the prevention of intestinal perforation and in the body’s fight and flight response against infection, and ultimately sepsis and septic shock. 7
The association between vitamin D levels and immunity has been discussed and validated in several studies,7–9 and some studies have examined the role of VDRs in multiple sclerosis, autoimmune disease, and B cell-dependent allergic immune responses.10–12 However, the role of VDR levels in immunity, sepsis, septic shock, and sepsis-related mortality remains unclear. We therefore aimed to establish the association between VDR levels and 28-day mortality in patients with sepsis.
Materials and Methods
Patients
This prospective cohort study enrolled patients of either sex, aged >18 years, who were diagnosed with sepsis and treated in the intensive care unit (ICU) at Adana City Training and Research Hospital from October 2019 to January 2020. Sepsis was diagnosed according to Sepsis-3 criteria. 13
Our main aim was to study patients with sepsis. Mortality rates are high in patients with septic shock, which may affect the statistical results, and we therefore excluded patients with septic shock from this study. In addition, antibiotics are one of the main treatments for sepsis but may also affect the inflammatory response in septic patients, and we therefore excluded patients who had used antibiotics in the previous 2 weeks. VDR levels have been shown to vary in patients with cancer,14,15 and inflammatory markers may be elevated in patients with cancer independent of infection, and we therefore also excluded patients with cancer from the study. We also excluded pregnant women. The patients were separated into two groups: survivors (group A), who were discharged or transferred within 28 days of the first diagnosis (patients were followed for 28 days if they were discharged or transferred from the ICU), and non-survivors (group B), who died within 28 days of the first diagnosis. A flow diagram for this study is presented in Figure 1. The Sequential Organ Failure Assessment (SOFA) score, Acute Physiological and Clinical Health Evaluation II (APACHE II) score, and Charlson Comorbidity Index (CCI) were calculated for each patient.

Flow diagram for patients.
The study was approved by the Local Ethics Committee of Adana City Training and Research Hospital (decision no. 528; August 28, 2019). Written informed consent was obtained from all patients or their legal guardians.
Laboratory tests
Complete blood counts and biochemical parameters of the patients were measured. Complete blood counts were analyzed using a Sysmex XN-10 Automated Hematology Analyzer (XN series, Sysmex Corporation, Kobe, Japan) according to the manufacturer’s instructions. Serum procalcitonin levels were measured with a Unicel-DXI (Beckman Coulter Inc., Brea, CA, USA) using a commercial chemiluminescence immunoassay test kit (Access PCT; Beckman Coulter Inc.). 25-OH vitamin D and parathormone levels were measured using a Beckman Coulter Unicell DXI 800 immunoassay analyzer (Beckman Coulter Inc.) with commercial chemiluminescence immunoassay kits supplied or validated by the manufacturer. Other biochemical parameters were measured using a Beucher Coulter AU 5800 (Beckman Coulter GmbH, Krefeld, Germany) with commercial test kits produced or validated by the manufacturer.
Serum creatinine, lactate, phosphorus, calcium, and albumin levels were analyzed using standardized laboratory procedures. Serum procalcitonin levels were measured using an immunoluminometric assay, and C-reactive protein levels were measured using nephelometry. Serum parathyroid hormone levels were measured by immunoradiometric assays, and 25-OH vitamin D levels were measured by chemiluminescent immunoassay.
VDR measurement
A 5-mL venous blood sample was taken from each patient after diagnosis and before treatment. The blood samples were centrifuged at 1790 × g for 10 minutes, and the resulting serum samples were frozen and stored at −80°C until testing. VDR levels were determined using a commercial enzyme-linked immunosorbent assay kit (MyBioSource, Inc., San Diego, CA, USA), according to the manufacturer’s instructions.
Statistical analysis
Statistical analyses were performed using R version 3.4.2 (R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism 8.0 (GraphPad Inc., San Diego, CA, USA). Continuous variables are presented as means (standard error) and categorical variables as numbers with percentages. The data were analyzed using χ2, Fisher’s exact, Mann–Whitney, and Student’s t-tests, as appropriate. Correlation coefficients of numerical variables that did not conform to at least one normal distribution measurement were calculated using Pearson’s test and statistical significance was determined using Spearman’s test. Prognostic factors for 28-day mortality in patients with sepsis were identified using Cox proportional hazards regression analysis with Wald’s test. All variables that were statistically significant for mortality were included in the univariate analysis and all variables with a P value <0.2 in the univariate analysis were included in the multivariate analysis. The predictive role of VDR levels for 28-day mortality was evaluated by receiver operating characteristic (ROC) curve analysis. The optimal threshold value for VDR was derived from the Youden index. The association between VDR level and survival rate was assessed by Kaplan–Meier curve analysis. A two-sided value of P < 0.05 was considered statistically significant.
