
Abstract
Objective:
This study aimed to assess the incidence and associated factors of acute postoperative pain after cesarean section within the first 24 h of postoperative period.
Methods:
An institutional-based prospective observational study was conducted on parturients who had undergone cesarean section in Gandhi Memorial Hospital from 1 December 2019 to 28 February 2020. A numerical rating scale was used to evaluate the incidence of acute postoperative pain. Patients having a pain score of >4 were considered having moderate-to-severe pain on numerical rating scale. Data were analyzed using SPSS version 20. Bivariable and multivariable logistic regression were used to assess the association of variables. A p value of less than 0.05 was taken as significant association with dependent variables.
Result:
In total, 290 parturients participated in the study with a response rate of 98%. Moderate-to-severe acute postoperative pain after cesarean section was 76.2% (95% confidence interval: 71%, 81%) in the first 24 h postoperatively. On multivariable analysis, previous cesarean section history (adjusted odds ratio: 2.80, 95% confidence interval: 1.40, 5.55; p = 0.003), preoperative anxiety (adjusted odds ratio: 2.70, 95% confidence interval: 1.45, 5.05; p = 0.003), transverse incision type (adjusted odds ratio: 3.35, 95% confidence interval: 1.67, 6.72; p = 0.002), and incision length (adjusted odds ratio: 2.46, 95% confidence interval: 1.24, 4.85; p = 0.009) were identified as risk factors for postoperative moderate-to-severe acute pain.
Conclusion:
The incidence of moderate-to-severe postoperative pain was high in the first 24-h postoperative period; this indicates that pain management after cesarean section was treated inadequately. History of previous cesarean section, preoperative anxiety, transverse incision, and incision length >10 cm were the factors of postoperative acute pain after cesarean section. Therefore, we suggest the study institution develop a protocol for pain management.
Introduction
Pain is a symptom of sensory and emotional experience influenced by physiological, psychological, and situational factors. Based on the International Association for the Study of Pain (IASP), pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”1–3
Cognitive and emotional patient characteristics together with other multiple factors such as age, gender, level of preoperative pain, and negative psychological conditions such as anxiety and depression were found to be very important risk factors for postoperative pain.4,5
Severe postoperative pain affects the performance of daily activities and it contributes to persistent postoperative pain. In patients submitted to cesarean section (CS), pain can also interfere with women’s ability to care for their babies, breastfeed effectively, and interact with their children satisfactorily. 6 Self-reporting pain assessment is one of the most accurate methods; from this, the numerical rating scale (NRS) is easy or less complicated to understand. 7 Among different techniques of postoperative pain management, pharmacological methods are most common which include opioid analgesics, non-steroidal anti-inflammatory drugs (NSAIDs), and regional techniques. 8 Effective and adequate postoperative pain management increased patient ambulation, decreased the risk of morbidity, and improved the maternal and fetal outcomes. 9 CS is associated with postoperative pain which can result in a negative impact both on the mother and the newborn at the postoperative period. Pain after cesarean birth can be related to postoperative pain from the wound and uterine contractions. Generally, multiparas experience more painful postpartum contractions than primiparas. 6
Acute postoperative pain is the most common and anticipated problem after CS as data obtained from developing country hospitals showed 62% pain incidence in all surgical procedures; from this, incidence of acute post-CS pain was 87%. 10 Untreated postsurgical pain results in reduced patient satisfaction, increases morbidity and mortality, and places a burden on health care finances. Moreover, the progression of acute postsurgical pain (APSP) to chronic postsurgical pain (CPSP) can affect the quality of life, interfere with daily activities, and result in physical disability. Therefore, early identification and adequate management of postsurgical pain is vital. 11 There are many options of treatment modalities of pain management after CS but there is no standard guideline specific to postoperative pain management after CS. Among treatment modalities are systemic and intrathecal administration of opioids, patient-controlled analgesia (PCA), and intramuscular (IM) injection of NSAIDs, and regional nerve blocks. Mostly these pain management modalities are applied as part of multimodal analgesia, which results in additive or synergistic analgesia with lowered side effects. 12
Even though pain management is advanced as such, parturients experience moderate-to-severe acute pain in the postoperative period, which was recognized as a major clinical problem that affects the mother and her baby. 13 Studies done in America, Europe, and Asia reported incidence rate of moderate-to-severe pain after CS is 78.4%–92% due to barriers in attitudes and educational status of both health care providers and patients about analgesics use and lack of adequate pain management service.14–16
Pain in developing countries including Ethiopia is the most ignored medical practice. Therefore, this study aimed to assess the incidence and associated factors of acute postoperative pain after CS within the first 24 h of the postoperative period in Gandhi memorial women and child care hospital, Addis Ababa, Ethiopia, 2020. The primary outcome of this study was incidences of moderate-to-severe pain and factors associated with pain. As secondary outcome, we studied the analgesic requirement of parturients during 24-h period.
