
Abstract
Background. Vaccine- preventable diseases constitute a major cause of morbidity and mortality in children under-5 years of age in Ethiopia and other developing countries. There are limited studies conducted on this aspect in Ethiopia especially in Gozamen district. Objectives. To assess missed opportunity for routine immunization and its associated factors among children aged <24 months in Gozamen district health centers. Methods. Institutional based cross-sectional study exit interview was conducted on 422 mothers with under 2 years old children. Data was collected using the standard World Health Organization’s missed opportunity tool. Vaccines examined in this study were BCG, OPV0, OPV1, PCV1, rota 1, penta valant 1, OPV2, PCV2, rota2, pentavalant 2, OPV3, PCV3, IPV, pentavalant 3, and measles vaccine. The vaccination status of the children was assessed by a structured questionnaire based on vaccination cards or mothers/caregiver verbal responses. Binary and multivariable logistic regression analysis were used to identify factors associated with missed opportunities for routine immunization among children aged <24 months. Result. The prevalence of missed opportunity for this study was 74.9% ; major vaccines with high missed opportunity were OPV0 (67.8), BCG (17.3%), and Measles (14%). Home delivery, lack of vaccination center near the village, unable to attend formal education and younger age (0-12 months) were independently associated with missed opportunity for routine immunization. Conclusion. The prevalence of missed opportunities for routine immunization in Gozamen district health centers was high. Health centers should give routine immunization services regularly.
Background
Immunization prevents up to 3 million deaths every year in all age groups from diphtheria, tetanus, pertussis, and measles. In 2013, an estimated 84% (112 million) of infants worldwide were vaccinated with 3 doses of diphtheria-tetanus-pertussis (DTP3) containing vaccine. Number of children under 1 year of age who did not receive DTP3 vaccine worldwide: 21.8 million in 2013 compared to 22.8 million in 2012. 1 About 29% of deaths in children 1 to 59 months of age are vaccine-preventable. Of the 136 million babies born into the world in 2011, nearly 5 million are estimated to have died before their first birthday and an additional 2 million are expected to die before reaching the age of 5. These correspond to an under-5 mortality rate of 51 per 1000 live births and an infant mortality rate of 37 per 1000. Under-5 mortality rate fail by 44%. However, 5.9 million children under age 5 died worldwide in 2015. Most of these deaths were from preventable causes.1,2
Inadequate levels of immunization against childhood diseases remain a significant public health problem in Ethiopia. So, Ethiopia has developed a strategic plan to achieve at least 90% national coverage with all vaccines by 2020. It is also planned to reduce the incidence of vaccine-preventable diseases through integrated interventions that would strengthen the overall health system. 1
But there is still shortage of researches regarding this public issue in the study area. Therefore, this study intends to evaluate the current prevalence of missed opportunity for immunization and its associated factors in the study area. The study can also be used as a reference for health care providers, health care educators, policymakers and future researchers in this and/or related fields.
Methodology
Study Area and Period
The study was conducted in Gozamen district which is located in the Northwestern (NW) part of Ethiopia around Debre Markos town. The town is 300 km NW of the capital city Addis Ababa and 265 km SE of Bahir Dar, the capital city of Amhara National Regional State. It has a total population size of 162 230 (male: 80 791; female: 81 439) and 37 728 district households.
In the study district, there are a total of total 8193 under 2 years of age children. It has 4 private clinics and 6 Government health centers. The district has 26 small administrative units which have their health posts; in each health post, 2 HEWs are assigned.
The study was conducted from March 26 to April 26 in 2019 in 6 Gozamen district health centers.
Study Design
Institutional based cross-sectional study exit interview was implemented in 6 health centers.
Inclusion criteria
➢ Mothers with under 2 year children who were attending in each Gozamen district health centers.
➢ Those mothers with under 2 year children who were volunteer to participate in the study.
Exclusion criteria
➢ Mothers with under 2 year children who were not mentally and physically capable of being interviewed.
Study Population
Randomly selected mothers with under 2 year children visiting Gozamen district health centers during the study period were the study population.
Sample Size Determination
The sample size was calculated using a single population proportion formula based on the following assumptions.
where n = minimum sample size required for the study,
d = margin of error = 0.05, Za/2 value of standard normal distribution (z = 1.96) with confidence interval of 95% and α is 0.05. P is taken by (49.1%) researches were done in Gurage zone Wolikte health center and adding a 10% non-response rate which gives a final sample size of 422.