Results
Patient characteristics
A total of 148 patients were enrolled in the study, including 96 patients in group A (survivors) and 52 patients in group B (non-survivors). The patient characteristics are shown in Table 1.
Patient characteristics.

Values given as mean ± standard deviation, median (interquartile range), or n (%).
APACHE II: Acute Physiological and Clinical Health Evaluation II; SOFA: Sequential Organ Failure Assessment; CCI: Charlson Comorbidity Index; SD: standard deviation.
Laboratory tests
The results of laboratory tests are shown in Table 2. The mean CRP level was significantly lower in group A (P = 0.005), and the mean 25-hydroxyvitamin D and VDR levels were both significantly higher in group A (P = 0.014 and P = 0.001, respectively), compared with group B.
Results of laboratory tests.
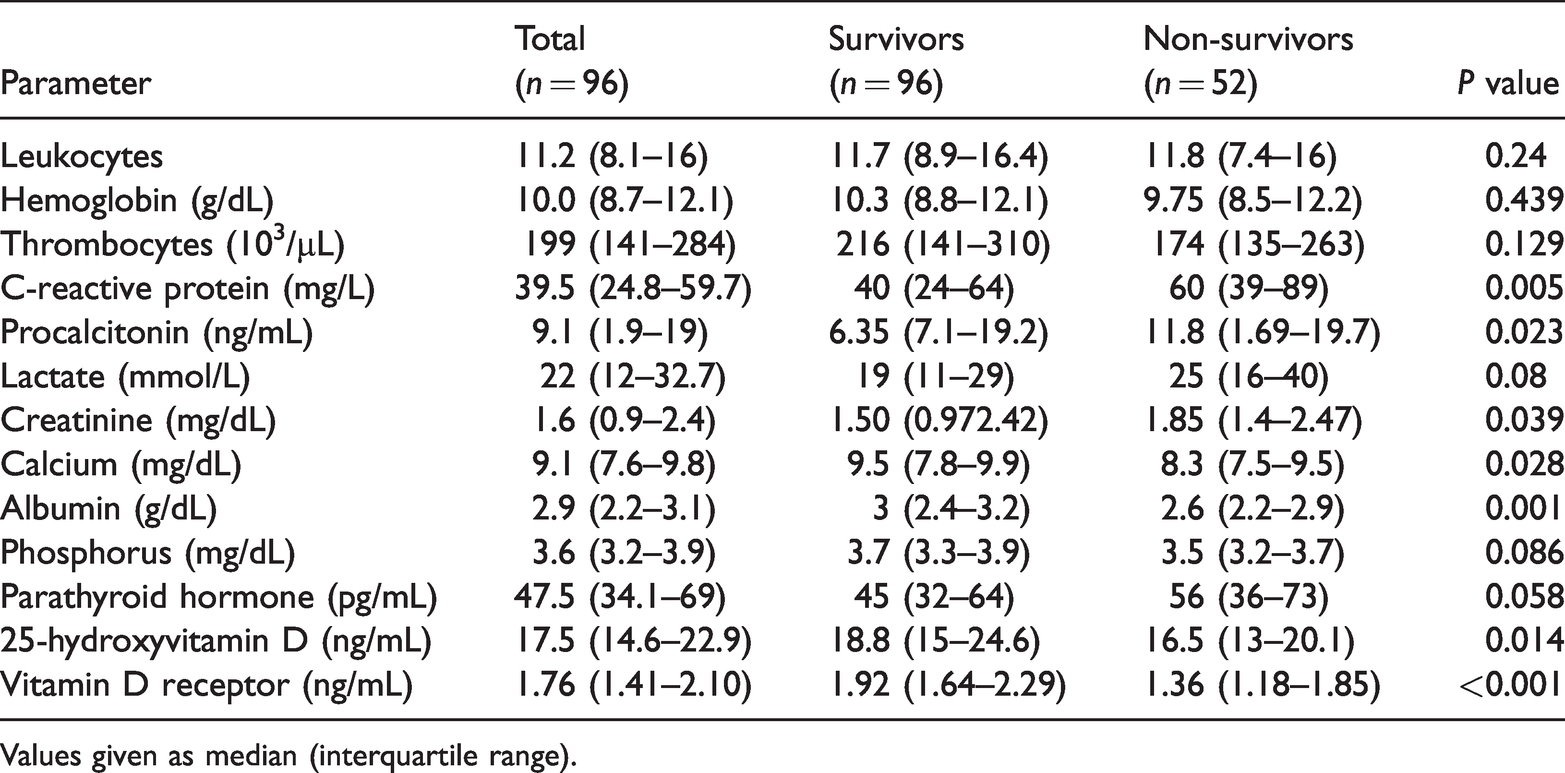
Values given as median (interquartile range).