Methodology
Before the study, ethical clearance was obtained from the Departmental Research and Ethics Review Committee (DRERC) of Department of anesthesia, School of Medicine, College of Health Sciences of Addis Ababa University and acceptance was also obtained from the study institutions (Gandhi memorial and child care hospital). Moreover, full clarification about the purpose of the study was made to the authorized person of the health facility. The purpose of the study was explained to the patients who were included in the study. Written informed consent from the patients was obtained, and confidentiality of the information was assured using code numbers and keeping questionnaires locked. Patients who were in pain during this study period were treated by their caregiver, who are informed by the data collector. Even though there are studies about the incidence and associated factors of postoperative pain after CS in developed countries, there is limited evidence in Ethiopia. Therefore, we conducted an institutional-based prospective follow-up study in Gandhi memorial women and child care hospital Addis Ababa, Ethiopia from 1 December 2019 to 28 February 2020. We included both elective and emergency CS. The indications for CS were maternal-related and fetal-related; in electives cases, most of them were previous CS/ scar, preference of mothers, oligohydramnios, and twin pregnancy. For emergency cases, non-reassurance fetal status/ fetal brady/tachycardia, preeclampsia, eclampsia, uterine rupture, antepartum hemorrhage, cephalopelvic disproportion (CPD), bad presentation of fetus, and fetal asphyxia were among indications. All parturients who gave birth by CS under general anesthesia and regional anesthesia were included except patients with cognitive dysfunction, inability to communicate, and ongoing treatment of chronic pain.
The sample size was calculated by single proportion formula using the prevalence of 50% because there was no previous study done in Ethiopia context and 5% margin of error at the 95% confidence interval using the following formula

where n = sample size, z = 1.96, p = 0.5, d = 0.05, CI = 95%.
And α = 5%.

where nf = n/(1 + n/N) in which N = 873 (estimated target population in the study period).
So
We added 10% of nf for the non-response rate (i.e. 267 + 26 = 293). Therefore, the final sample size was 293 (Figure 1).

Flow of participation chart.
Every voluntary parturient fulfilling the criteria of inclusion was selected until the required sample size was achieved by consecutive sampling method undergoing CS in Gandhi memorial women and child care hospital obstetric ward by signing informed consent from 1 December 2019 to 28 February 2020.