Sampling Procedure
All Gozamen district health centers (Gozamen, Libanose, Yebokella, Geraram, Fendeka and Chertekel health centers) were included in the study. Total monthly estimated number of children in the 6 health centers during the study period was (N = 678) which shows that the monthly estimated children in Gozamen health center is 115 children, Yebokela health center 125 children, Libanose health center 108 children, Cheretkel health center 140 children, Fendeka health center 110 children and Giraram health center 80 children. Overall sample was taken proportionally from all Gozamen district health centers. Then, proportional numbers of mothers with under 2 year child were included in to the sample from each health center to make up a total sample size. Each study participant was selected using systematic random sampling technique in which every second client was interviewed in each health facility. To ensure that children were only included once, they were given ID number by data collectors after interview (Figure 1).

Sampling procedure.
Data collection procedure
The data was collected by exit interviews of mothers after they get any services for their children and themselves with modified WHO standardized tools for missed opportunity vaccination protocol using face to face interviews with pretest semi-structured questionnaires. The questionnaires were prepared in English and translated to the local language Amharic.
Data Collection Tool
Data collection training was given to 9 data collectors and 2 supervisors before data collection on the antigens, routine immunization schedule, interview methods and techniques, inclusion and exclusion criteria and data collection instrument of the study. The data was collected by exit interviews of mothers after they get any services of their children and themselves with modified WHO missed opportunity vaccination protocol questioners based on Ethiopia immunization schedule. Vaccines given for children in Ethiopia and included in this study are BCG, OPV0, OPV1, PCV1, rota 1, penta valant 1, OPV2, PCV2, rota2, penta valant 2, OPV3, PCV3, IPV, penta valant 3 and measles vaccine. Data was collected by a pre-tested questionnaire. The data collectors assess the vaccination status of the children based on vaccination cards or mothers /caregivers’ verbal responses using a structured questionnaire. The questionnaire was employed to collect important information about demographic, environmental and associated factors for the missed opportunity of immunization.
Data Analysis Technique
The data was cleaned, coded and entered in Epi data version 3.1 and transferred to SPSS version 25 for analysis. Descriptive and inferential statistics were used to present the data. Odd ratio, bivariate logistic regression analyses were computed for each independent variable and those variables with P-value ≤.25 were entered into the multivariable logistic regression model. Those variables with P-value <.05 were considered as significantly associated with the outcome variable at 95% CI and below .01 consider highly significant. The results were presented using text, tables, graphs and pie charts based on the types of data.
Ethical approval and informed consent
This study was conducted in accordance with the Declaration of Helsinki.
3
Debre Markos University reviews the protocol by its institutional research ethics review committee (ref N