Spearman’s analysis of the correlations between VDR level, sepsis severity, and inflammation biomarkers showed that VDR levels were negatively correlated with APACHE-II (P < 0.05), SOFA (P < 0.001), and CRP (P < 0.05) (Table 3).
Correlations of serum vitamin D receptor levels with clinical parameters and blood markers.

APACHE II: Acute Physiological and Clinical Health Evaluation II; SOFA: Sequential Organ Failure Assessment.
Prognostic factors for 28-day mortality
We investigated the potential prognostic factors for 28-day mortality in patients with sepsis by univariate and multivariate Cox proportional hazards regression analyses using 13 potential risk factors routinely assessed during hospitalization in the intensive care unit (Tables 1 and 2). Univariate Cox analysis identified the presence of septic shock, invasive mechanical ventilation, renal replacement therapy, SOFA and APACHE II scores, creatinine, albumin, and VDR levels as potential prognostic factors in patients with sepsis (Table 4). All variables with a P value <0.2 in univariate analysis were included in the multivariate analysis, which confirmed the presence of septic shock (P < 0.05), APACHE II score (P < 0.05), and low VDR levels (P < 0.05) as independent prognostic factors associated with 28-day mortality in patients with sepsis.
Univariate and multivariate Cox proportional hazards regression models to identify variables independently associated with 28-day mortality.

APACHE II: Acute Physiological and Clinical Health Evaluation II; SOFA: Sequential Organ Failure Assessment; HR, hazard ratio; CI, confidence interval.
VDR levels and prognosis
Baseline VDR level was a significant predictor of 28-day mortality, with an area under the curve (AUC) of 0.778 (95% confidence interval: 0.695–0.861), a cut-off value of ≤1.7, a sensitivity of 73.1%, and a specificity of 72.9% (Figure 2). Patient were categorized into high (>1.7) and low VDR (≤1.7) groups, according to the cut-off value. A low VDR level was significantly associated with lower overall survival in patients with sepsis according to Kaplan–Meier curve analysis with log-rank test (P < 0.05) (Figure 3).

Predictive value of vitamin D receptor for 28-day mortality in septic patients determined by receiver operating characteristic (ROC) curve analysis.

Overall survival rate and vitamin D receptor levels by Kaplan–Meier curve analysis. Low vitamin D receptor level (≤1.7) was significantly associated with a lower overall survival rate in septic patients, determined by log-rank test.
Discussion
This study showed that a low baseline level of VDR was associated with a high incidence of 28-day mortality among patients with sepsis in an ICU setting.
Numerous studies worldwide16,17 have examined the causes of morbidity and mortality in patients with sepsis, and have identified septic shock, high APACHEII score, invasive mechanical ventilation, high SOFA score, and low 25-hydroxyvitamin D levels as the main associated factors. However, the current research is the first comprehensive study to investigate the role of VDR levels in 28-day mortality in critically ill patients.
Tayel et al. 3 showed that vitamin D deficiency and variations in VDR levels in neonates/mothers were associated with neonatal sepsis, providing evidence of a role for VDR in the development of sepsis, independent of other risk factors. These results were comparable to those of the current study; however, their study was conducted in neonates, suggesting that although the study patients can change the outcome, the pathophysiology involving low VDR levels remains the same.