Three data collectors and one supervisor were assigned; two BSc nurses, one BSc anesthetist, and one MSc anesthetist as supervisor were trained on NRS and patient interview by the questionnaire. In validation of the questionnaire, two assistant professors of anesthesia and two post-anesthesia care unit nurses who have more than 10 years of experience involved in the reviewing accuracy, comprehensiveness, clarity, and relevance of the questionnaire in the study setup.16–20 The researchers revised and finalized the validated tools based on the expert’s recommendations. Then pretest was done on 5% of the sample size at Zewditu Memorial Hospital to check the validity of the questionnaire (available as a supplementary file). A detailed explanation was also given to the participants on how to point their pain intensity on NRS in the preoperative clinic. On the day of surgery, additional information was given to each patient in the waiting room, then the written informed consent of participation was taken. Data collection procedure was including a chart review and an interview-based questionnaire. In our study hospital, there was no guideline of pain assessment timeline and management; therefore, patients received anti-pain only when they requested analgesia for their pain. The data collectors reviewed the chart and documented the pain score using an NRS at 2, 12, and 24 h postoperatively. At the same time, the given analgesics were also documented. The supervisor was controlling the data quality and its completeness at the end of data collection for a single participant. A structured and pretested questionnaire consisting of an NRS was done in 24 h; first postoperatively at 2 h after the operation, second on 12 h, and third at 24 h. Pain in NRS was described as 0: no pain, 1–3: mild pain, 4–6: moderate pain, and 7–10: severe pain. 17 Motor and sensory senses were checked whether the parturient was free of spinal anesthesia or not. 18 The ward and bed number of the parturients had been written by the data collector before the parturient left the post-anesthesia care unit (PACU). Patient’s preoperative assessment, socio-demographic characteristics, intraoperative status, analgesic medication, and postoperative events were obtained from their medical record. The supervisor was controlling the data quality and its completeness at the end of data collection for a single participant.
Data processing and analysis
The data were entered on EpiData software version 7 and were transferred to SPSS version 20 computer program for analysis. Descriptive statistics were used to summarize data, tables, and figures for display results. The association among independent factors and the outcome variable were determined by chi-square test, bivariable, and multivariable logistic regression. The statistical significance was p < 0.2 for bivariable and p < 0.05 for multivariable regression. Crude and adjusted odds ratios were used to see the strength of the association for bivariable and multivariable logistic regression, respectively. A p-value of less than 0.05 was considered statistically significant. Hosmer–Lemeshow test was applied to check the goodness-of-fit.
Operational definitions
Acute pain. The pain experienced immediately after tissue injury for a short duration of time with the exclusion of a given length of time, the tissue heals and the pain resolves, usually lasting for days. 18 Moderate-to-severe pain: patients having a pain score of >4 on an NRS. 16
Anxiety. It is a fundamental phenomenon and the central problem of neurosis and the most pervasive psychological phenomenon of our time. 19
NRS. It is a valid pain intensity assessment tool that involves asking a patient to rate pain from 0 to 10 (11-point scale) with the understanding that 0 is equal to no pain and 10 is equal to the worst possible pain. 20 Acute pain can be reliably assessed with tools such as NRS or Visual.
Analog scales, both NRS and visual analog scale (VAS), for the assessment of pain intensity are equally sensitive in assessing acute pain after surgery and superior to verbal rating scale; but here in our study, NRS was more applicable because it is uncomplicated and parturients able to understand easily. 20
Result
Socio-demographic characteristics and severity of pain of the respondents
A total of 290 parturients were recruited in the analysis with 100% response rate, but three parturients were excluded due to incomplete data. Age, body mass index (BMI), marital status, and level of education were assessed in this character. In total, 71% of the parturients were between the ages of 18–34 years. The majority of parturients were BMI of between 18.5 and 24 (71.0%), and parturients who were married were 160 (55.2%). The educational status of 107 (36.9%) parturients was college and above. Moderate-to-severe postoperative pain within 24 h was higher than none to mild pain in all socio-demographic variables (Table 1).
Frequency, percentage of parturients response, and cross-tabulation of socio-demographic characteristics versus their postoperative pain after cesarean section in Gandhi memorial and child care hospital, Addis Ababa, 2020 (n = 290).