Results
Socio-demographic Characteristics of the Children
A total of 422 children were included in this study. Among this, 236 (55.9%) were males and 186 (44.1%) were females. Of the mothers/caregivers, 371 (87.9%) attended antenatal care where as 51 (12.1%) didn’t. The age of study participants ranged from 0 to 23 months with a mean age was 9.96 ± 6.44 months, from which 252 (59.7%) were age below 12 months and 170 (40.3%) were above 12 months (Table 1).
Socio-Demographic and Related Characteristics of Child <23 Months in Gozamen District Health Centers, 2019.

Socio-demographic Characteristics of the Mothers
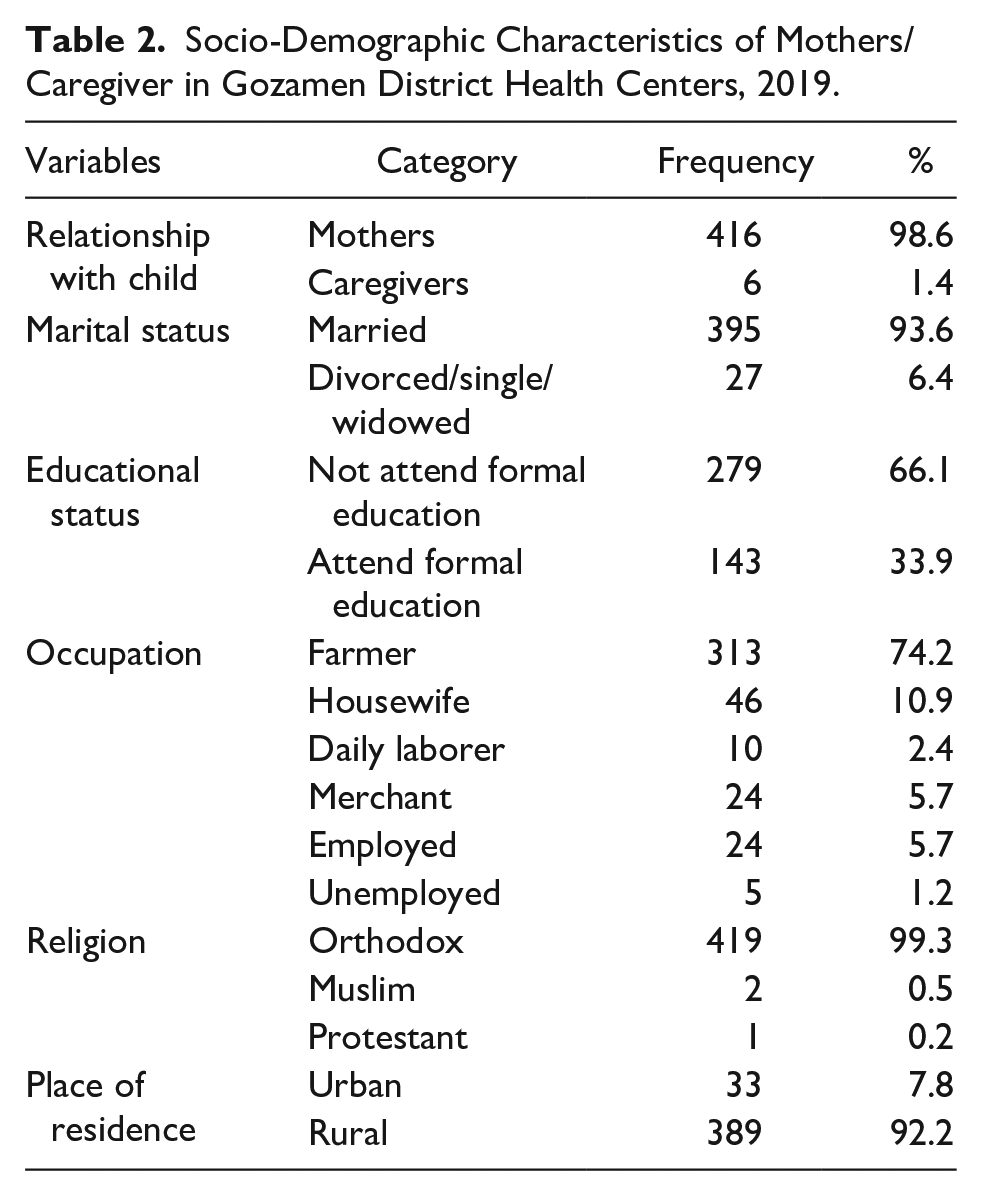
Among 422 participants visited the health facilities, 416 (98.6%) were mothers of the children’s and 6 (1.4%) were caregivers. Only 143 (33.9%) mothers/caregivers attended formal education Majority of the study participants (74.2%) were farmers (Table 2).
Socio-Demographic Characteristics of Mothers/Caregiver in Gozamen District Health Centers, 2019.
Prevalence of Missed Opportunity for Immunization
From 422 of the study participants, 316 (74.9%) missed vaccinated for age and 106 (25.1%) were vaccinated for age respectively (Table 3). Among the missed vaccinated for age were OPV0 286 (67.8%), BCG 73 (17.3%) and measles 59 (14%) (Table 4).
Prevalence of Missed Opportunity for Immunization in Gozamen District Health Centers, 2019.

NB, missed vaccinated for age refers to an eligible child has contact with a health facility and not received an eligible vaccine. Vaccinated for age refers to a child gets vaccines that are required for his/her age.
Missed Opportunity for Immunization Per Vaccine in Gozamen District Health Centers, 2019.

Possible Factors and Their Relation With Missed Opportunity for Routine Immunization
The relation between individual missed opportunity factors and vaccinated for age were assessed using multivariate logistic regression. Statistically significant association was observed between the age of children (P < .01), place of birth (P < .01), educational status (P = .045) and vaccination centres near the villages (P < .01). However antenatal care, place of residence, vaccination messages and distance reach to health facility did not show statistically significant association (Table 5).
Multivariable Analysis for Factors Associated with Missed Opportunity for Immunization in Gozamen District Health Centers, 2019.

Significant. **Highly significant.
Additional Challenges Given by Mothers
There were various reasons for missed opportunities for immunization given by mothers to their children from this, mothers too busy by social activities, fear of side effects and others are summarized below in Figure 2.

Sampling procedure.
Discussion
In this study, the prevalence of missed opportunity for routine immunization was found to be higher than previous studies in Gurage Zone Wolikte health center (49.1%) 4 and the finding of the study conducted in Siaya county referral hospital, southwest part of Kenya (16.2%). 5 The prevalence of missed opportunity were higher than the previous study pediatric outpatient clinic in Juba teaching hospital (56.5%) and Cape Tawn, South Africa (4.6%). 6 The possible difference between this finding and others may be due to socio-economic, study area and study period difference.
