
Abstract
Objectives
We tested the hypothesis that vitamin D supplementation is associated with early body mass index (BMI) patterns.
Methods
Using retrospective longitudinal data of infants and toddlers in a 2-year follow-up study, we identified BMI-for-age Z score (BAZ) growth trajectories using latent class growth modeling (LCGM) analysis. Logistic regression models were adopted to investigate the impact of vitamin D supplementation on BAZ patterns.
Results
Five BAZ trajectories were derived using LCGM. Higher intake of vitamin D supplement was significantly associated with lower odds of rapid weight gain or mild undernutrition in the first 2 years (odds ratios: 0.60–0.83 for class 2: early rapid growth; 0.69–0.82 for class 3: early weight loss, late rapid growth; 0.83–0.89 for class 4: suboptimal growth). Adherence to 400 IU Vitamin D ≥ 1 year was significantly associated with less likelihood of being in class 3 (odds ratio 0.17).
Conclusions
Among infants and toddlers aged 0 to 2 years, dietary supplementation of vitamin D is insufficient in rural areas of China. Insufficient vitamin D intake was found to be associated with suboptimal BAZ growth at early stages. Effective collaboration is needed between pediatricians and caregivers, to assure adherence to the nutritional guideline.
Introduction
The incidence of childhood obesity in China has increased dramatically in recent years, which has become a public health threat for Chinese children, 1 as in many low- and middle- income countries confronted with similar challenges.2,3 Surveillance data reveal that in 2015, China had the highest number of obese children (15.3 million) worldwide. 4 Although considerable attention has been given to addressing this issue, national progress toward preventing childhood obesity remains unbalanced. The problem is more prominent in urban areas but the prevalence of overweight and obesity in rural areas has caught up quickly over the past decade. 5 Growth acceleration during infancy, mainly driven by inappropriate parental feeding and behaviors, has been found to increase the susceptibility to being overweight and obese among young school-age children in rural western China. 6 Rapid gain in the body mass index (BMI) during early stages of growth (0–2 years) increases subsequent obesity risk.7,8 Nearly half of children who are overweight at age 2 years may develop obesity or remain overweight in adolescence, 9 which are both linked to a series of health risks in adulthood. 10 Therefore, interventions to prevent childhood obesity should focus on the first 1000 days of life, that is, from before birth to age 2 years. 11
Vitamin D is an indispensable micronutrient that has numerous biological effects on children’s growth and development. 12 There is strong consensus that infants should receive daily vitamin D supplementation during the first year of life, to establish a healthy vitamin D status.13,14 Moreover, there is growing concern over the association between vitamin D and pediatric anthropometric status, considering that adipose tissue has been identified as an extraskeletal target of the vitamin D endocrine system. 15 Cross-sectional studies have confirmed that sufficient vitamin D concentrations among children and adolescents are associated with lower risks of cardiovascular disease and metabolic syndrome.16,17 By contrast, an inverse significant correlation between low plasma 25-(OH)vitamin D (25OHD) and obesity has also been reported.18–20 However, it remains unclear whether vitamin D repletion influences childhood BMI-for-age Z score (BAZ) patterns at young ages, which could be important because early growth during the first 2 years of life predicts the prevalence of obesity and other noncommunicable diseases (NCDs) later in the life course.21,22
In this paper, we aimed to assess the hypothesis that 1) the dosage of vitamin D supplementation is associated with early BAZ growth patterns; 2) high adherence to the recommended dietary allowance (RDA) of daily vitamin D intake (400 IU/day) for at least 1 year is associated with optimal BAZ trajectories, and low adherence could lead to unsatisfactory outcomes.
Methods
Study design and participants
The study was conducted in a low-income rural area of southwestern China, Zhenxiong County, Zhaotong City, Yunnan Province. 23 This area is geographically located on the Yunnan–Guizhou Plateau on the Chinese mainland at 630 to 2416 m above sea level.