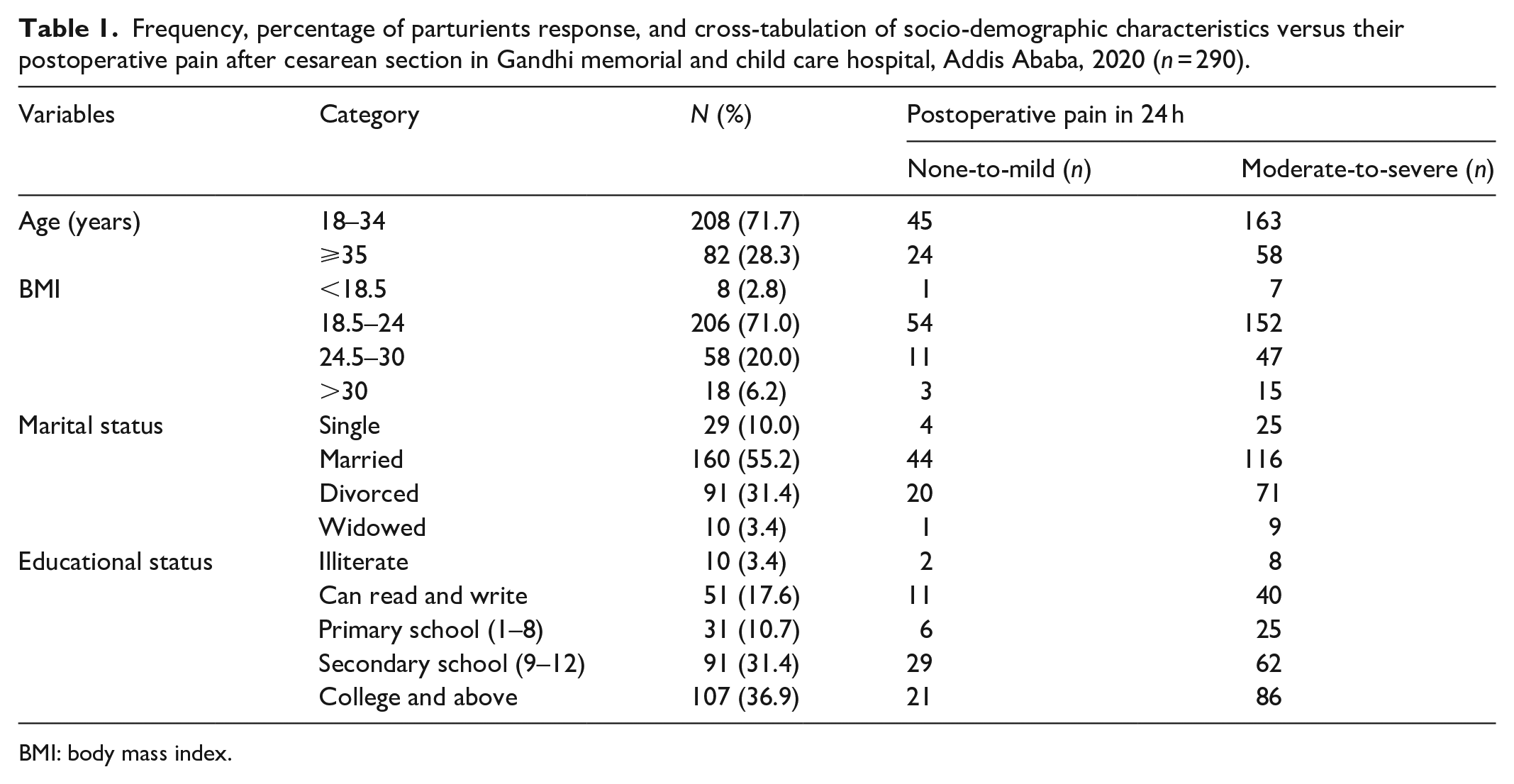
BMI: body mass index.
Preoperative factors
Based on preoperative factors, greater numbers of the respondents were ASA II 250 (86.2%). About 86% of the parturient did not get perioperative analgesia and that parturient who had a history of previous CS were 222 (76.6%). In total, 180 (62.1%) parturients experienced preoperative anxiety. None-to-mild and moderate-to-severe pain experiences of parturients are set with different variables (Table 2).
