
Abstract
Objectives. Prevention of mother-to-child HIV transmission has been globally successful leading to a decline in HIV-infected infants. Thus, the number of HIV-exposed, but uninfected, infants is increasing. As growth is an important indicator of child health, this study aimed to evaluate growth parameters of HIV-exposed Chinese infants. Methods. A prospective study was conducted among HIV-exposed (HIV-infected and uninfected) infants born during 2007 to 2015 in Liuzhou, China. Their weight and length were assessed longitudinally from birth to 18 months of age and compared with HIV-unexposed, uninfected (HUU) infants from the same region. Results. There were 467 HIV-exposed infants. Four percent of infants were HIV-infected. The mean weight-for-age (WAZ) and length-for-age (LAZ) z scores of HIV-infected infants were significantly lower than those of HIV-exposed but uninfected (HEU) infants during 9 to 18 months and 12 to 18 months of age, respectively. Additionally, the mean WAZ and LAZ scores of HIV-infected infants were significantly lower than HUU infants during the first 12 months and 18 months of life, respectively. The mean WAZ and LAZ scores of HEU infants were significantly lower than HUU infants during the first 12 months and 6 months of life, respectively. HEU infants also had a lower mean weight-for-length z score than HUU infants during the first 6 months. Conclusion. We demonstrated poor growth among HIV-exposed Chinese infants, including HIV-uninfected, compared with HUU infants. The results emphasize the need for nutritional monitoring and interventions for HIV-exposed infants regardless of HIV infection status. Research is needed on long-term growth trajectories and factors affecting growth of HIV-exposed infants in China.
Introduction
The prevalence of human immunodeficiency virus (HIV) among women of child-bearing ages has increased worldwide. 1 According to the latest information from the Joint United Nations Program on HIV/AIDS, there were 17.8 million women living with HIV in 2016, 2 and approximately 1.2 million women living with HIV give birth annually. 3 Prevention of mother-to-child HIV transmission (PMTCT) has been globally successful; there has been a 48% decline in the number new infections in infants in the highly endemic HIV regions since 2010. 4 As a result, the cumulative number of infants born to HIV-positive mothers but uninfected is expected to increase over time.
Several studies from developed and developing countries have focused on the health, particularly the growth parameters, of the HIV-exposed but uninfected (HEU) infants. A large prospective European study revealed no major differences in growth between HEU children and children in the general population from birth to 10 years of age. 5 In a multicenter cohort study in the United States, HEU children whose mothers initiated antiretroviral therapy (ART) during pregnancy had lower than average birth weight and length. However by 2 years of age, their mean weight Z score, length Z score, and weight-for-length Z score were above average. Moreover, weight-for-length Z score at 2 years of age was more than the 95th percentile in 13%. 6 In contrast, a prospective study in Uganda found that a significant proportion of HEU children were substantially below the World Health Organization (WHO) growth standards for weight and height from birth to 4 years of age. 7 In a longitudinal analysis comparing growth of HEU infants and children and HIV unexposed and uninfected (HUU) counterparts from 2 cohort studies in Zambia, the HEU group had lower weight-for-age and length-for-age during early childhood and these differences still existed when children reached school age. 8 Some authors have suggested that the growth differences between American, European, and African cohorts, and even subcohorts within Africa, of HEU infants and children compared with the HUU may be related to specific formula feeding versus breastfeeding practices, along with differences in universal maternal ART and newborn prophylaxis.9-13 In one study of Ethiopian infants, HEU infants actually had noninferior growth and higher mean weight-for-age Z score than HUU controls. 14 Thus, there appears to be conflicting results on growth in HEU children in various settings globally. Moreover, HIV-unexposed (uninfected) infants were not always included as the control group for comparison in some of these studies.
