
Abstract
Multiple epidemiological studies have shown that vitamin D deficiency is highly prevalent amongst adolescents in the USA. However, recommendations regarding the treatment of vitamin D deficiency in healthy adolescents are not well defined. We carried out a prospective pilot study, to determine whether treatment with 2000 international units of vitamin D3 daily for 3 months, would normalize the vitamin D levels in vitamin D deficient adolescents. Following treatment there was a 56.02% increase in the vitamin D levels from the mean baseline values and 80.39% of the subjects normalized their vitamin D levels. There were no adverse effects associated with this intervention. This study offers complementary guidelines to the existing recommendations from the American Academy of Pediatrics on the optimal dose and duration of vitamin D3 therapy in vitamin D deficient, but otherwise healthy adolescents. Further prospective, large scale, case control studies are indicated to validate our results.
Keywords
Introduction
The primary role of vitamin D is the mineralization of bone by regulating osteoblast activity and facilitating the absorption of calcium and phosphorus from the intestines and calcium from the kidneys via its active metabolite 1,25 dihydroxy vitamin D.1,2 Therefore vitamin D deficiency results in rickets in growing children and adolescents and osteomalacia in adults. 3 Additionally, recent epidemiological studies have linked vitamin D deficiency to cardiovascular disease,4,5 dyslipidemias,6-8 diabetes mellitus,9,10 cancers,5,11,12 and auto immune diseases,3,13,14 although causality has not yet been established. Thus, vitamin D deficiency effects not only musculoskeletal health, but potentially a wide range of acute and chronic medical conditions. It is therefore important to recognize and treat vitamin D deficiency promptly and effectively.
The American Academy of Pediatrics (AAP) and the Institute of Medicine (IOM), defines vitamin D deficiency, as a serum 25 -hydroxyvitamin D level of < 20 ng/ml.3,15 By this definition, the prevalence of vitamin D deficiency amongst healthy US adolescents varies from 21% to a high of 42%, depending on the geographical location, ethnicity, sex, sun exposure, BMI and the diet of the population studied.16-19 In a previous study we reported that 27.8% of healthy Hispanic adolescents presenting to our community clinic for routine physical examinations were vitamin D deficient. 20 Guidelines from the AAP and the IOM, regarding vitamin D supplementation for infants, children, adolescents and adults are well established.3,22 Whilst there are evidence based guidelines for treating vitamin D deficiency states such as rickets3,21,22 and those associated with chronic medical conditions such as chronic kidney disease23,24 and cystic fibrosis,25-27 there are no recommendations from the AAP or the IOM, regarding the treatment of vitamin D deficiency in otherwise healthy adolescents. We conducted a prospective pilot study to determine whether treatment with 2000 international units (IU) of vitamin D3 (Cholecalciferol) daily for 3 months, would normalize the vitamin D levels in vitamin D deficient, but otherwise healthy adolescents, who were not taking vitamin D supplements.
Design
Prospective interventional study, with each patient acting as a retrospective control.
Subjects and Methods
The study was conducted between December 1st 2017 and July 31st 2019, in a community based pediatric and adolescent medicine practice in Huntington Beach, CA. Healthy adolescents 13 to 19 years of age presenting for routine physical examinations were eligible for the study. Adolescents with acute or chronic medical problems, dietary restrictions, abnormal labs, and those taking vitamin D supplements were excluded. At time of presentation detailed history, complete physical examination and standard labs to include complete blood count (CBC), comprehensive metabolic panel (CMP), blood sugar, thyroid stimulating hormone (TSH), 25-hydroxyvitamin D level, and urinalysis were done. According to AAP parameters, those adolescents with a serum 25-hydydroxyvitamin D level below 20 ng/ml were considered to be vitamin D deficient and were empirically treated with 2000 IU of vitamin D3 (cholecalciferol) daily for 3 months and advised to return in 3 months for a follow up examination and measurement of their CMP, serum 25-hydroxyvitamin D level, and for a urinalysis. All participants were counselled about a vitamin D adequate diet, exercise and sun exposure. Written informed consent was obtained from all the adolescents and their parents, prior to recruitment for the study. Formal ethics approval was deemed not necessary by the pediatric peer review committee at Fountain Valley Regional Hospital, since the study involved treatment with vitamin D, a vitamin supplement freely available over the counter to the public.
Results
During the study period, 312 consecutive adolescents with no acute or chronic medical problems, who were not taking vitamin D supplements, presented for annual physical examinations (PE) and consented for the study. The flow chart for patients eligible for vitamin D3 treatment are in Figure 1 below.

Flow Chart of patients assigned for treatment with vitamin D3.
The baseline characteristics of the study group are in Table 1 and the laboratory data following treatment are in Table 2.
Baseline Characteristics of Study Group.