A series of observational retrospective longitudinal data was generated from routine physical examination of children who were registered at birth and followed up during 0 to 24 months in the Health Center of Wude Town, Zhen Xiong County, Zhaotong City, Yunnan Province. This center was selected as it is a collaborative institution of Shanghai Children’s Hospital affiliated to Shanghai Jiao Tong University, and members of the research team are active volunteer pediatricians at this center. This study received exemption from an ethics review by the Research Ethics Commission of Zhen Xiong People’s Hospital because the study involved the use of existing data. The requirement for participants’ signed informed consent was waived as the data were de-identified and all identifiable private information of participants could not be ascertained by any means.
Anthropometric measurements and nutritional assessment
For anthropometric measurements, one research assistant participated on the physical examination team of Wude Health Center between May 2016 and June 2018. All parents were informed about the physical examinations via notification from the local villagers' office. An electronic length and weight scale was used to assess the recumbent length and weight of children, measured by well-trained professionals following the guidance of the World Health Organization. 24 Measurements were obtained with children wearing light clothing and no shoes. Weight was measured to the nearest 0.1 kg and length to the nearest 0.1 cm. The raw measurements of length and weight were converted to weight-for-age Z-score (WAZ) and BAZ using the World Health Organization sex- and age-specific reference standards (WHO Multicenter Growth Reference Study Group 2006 25 ).
Vitamin D supplementation and covariates
The primary variable of interest was infant daily vitamin D intake. At each health visit during the first 2 years, this was measured by questioning mothers in face-to-face interviews, as follows: “At what dosage and for how long has your child been supplemented with vitamin D (prescribed vitamin D and any vitamin D supplements)?” Supplementation for each infant was clearly recorded; data of brands were not collected. The daily use was calculated by considering both dose and frequency. 26 For example, if an infant consumed 400 IU vitamin D every day, the daily use would be 400 IU; if the dosage was 400 IU every other day, the daily dose was considered to be 200 IU/day. We also included covariates of sex, gestational age (weeks), birth weight Z-score, 27 maternal age at delivery (years), 28 maternal education attainment 29 (<12 years, illiterate to primary school graduate; ≥ 12 years, middle school graduate and over), season of birth, 30 whether exclusively breastfed during the first 6 months, 2 and duration of daily outdoor activity (hours). 31
Analytical procedure
Data pre-processing
Among 2100 newborns registered in the system, 1233 infants who were followed up had complete data on anthropometry and vitamin D use at birth, 3 months (12–16 weeks), 6 months (24–28 weeks), 1 year (10–14 months), 1.5 years (16–20 months), and 2 years (22–26 months). Selection of these age time points was designed to create a more robust growth curve at similar follow-up times using comparable anthropometric data. 32 We excluded 51 preterm (gestational age [GA] < 37 weeks) and post-term (GA ≥ 42 weeks) infants from the analysis because the WHO growth trajectories were not applicable to these infants. 33 Infants with unreasonable BAZ (<−5 or WAZ > 5) at any of the abovementioned time points were excluded (n = 23) owing to potentially incorrect data entry.
Growth patterns and grouping
To derive different BAZ growth patterns, we performed a latent class growth modeling (LCGM) analysis, a technique designed to identify homogeneous subgroups within a heterogeneous population 34 that is very applicable to the study of longitudinal developmental trajectories at early stages.7,32 The number of BAZ growth profiles was decided on the basis of the Bayesian information criterion (BIC); models with smaller values of the BIC imply a better fit.
Statistical analysis
Standardized BAZ and WAZ at birth were estimated using the publicly available software, WHO Anthro 3.2 (https://www.who.int/growthref/tools/en/). Other statistical analysis was carried out using RStudio (The R Project for Statistical Computing, Vienna, Austria). LCGM analysis was performed using the “poLCA” package in RStudio. 35 Frequencies with percentage or means with standard deviation (SD) of basic characteristics were calculated, as descriptive statistics. Logistic regression models were performed to estimate the effects of vitamin D use on BAZ growth when covariates were controlled. Relationships between daily supplementation with 400 IU ≥ 1 year and BAZ growth patterns in early childhood were also assessed in the logistic regression model, where the dosage of vitamin D was divided by 100.