The current finding also showed that the prevalence of missed opportunity for immunization was higher than a systematic literature review of missed opportunity for immunization in low-and middle-income countries the pool MOI prevalence were (32.2%) 7 and research conducted in the Dominican Republic were (42.8%). 8
The finding of this study shows that most missed vaccines are OPV0 (68.7%), BCG (17.3%) and Measles (14%). However, in contrast with the previous study in Wolikte health center OPV0 was lower (35.9%) and higher in BCG (35%) and Measles (31.1%) than this study. 4 The difference may be due to the availability of lower dose vaccines in the previous time and government involvement in the immunization program.
Study finding in Siaya county referral hospital, southwest part of Kenya, mostly Rotavirus1 (18.4%), OPV3 (17.2%) and measles (24.5%) 5 higher than this study measles (14%). The current study was lower than the study conducted in a pediatric outpatient clinic in Juba teaching hospital most common for OPV3 (24.4%), DPT3 (22.1%) and measles (31.2%). 9 In India BCG 37.1% more than prevalence (17.3%) of the present study but South Africa was not BCG (5.1%), Nigeria tertiary hospital BCG (5%) was lower and measles 70% much higher than present study. 7 Dominican Republic’s were MOVs, within BCG, (11.4%) lower to the present study but, DPT (52.7%) and OPV (38.3%) higher to this study. 8 The difference may be due to socio-cultural and geographical difference.
The present study shows that younger age of children, place of delivery, lack of vaccination center near the village and educational status of mothers/caregivers were independently associated for missed opportunity for immunization when we compared with the previous study Wolikte health center age of children, were similar to this study but, experience of caretakers, knowledge of contact time and purpose of visit to health facility were independently associated factors in Wolikte health center. 4
In this study place of delivery and educational status were strongly associated. But antenatal cares were not significantly associated. Similarly, a study conducted in Siaya county referral hospital, place of delivery, educational status and antenatal care were significantly associated. 5
The present study was similar reasons for missed opportunity for immunization to the study in the Pediatric outpatient clinic in Juba teaching hospital, the reason for the missed opportunity was failure to attend antenatal care, place of delivery and lack of formal education was associated with missed opportunity for immunization. 9
In this study younger age of children, place of delivery, lack of vaccination center near the village and educational status of mothers/caregivers were independently associated for missed opportunity for immunization unlike study conducted in South Africa, Cape Town, health worker knowledge, regarding schedules and contraindications to immunization it appears that false contraindications to immunization or concerns regarding simultaneous administration of immunizations contributed to the missed opportunities. 6
The present stud like South Africa, Cape Town, Dominican Republic’s study that MOVs participants said the doctor or nurse had did not need any additional vaccine(s) and the child could not be vaccinated due to illness. False contraindications included cold/cough, mild fever, malnutrition and/or anemia, and stomach pain. Reasons associated with the caregiver were related to the belief that the child did not need vaccines or that they had already completed the immunization schedule and lack of vaccination due to vaccine stock-outs 8 were main reasons to missed opportunity for immunization but not the present study. In this study there were several additional challenges were given by mothers or caregivers for missed opportunity for routine immunization from this, mothers too busy(11.6%), vaccinator absent(11.1%), fear of side effects(8.5%), place of immunization to far(8.3%), vaccine not available (8.3%), vaccine not open for a single child(7.8%), and long vaccine time(5.2%).
Generally, missed opportunity of OPV0, BCG and measles were higher than other antigens this might be due to absence of accessibility of the vaccination for newborn at birth that delivery in health centers and BCG and measles vaccine vials that may lead vaccinators not to open for less number of children to avoid vaccine wastage.
Conclusion
The prevalence of missed opportunity for routine immunization in Gozamen district health centers was 74.9%. Home delivery, lack of vaccination center near the village, younger children (<12 months) and not attended formal education were independently associated with missed opportunities for routine immunization.
Recommendation
It might be reduced by educating mothers to deliver in health facilities and administer immunization at birth. The dose of BCG 20 doses per vial and measles antigens 10 doses per vial which is currently available at health facility should be lower doses per vial to reduce missed opportunity for routine immunization. Zonal and district health offices should supervise the whole health institution to be given routine immunization services regularly. Functional refrigerators should be addressed to all health institutions. All the health professionals should administer oral polio vaccines for all newborns that delivered at health institutions at birth and appoint the next immunization date according to the WHO schedule.
Footnotes
Acknowledgements
We would like to thank supervisors, data collectors, and study participants.
Author Contributions
All of the authors contributed equally in the design,conception, and write up of the proposal. FM collected and supervised the data. All of the authors contributed in the write of the analysis and the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.