Although China remains a low-prevalence country with the national HIV prevalence rate of 0.037%, 15 HIV cases, including women of child-bearing ages, have been reported in nearly every province as of 2015. 15 The reported rate of mother-to-child HIV transmission in China was 5.7% in 2016. 15 The information on growth among HIV-exposed, either HIV-infected or uninfected, Chinese infants remain limited to date. We analyzed the cohort data of pregnant women with HIV infection and their infants who received medical care and services at Maternal and Child Health Hospital of Liuzhou (MCHHL). Our aims were to compare growth parameters between HIV-infected infants and HEU infants, and to evaluate growth differences between infants born to HIV-infected women and infants born to HUU women during the first 18 months of age in Southwestern China. We also aimed to explore demographic and socioeconomic factors that might have affected their growth trajectories.
Material and Methods
Setting
Guangxi province ranks third in the number of people living with HIV in China. 15 Liuzhou is a major city in the center of Guangxi province with a population of 3.7 million. There are approximately 100 women living with HIV giving birth annually in Liuzhou. MCHHL is the largest tertiary hospital that provides medical as well as obstetric care specifically to women, infants, and children in Liuzhou and cities nearby.
Study Population
This prospective, hospital-based study was conducted at MCHHL between January 2007 and June 2015. All infants born to HIV-infected women were entered into the study after maternal written informed consent was obtained. In this analysis, the inclusion criteria were (1) an infant surviving at least 18 months, (2) born a singleton, (3) a gestational age between 37 weeks and 42 weeks, (4) a birth weight at least 2500 g, (5) having no congenital anomalies, and (6) having at least 2 follow-up visits after birth.
The PMTCT program at MCHHL is outlined as follows: pregnant women seeking prenatal care at MCHHL were counseled to undergo a free HIV antibody test by ELISA (enzyme-linked immunosorbent assay) at the first visit. If reactive, positive samples were confirmed by western blot immunoassay (HIV/AIDS Testing Laboratory, Center for Disease Control of Liuzhou). Serial, free HIV testing was provided to initially noninfected women during the second trimester and at delivery. Syphilis and hepatitis B screening was concurrently performed in early pregnancy, in the second trimester, and at the time of delivery. Women with confirmed HIV infection received CD4 T-cell count testing and were prescribed combination ART from 14 weeks gestation onward, typically containing either zidovudine with lamivudine and lopinavir/ritonavir, or tenofovir disoproxil fumarate with lamivudine and efavirenz.
Infants born to HIV-infected mothers at MCHHL received nevirapine or zidovudine prophylaxis from birth to 4 to 6 weeks of age as well as cotrimoxazole until HIV infection was excluded. All were followed at 1, 3, 6, 9, 12, and 18 months of age. Blood samples were taken at 1 month and 3 months of age for HIV DNA-PCR (polymerase chain reaction) and at 18 months of age for HIV antibody testing (HIV/AIDS Testing Laboratory, Center for Disease Control of Liuzhou). HIV-infected infants received zidovudine or stavudine combined with lamivudine and nevirapine or efavirenz (efavirenz was only available in tablet form and given after 3 years of life). Free infant formula was recommended and provided through 18 months of age for every HIV-exposed infant. If the infant was found to have poor growth, the treating physician would offer additional advice on nutritional guidance at his/her own discretion. For those lost to follow-up, they were assigned to a physician who made phone contacts to encourage returning to care.
We utilized a cohort of HUU infants as the control group in this study. This cohort consisted of infants born from 2014 to 2016 to women with a negative HIV test during pregnancy and living in Liubai district within the city of Liuzhou. Liubai district is a national surveillance site for pediatric nutrition and health. It was selected for comparison in this study due to its high quality of health data from the same geographic location as our HIV-exposed infants with a representative economic level and appropriate population size.
Data Collection
The birth weight and length were measured using neonatal scales accurate to the nearest 10 g and 1 mm at birth. Weight and length were measured with standardized techniques at each visit. Each anthropometric parameter was measured twice and the average of 2 readings was used for data analysis. The pregnant women’s demographic and socioeconomic variables, including marital status, education, and employment, were obtained at first visit.