Frequency, percentage of parturients response, and cross-tabulation of preoperative factors versus their postoperative pain after cesarean section in Gandhi memorial and child care hospital, Addis Ababa, 2020 (n = 290).

Intraoperative factors
From intraoperative factor distribution, most of the participants were incised transversely (79.3%); however, parturients who had been done by spinal anesthesia were 228 (78.6%), whereas parturient with an incision length of ⩾10 cm was 206 (71.0%) and the frequency of pain severity also mentioned in Table 3.
Frequency, percentage of parturient response, and cross-tabulation of intraoperative factors versus their postoperative pain after cesarean section in Gandhi memorial and child care hospital, Addis Ababa, 2020 (n = 290).

Analgesics given postoperatively
Parturients were given different types of systemic analgesia at different times in postoperative conditions. From that systemic analgesia, tramadol was frequently given (29.7%) at 2 h, whereas 28.6% of the parturients did not take any systemic analgesia. In 12 h, diclofenac was given (49.0%) most commonly, and some others were not given (3.8%). At 24 h, diclofenac was also given (37.9%) frequently; however, some other parturients were not given analgesia (34.1%) (Figure 2).

Systemic analgesia given in the postoperative period after cesarean section in different time intervals 2, 12, and 24 h of study participants in Gandhi memorial women and child care hospital, Addis Ababa, 2020 (n = 290).
Postoperative pain incidence
The incidence of moderate-to-severe pain after CS among parturients was 53.4%, 75.9%, and 52.8% at 2, 12, and 24 h, respectively (Figure 3). All in one, incidence of postoperative moderate-to-severe pain after cesarean delivery was 76.2% (95% CI: 71%, 81%) in the first 24 h of postoperative NRS pain assessment method (Figure 3).

Acute postoperative pain reported after cesarean section in different time intervals in Gandhi memorial and child care hospital, Addis Ababa, 2020 (n = 290).
Factors associated with incidence of acute postoperative pain within 24 h
We analyzed the variables in both bivariable and multivariable methods to determine the independent association between postoperative pain and factors of acute pain. On the bivariable analysis method, age, marital status, previous CS, ASA status, preoperative anxiety, incision type, incision length, anesthesia type, and anesthesia time were with p value less than 0.2 (Table 4). However, only the following variables were found to have association with moderate-to-severe pain in the post-CS—patients with previous CS were 2.8 times to had moderate-to-severe pain than those who had no history of previous CS, p = 0.003 (adjusted odds ratio (AOR): 2.8, 95% CI: 1.40, 5.55); patients with preoperative anxiety were also 2.70 times to experience moderate-to-severe pain than those who were not anxious preoperatively, p = 0.002 (AOR: 2.70, 95% CI: 1.45, 5.05); however, patients who were incised with transverse line were 3.35 times to respond moderate-to-severe postoperative pain than those who were incised in midline type, p = 0.001 (AOR:3.35, 95% CI: 1.67, 6.72); the study also showed that patients with incision length of ⩾10 cm were also experienced 2.46 times moderate-to-severe post-cesarean acute pain than those with incision length of <10 cm, p = 0.009 (AOR:2.46, 95% CI: 1.24, 4.85) (Table 4).
Factors associated with postoperative pain analyzed in both bivariable and multivariable logistic regression in Gandhi memorial and child care hospital, Addis Ababa, 2020.

Variables significant in the bivariable logistic regression analysis (p < 0.2).
Variables significant in the multivariable logistic regression analysis (p < 0.05).
1.00 Reference/indicator.
Discussion
This study intended to find out the incidence of post-CS moderate-to-severe acute pain in the first 24 h and to confirm whether there is an association between the demographic, preoperative, intraoperative, and postoperative factors as relevant explanatory power of postoperative acute pain incidence or not.