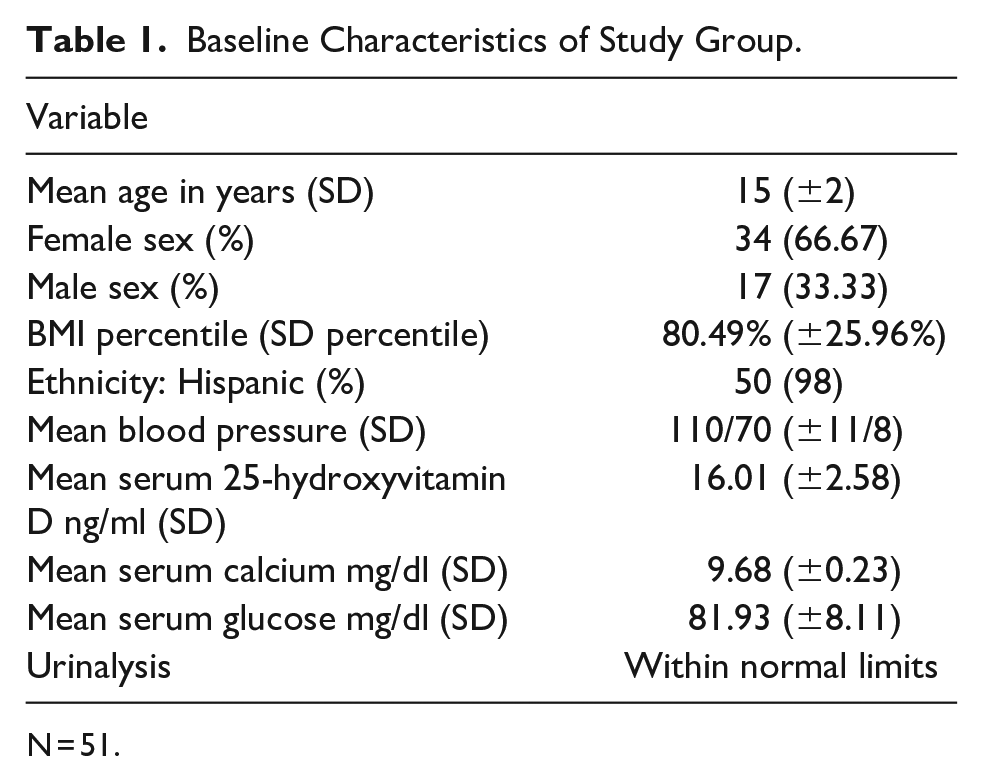
N = 51.
Laboratory Values Following Treatment.

N = 51.
There was a 56.02% increase in the mean serum 25-hydroxyvitamin D level from the mean baseline value following treatment Tables 1 and 2. 41 patients (80.39%) in the study group had normalized their serum 25-hydroxyvitamin D level to ≥ 20 ng/ml and in 10 patients (19.61%) it was yet deficient (≤19.9 ng/ml).
The follow up serum calcium, blood sugar, and urinalysis were within the normal range. There was no evidence of hypercalcemia, nephrolithiasis, or any other adverse symptoms associated with the vitamin D3 therapy.
Discussion
The dose for vitamin D supplementation in healthy adolescents is well defined by the AAP 3 and the IOM. 22 However there are no guidelines from the AAP or the IOM, regarding the optimal dose and duration of vitamin D3 therapy, in the treatment of vitamin D deficiency in otherwise healthy adolescents. Talib et al has reported that treatment with 5000 IU of vitamin D3 daily for 8 weeks corrected the vitamin D deficiency in a cohort of predominantly hispanic and black adolescents. 28 Following a placebo controlled, double blind, pilot study, Wu et al have reported that both 50,000 IU vitamin D3 monthly or 150 000 IU 3 monthly for 1 year safely and effectively corrected vitamin D deficiency in a population of adolescents from Tasmania, Australia. 29 The Indian Academy of Pediatrics recommends 60 000 IU/week of vitamin D for 6 weeks in the treatment of vitamin D deficiency in adolescents. 30
In adolescents, in order to avoid toxicity, as well as for cost and logistical reasons, it is important to treat vitamin D deficiency, with the least concentrated dose for the shortest duration that normalizes the vitamin D levels. Treatment with 2000 to 5000 IU of vitamin D3 daily has not been associated with vitamin D toxicity,31,32 whilst super high doses for prolonged periods have been reported to cause hypercalcemia and nephrolithiasis.33-35 In our population of healthy vitamin D deficient adolescents, we empirically treated the vitamin D deficient subjects with 2000 IU of vitamin D3 daily for 3 months. Following treatment with vitamin D3, there was a 56.02% increase of the mean vitamin D levels from the mean pretreatment values and the levels normalized in 80.39% of the subjects. There was no hypercalcemia, nephrolithiasis, or any adverse symptoms associated with this intervention.
The AAP does not recommend routine screening for vitamin D deficiency in healthy adolescents presenting for annual physical examinations. However epidemiological data shows that vitamin D deficiency is highly prevalent across the US, and in our community the prevalence was 27.8%. This warrants screening for vitamin D deficiency during annual physical examinations and prompt and effective treatment, in order to avoid skeletal and extra skeletal morbidities, in those who are vitamin D deficient.
We conclude that in a cohort of otherwise healthy, vitamin D deficient adolescents, who were not taking vitamin D supplements, treatment with 2000 IU of vitamin D3 daily for 3 months, increased the 25-hydroxyvitamin D level by 56.02% from the mean baseline values and normalized the vitamin D levels in 80.39% of the subjects. This was a pilot study, where the study sample was small, 98% of the subjects were of Hispanic ethnicity, there was no control population and the study were limited to the community in Huntington Beach, California. In order to test the hypotheses further, prospective, large scale case control studies, from across the USA is indicated.
Footnotes
Acknowledgements
The authors wish to thank Vicenta Cisneros and Meguen Salazar for secretarial help, and Shanti Gunawardena, MD for reviewing the manuscript.
Author Contributions
All authors contributed equally to the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.