Results
In total, 1159 eligible infants and toddlers were included in the final analysis. The characteristics of the study population are summarized in Table 1. Boys accounted for 56.6% of the final sample. The mean age of gestation was 39.8 weeks, with an average birthweight Z-score −0.2.
Characteristics of study participants identified using latent class growth modeling: Zhenxiong, Zhaotong, Yunnan, China 2016–2018 (n = 1159).

1Chi-square tests were performed to determine the P value for categorical variables. Results are expressed as number (percentage).
2Analysis of variance was adopted to determine the P value for continuous variables. Results are expressed as mean (standard deviation).
3Z-scores were calculated according to age- and sex-specific World Health Organization child growth standards.
4Maternal higher education was defined as completing > 12 years education.
5Comparison among growth patterns.
6Comparison between term infants included and excluded in the analysis.
EBF, exclusively breastfed.
Growth trajectories in the first 2 years
Using LCGM, the BIC outputs for the fitted models from two to six growth categories were 18,601.46, 18,116.95, 17,981.84, 17,946.97, 18,001.04. Therefore, the BAZ growth of the study population was divided into five categories, as depicted in Figure 1.

Five BAZ growth patterns of infants and toddlers in the first 2 years according to LCGM
Trajectory class 1, comprising 42.4% of the study population, was termed “normative growth”. These children had mean estimated BAZ −0.20 at birth and showed an optimal normative growth pattern around standard levels. BAZ growth class 2, denoted “early rapid growth”, comprised 10.9% of children. This trajectory class showed a rapid weight gain early, within the first 3 months of life, and remained 1 unit above the ideal growth standards until 2 years of age. BAZ growth trajectory class 3 (8.9%), “early weight loss, late rapid growth”, included children who experienced weight loss during the first 3 months but who were substantially accelerated by 2 SD within the following 2 years. The BAZ trajectory class 4 comprised children with unsatisfactory growth, close to mild malnutrition status, 36 which continued to decline over time to 1 SD below the standard level until age 2 years; this class was termed “suboptimal growth” and comprised 12.5% of the study population. The trajectory class 5, “early normative, late rapid growth”, showed a pattern similar to normative growth in the first 6 months but then deviated by +1 SD above standard growth; this class comprised 21.9% of the whole sample.
Using analysis of variance or chi-square tests, some disparities in the distribution of demographic characteristics were observed among the different groups. Therefore, the heterogeneity of participant characteristics was accounted for by adjusting for potential confounders (Table 1). The table also presents the difference between included and excluded term newborns in this study, in which most characteristics were not significantly different at baseline.
Status of supplemental vitamin D use
Data on the proportion of children who were ever given supplemental vitamin D at each visit are shown in Figure 2. Overall, the highest proportion of children routinely receiving supplemental vitamin D at most visits were those with normative growth (trajectory class 1). By contrast, fewer than 25% of children in class 3 (early weight loss, late rapid growth) ever received vitamin D within the first 2 years of life. In terms of adherence to the recommendations, in general, only 37.1% of the study population received supplemental vitamin D ≥ 1 year. As displayed in Figure 3, class 1 (normative growth) accounted for the highest percentage (41.8%) of participants who received at least 400 IU vitamin D supplementation daily for the first year. Significant differences were found when comparing class 1 with classes 3 (early weight loss, late rapid growth, p < 0.001) and 4 (suboptimal growth, p = 0.003).

Proportion of children who received supplemental vitamin D at each visit.

Proportion of children who received at least 400 IU vitamin D daily for 1 year in each group
Vitamin D supplementation and growth trajectories
We analyzed the association between daily vitamin D intake dosages and BAZ growth patterns, as shown in Table 2. In comparison with those who had normative growth (class 1), children in classes 2 ,3, and 4 had, respectively, 0.60 to 0.83 (class 2), 0.69 to 0.82 (class 3) and 0.83 to 0.89 (class 4) times the risk of having early or late rapid weight gain with every 100 IU/day vitamin D increase, suggesting that vitamin D supplementation had a protective effect against rapid growth.