We assessed the incidence of postoperative pain in 290 parturients who had undergone CS. In this study, incidence of moderate-to-severe pain has been found as 53.4%, 75.9%, and 52.8% at 2, 12, and 24 h, respectively. The overall incidence of moderate-to-severe acute pain within the first 24 h after CS was 76.2% (95% CI: 71%, 81%). Although there are many different types of pain management practice standards and guidelines worldwide, this study indicates that there is inadequate treatment of postoperative pain after CS. As data obtained from studies, postoperative acute pain after CS is undertreated and continued to be undermanaged.20,21
In agreement with our finding, a descriptive patient survey conducted in Sweden in women undergoing cesarean delivery reported about 78% of moderate-to-severe pain with a score of ⩾ 4 on the VAS indicating pain as inadequately treated. 6 Another longitudinal study in Brazil on 1062 women undergoing CS reported a high incidence (78.4%) of moderate-to-severe acute postoperative pain which was almost agreed with our findings. 15 The above studies are almost consistent with our finding. There is also another study conducted in South Africa on surgical patients consisting of CS, from those total procedures patients with CS had reported the largest incidence (87%) of moderate-to-severe acute postoperative pain. 10 This finding is slightly higher than ours, as parturients with CS procedures in this study were not given adequate systemic analgesia in the postoperative conditions relative to our cases which might be the possible reason for this difference. 10 Our study was also evidenced by another prospective longitudinal study which was conducted in Brazil on postoperative pain in women undergoing CS was reporting high incidence (92.7%) of moderate-to-severe acute pain after CS, 16 the reason for this big difference from our finding was that women were having tubal sterilization procedures in addition to CS that might lead to more extensive and manipulation of surgery which in turn results more pain. Study that investigated the quality of postoperative pain management in Jimma University also reported moderate-to-severe pain as 88.2%; 22 even though both studies were done in Ethiopia, the study which was conducted in Jimma included other general surgery procedures other than CS, and thus might cause more incidence of postoperative pain than our finding. An institutional-based cross-sectional study on severity and risk factors of postoperative pain was conducted in University of Gondar concluded that moderate-to-severe pain were 57%, 78%, and 53% at 2, 12, and 24 h, respectively, and both studies in Jimma and Gondar Universities implied inadequate treatment of postoperative pain in Ethiopia. 17
Postoperative moderate-to-severe acute pain after CS was also found in a sample of 1288 women investigated by a prospective follow-up study in New York, where the incidence within 36-h post-delivery was 10.9%, 23 which shows lower incidence than ours. This is not unexpected in New York; many factors can be considered inconsistent with our finding. Very good clinical practice, use of multimodal analgesia, and regional nerve blocks as postoperative analgesia make lower finding than ours, whereas our study was done in a site where poor clinical practice and less standardized pain management model applied, which results high incidence of postoperative moderate-to-severe acute pain than that of New York.
Another prospective institutional-based study done in Mulago on women who were delivered by CS under spinal anesthesia had reported moderate-to-severe pain as 11%, 14%, and 6% at 0, 6, and 24 h, respectively. 24 However, in our study, the incidence was higher in different time gaps, 53.4%, 75.9%, and 52.8% at 2, 12, and 24 h, respectively, and the possible reason for this visible variation from our study could be that the study in Mulago was done only in spinal anesthesia which was not wearing off with 0-h postoperative time and this could mask the incidence of pain during data collection time; in addition to this, patient with general anesthesia may recover earlier than spinal which leads to the patient feels pain earlier in which our study includes and makes our finding more than Mulago.