Another study conducted by Olejarova et al. 18 showed that low levels of vitamin D in patients with sepsis who did not survive to day 7 (p = 0.0076) and day 28 (p = 0.0338) of hospital care. They also found a negative correlation between levels of vitamin D and the inflammatory markers CRP (P = 0.0003), presepsin (P = 0.0032), and sTREM-1 (triggering receptor expressed on myelocytes; P = 0.0065), and clinical condition (SOFA score; P = 0.0385) in all patients with systemic inflammatory response syndrome/sepsis. These results were in accord with the results of the current study. Although we primarily considered low levels of VDR, we also found negative correlations between VDR levels and APACHEII score (P<0.05), SOFA score (P<0.001), and CRP levels (P<0.05). Overall, these studies suggest that sepsis might result in a reduction in VDR levels, and that VDR levels are associated with poor outcome.
Although many studies have examined vitamin D levels in patients with sepsis, the present study considered both vitamin D and VDR levels at the same time, which represents a strength of our study. However, the relationship between vitamin D and VDR levels remains controversial. Han et al. 19 found that low vitamin D levels were associated with decreased VDR expression in peripheral blood mononuclear cells in patients with sickle cell anemia. Lee et al. 20 found that VDR gene expression increased after vitamin D supplementation in white adipose tissue in obese rats, while Mazdeh et al. 21 found no significant correlation between vitamin D and VDR gene expression levels in the peripheral blood in epileptic subjects, and Tomaszewska et al. 22 found no changes in VDR gene expression in the sinonasal epithelium after oral vitamin D supplementation.
An important aspect of this study was that we only included patients with sepsis, and excluded patients with septic shock. In contrast, most previous studies included patients with septic shock, which is an independent risk factor for 28-day mortality in patients with sepsis.
Albumin is a negative acute-phase protein that may reflect the degree of inflammation, and the level of hypoalbuminemia may reflect the severity of the inflammatory reaction in critically ill patients. The current study found significantly lower albumin levels among non-survivors, in accord with the literature. 23 However, multivariate Cox regression analysis did not identify hypoalbuminemia as an independent risk factor. Nutritional status and chronic inflammatory disorders also affect albumin levels, albumin levels are therefore low in critically ill patients, and albumin-based predictions could have limitations.24,25 Elevated lactate levels are also associated with poor clinical outcomes and high patient mortality, 26 and the current study accordingly found significantly higher lactate levels among non-survivors. Lactate can be used for the early diagnosis, management, and risk stratification of patients with sepsis. 27 We also compared VDR levels with other biomarkers, and showed that VDR levels were negatively correlated with the inflammatory marker, CRP, and with the impaired tissue oxygenation marker, lactate. Low levels of VDR were an independent factor associated with a poor outcome.
Calcium plays an important role in many physiological processes, and hypocalcemia is common and is associated with increased mortality in critical care patients. However, the etiology of hypocalcemia in critical care patients is unclear and potentially multifactorial. Vitamin D deficiency is a common cause of hypocalcemia. 28 The current study found a significant decrease in calcium levels in non-survivors. The significantly lower levels of vitamin D and calcium among non-survivors compared with survivors supports the previous literature.
Predictive scoring systems are used to predict mortality in ICU patients. The APACHE II and SOFA scoring systems have been widely validated and used by many ICUs to classify sepsis severity and predict hospital mortality.29,30 In our study, the APACHE II and SOFA scores differed significantly between survivors and non-survivors, comparable to the literature. In addition, VDR levels were negatively correlated with both APACHE II and SOFA scores.
This study had some limitations. First, it was conducted at a tertiary healthcare center, resulting in a degree of patient homogeneity. Furthermore, it was a single-center study with a limited sample size, and VDR levels were determined after diagnosing sepsis, which could affect the results. The calculated P values presented in this study do not support any powerful statistical conclusions and should be interpreted with caution. We excluded patients with cancer, patients who were pregnant, patients who had used antibiotics in the 2 weeks before presentation at the hospital, and patients who required vasopressors at the time of admission (indicating septic shock). Although we had reasons for excluding these patient groups, the lack of these patients still represents a limitation of our study. In addition, VDR is a novel biomarker, and it may not be possible to control for all variables affecting VDR levels.
Conclusions
Low VDR levels were associated with high 28-day mortality in patients with sepsis. Furthermore, VDR levels were negatively correlated with lactate, CRP, APACHE II and SOFA scores, and disease severity. VDR levels can act as an early warning in septic patients. We recommend that the rate of change in VDR levels after sepsis treatment should be examined. Further studies are also needed to investigate the specific role of VDR in sepsis and sepsis-related mortality.