Logistic regression for daily dose vitamin D (unit: 100 IU) according to growth trajectory at all visits: Zhenxiong, Zhaotong, Yunnan, China 2016–2018 (n = 1159).
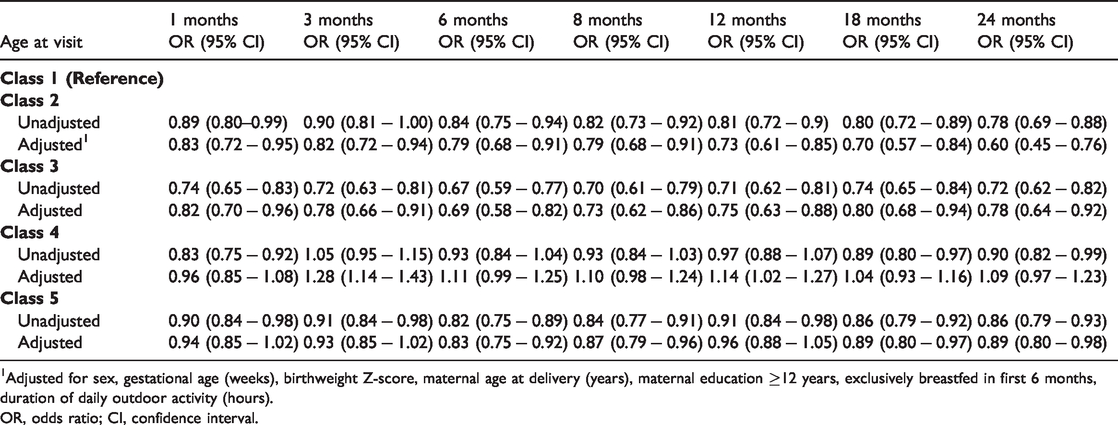
1Adjusted for sex, gestational age (weeks), birthweight Z-score, maternal age at delivery (years), maternal education ≥12 years, exclusively breastfed in first 6 months, duration of daily outdoor activity (hours).
OR, odds ratio; CI, confidence interval.
The odds ratios (ORs) of the covariate models are presented in Table 3, which demonstrated that 400 IU vitamin D daily for < 1 year (as compared with adherence to 400 IU vitamin D per day ≥ 1 year) was related to the type of BAZ growth pattern that a child had the greatest likelihood of developing. Compared with reference class 1, infants who received daily 400 IU for ≥ 1 year showed 0.17 greater odds of developing rapid weight gain prior to 2 years of age (class 3). The association remained significant (OR 0.17, 95% CI 0.04–0.50, p < 0.001) after accounting for all relevant covariates (model 2). A similar association was found for class 4, which indicated that infants with maternal adherence to the recommendations had a 0.53-fold decreased likelihood of suboptimal growth (OR 0.53, 95% CI 0.35 − 0.80, p = 0.003), even though this association was attenuated when the covariates were fully adjusted. A similar association was found for class 4, which indicated that infants with maternal adherence to the recommendations had a 0.53-fold decreased likelihood of suboptimal growth, even though this association was attenuated when the covariates were fully adjusted.
Association of daily vitamin D supplementation ≥12 months with growth patterns in the first 2 years: Zhenxiong, Zhaotong, Yunnan, China 2016–2018 (n = 1159).

Discussion
The main findings of our study were that additional vitamin D intake in infancy has benefit in the development of optimal BAZ growth, and low or no vitamin D supplementation is more likely to be associated with poor growth outcomes during the first 2 years of life. Our results lend support to the recommendation that adherence to the RDA of 400 IU/day vitamin D for 1 year increases the likelihood of a better growth trajectory in comparison to supplementation for less than a year. Although the benefits of vitamin D with respect to calcium and bone homeostasis have been adequately demonstrated, little evidence as to the effects of vitamin D on BAZ growth for infants and toddlers during the first 1000 days is available. We believe that our results will serve as a basis for further studies on the vital clinical importance of early micronutrient supplementation for body growth and the prevention of obesity later in life. Our findings also highlight the importance of collaboration between pediatricians and caregivers in implementing nutritional guidelines in developing countries, particularly in rural areas.