From our findings, there was a significant association between a parturient having a previous CS and postoperative moderate-to-severe acute pain. Parturients with previous CS had 2.8 times more moderate-to-severe pain than parturient without previous CS. There was a study that agreed with our finding, a randomized control trial study in Thailand found that repeated CS had a marked effect on postoperative pain. 25 The reason for this happening was an increased postsurgical adhesions and this in turn leads to an increased operation time and more trauma that did cause postoperative pain worse.25,26
In our study, there was also a significant association between parturients who were anxious preoperatively and postoperative pain, parturients who had preoperative anxiety were 2.70 times faced more moderate-to-severe postoperative pain than those who were not anxious, and this finding was supported by a prospective longitudinal study done in Brazil directed with our finding, as preoperative anxiety increased moderate-to-severe acute postoperative pain after CS was 1.6 times than those who were not anxious, this was due to psychological change that included anxiety, frustration, and other emotional responses that had an influence on patient recovery which means high preoperative anxiety can result in moderate-to-severe pain in the postoperative period. 15
The type of incision had a significant association with postoperative moderate-to-severe acute pain after CS; patients with a transverse (Pfannenstiel) incision were 3.35 times experienced postoperative pain than those who had midline incision. The study that supported our finding was done in Thailand; it was a prospective double-blind randomized-controlled trial that compared the incidence of postoperative pain in both vertical (midline) and Pfannenstiel (transverse) incision group. It finally found that in repeated CS, incidence of postoperative pain was higher in Pfannenstiel (transverse) group than vertical (midline) group at 6 and 12 h postoperatively; but in first CS, the incidence of pain was higher in vertical (midline) group than Pfannenstiel (transverse) group, and the length of incision was 10 cm which was optimal and may be considered as the feasible rationale for this finding. 25 However, in our finding, most of our cases were incised with an incision length of greater than 10 cm (71%) and had previous CS or repeated CS (76.6%), all of these in turn made the parturient have more moderate-to-severe postoperative pain in our study.
Incision length was also significantly associated with postoperative pain incidence during our study; parturients with an incision length of ⩾10 cm were 2.46 times felt moderate-to-severe pain than those who had an incision length of <10 cm. A cross-sectional study that was done in Gondar, Ethiopia supported to our finding that parturients with incision length >10 cm reported that they experienced postoperative moderate-to-severe pain when compared to those with incision length of <10 cm. 17 The higher the increase in the length of incision, the higher the tissue injury the patient had, and this, in turn, can lead to the patient feeling more pain.
Limitation and strength of the study
Even though the multivariable logistic regression analysis showed that type of anesthesia (regional versus general anesthesia) did not affect the incidence of pain, the limitation is that it is a single-center study and we studied patients who received spinal and general anesthesia together. The strength of this study is the collection of data at a regular time intervals or follow-up style.
Conclusion
The incidence of moderate-to-severe postoperative pain was high in the first 24-h postoperative period, this indicates that pain management after CS was treated inadequately. History of previous CS, preoperative anxiety, transverse incision, and incision length >10 cm were the factors of postoperative acute pain after CS. Therefore, we suggest the study institution to develop a protocol for pain management.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221133190 – Supplemental material for Incidence and associated factors of acute postoperative pain within the first 24 h in women undergoing cesarean delivery at a resource-limited setting in Addis Ababa, Ethiopia: A prospective observational study
Supplemental material, sj-docx-1-smo-10.1177_20503121221133190 for Incidence and associated factors of acute postoperative pain within the first 24 h in women undergoing cesarean delivery at a resource-limited setting in Addis Ababa, Ethiopia: A prospective observational study by Dagim Bimrew, Abebaw Misganaw, Hirbo Samuel, Tenbite Daniel Desta and Samuel Debas Bayable in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank Addis Ababa University and the Department of Anesthesia for all their inspiring and immense contributions. They also want to thank Gandhi memorial women and child care hospital staff for their assistance and cooperation in the completion of this study. They further thank all the study participants, for their voluntary participation during data collection, and data collectors and supervisors.
Author contributions
All authors made substantial contributions to the conception and design, acquisition of data or analysis, and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Data availability
All related data have been presented within the article. The data set supporting the conclusions of this article is available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Addis Ababa University School of Anesthesia ethical review board. We received the ethical approval number (AAUMF 01-008) on 29 November 2019.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.