We note that at most age time points, infants with higher vitamin D intakes were more likely to have a normative BAZ growth pattern. In other words, relatively low doses or no use of vitamin D was associated with the risk of excess BAZ growth. To our knowledge, limited longitudinal studies exist regarding the association between vitamin D intake and infant BAZ patterns. A Polish cross-sectional study reported that a greater percentage of children aged 1 to 3 years did not achieve adequate vitamin D intake among obese children than normal weight children. 37 Weker et al. also detected an insufficient supply of vitamin D among overweight and obese toddlers. 38 Conversely, vitamin D administered to children was not linked to anthropometric benefits in a trial conducted during pre-puberty, 39 when the demand for nutrients for rapid growth is not high as in infancy. Clearly, these findings require replication in other cohort studies.
Nutritional intake and ultraviolet B radiation-induced synthesis in the skin are both natural sources of human vitamin D. However, few foods contain vitamin D 40 and infants, whose skin is thinner, are more vulnerable to DNA damage caused by exposure to direct sunlight. 41 Moreover, attaining adequate 25OHD concentrations is challenging for children residing at high altitudes, 42,43 such as the participants in our study, which highlights the need for additional intake despite adequate sunshine. Vitamin D supplementation has been shown to generally protect against low 25OHD in systematic reviews and meta-analyses.44,45 Similar to other scientific or governmental nutritional guidelines, e.g., the Institute of Medicine 46 and guidelines in the United States 47 and Canada, 48 a dose of 400 IU per day vitamin D is recommended from birth until age 12 months by the Chinese Nutrition Society. Nevertheless, we found that only a few parents or caregivers in this study had adhered to this recommendation. Surprisingly, over one-third of infants received no vitamin D supplementation in the first year, and the percentage of toddlers who received vitamin D supplements decreased with increased age. Pediatricians play a critical role in ensuring that infants receive adequate amounts of vitamin D because advice from these health care professionals is considered more reliable among child care providers. 49 In rural areas, where mothers have lower education levels and limited access to nutrition-related knowledge, pediatricians hold an important position in protecting child health.
Among all covariates, we noted that children with longer durations of outdoor activity were less likely to have rapid weight gain within the first 2 years. This may be attributable to the benefits of sunshine exposure, leading to vitamin D synthesis. 50 Maternal education more than 12 years was also a protective factor that had impact on BAZ growth in this low-income area, as in studies conducted in other developing parts of the world. 51
There are some limitations in the study. Nearly half of the registered newborns were unavailable for follow-up at all time points, largely owing to migration losses, which might cause potential selection bias in relation to vitamin D supplementation. Use of vitamin D was self-reported by caregivers and could possibly result in social desirability bias and recall bias regarding actual feeding behavior. Under the conditions at local health centers, biomarkers such as 25OHD were unable to be measured. As a common problem in observational research, we could not consider all possible covariates. For example, we did not include factors related to maternal nutrition and cutaneous synthesis of vitamin D, e.g., habitual clothing and skin pigmentation.
Conclusions
Among infants and toddlers aged 0 to 2 years, sufficient dietary supplementation with vitamin D is lacking in rural areas of China. Insufficient vitamin D intake was found to be associated with suboptimal BAZ growth at early stages. Vitamin D intake of at least 400 IU/day, sustained for the first 1 year of life, resulted in improved body growth within 0 to 2 years. Effective collaboration between pediatricians and caregivers is needed, to assure adherence to the nutritional guideline.
Footnotes
Acknowledgements
The authors thank the study participants, their parents, and doctors at Wude Health Center, as well as the researchers in this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Shanghai Municipal Committee of Science and Technology (grant numbers: 16411970100, 18411967700); Shanghai Children's Health Services Capacity Planning Special Program for Advanced Pediatric Overseas Research Team Training Program (grant number: GDEK201710); and Shanghai Municipal Health Commission (grant number: GWV-10.1-XK19).