Statistical Analysis
Demographic variables were analyzed using descriptive statistics. Weight and length are reported as mean and standard deviation (SD). Student’s t test was used to compare weight and length differences between HIV-infected infant group and HEU group, HIV-infected group and HUU group, and HEU group and HUU group.
The Z score was estimated for each anthropometric parameter, including weight-for-age, length-for-age, and weight-for-length, which were calculated using the 2006 WHO Child Growth Standards. 16 The Z score for weight-for-age (WAZ), for example, is calculated by subtracting the mean weight of the reference population at the child’s age from the child’s weight and dividing by the SD of the weight of the reference population at that age. The Z score results are reported as mean ± SD at each age.
All values were generated using Microsoft Office Excel 2007, and the Z scores were calculated by using WHO Anthro (version 3.2.2, January 2011). Statistical analysis was performed using SPSS 23.0 software for Windows (SPSS Inc, Chicago, IL). A significance level of .05 was adopted in bivariate comparisons.
Ethical Approval and Informed Consent
This study was approved by the Liuzhou Maternal and Child Health Hospital Institutional Review Board but no reference or approval number was assigned. Women provided written informed consent for themselves and their infants prior to study entry.
Results
Maternal and Infants’ Demographic and Socioeconomic Characteristics
The total number of HIV-exposed infants was 512, but 1 set of twins, 19 premature births, and 25 low-birth-weight infants did not meet the inclusion criteria. Therefore, a total of 467 HIV-infected mother-infant pairs were included in this study. The mean age of the mothers was 28.8 (±4.7) years. The majority (70.0%) of the mothers were married, 13.6% were divorced, and 16.1% were unmarried. While 52.3% and 21.4% of the mothers completed junior and senior high school, respectively, 16.3% had received only primary school education or no formal education. Over half (58.7%) were from rural areas and nearly half (49.0%) were housewives (Table 1). Of note, there were less C-section deliveries in the HUU group as compared to the HIV-infected group and HEU group.
Demographic Characteristics of HIV-Infected Infants, HIV-Exposed Uninfected (HEU) Infants, and HIV-Unexposed, Uninfected (HUU) Infants and Their Mothers.

P1:comparison of characteristics of HIV-exposed and HUU.
P2: comparison of characteristics of HIV-infected and HEU.
Two thirds of the HIV-infected mothers were of Chinese ethnic minorities, including Zhuang, Miao, and Yao minorities, whereas the other one third were of Han (Chinese ethnic majority). Most (81.3%) have had more than one pregnancy; however, for 65.3% of them this was their first delivery. The modes of delivery were Caesarean section in 80.7% and spontaneous vaginal delivery in 19.3%. Two thirds knew they were HIV-positive before becoming pregnant, and one third were diagnosed with HIV at their first prenatal visit. Of the 467 mothers, 80 mothers (17.1%) had no antenatal care until delivery.
Among 467 HIV-exposed infants, 233 were males. Nineteen (4.1%) were infected. The reported formula feeding after 1 week postpartum was 100%. There were initially 881 HUU infants. However, 100 were excluded due to twin birth (26), prematurity (23), low-birth-weight (31), having <2 pre- or postnatal visits (8), and missing key data (12), resulting in 781 HUU infants being included in this analysis. The demographic and socioeconomic characteristics of HIV-infected infants, HEU infants, and HUU infants and their mothers are shown in Table 1.
Growth Comparison Between HIV-Infected Infants and HEU Infants
Weight-for-Age
HIV-infected infants had slightly lower mean WAZ than HEU infants at birth and the difference in WAZ between the 2 groups reached statistical significance at 9 months through 18 months of age (Table 2).
Weight-for-Age, Length-for-Age, and Weight-for-Length Z Scores in HIV-Infected Infants, HIV-Exposed but Uninfected (HEU) Infants, and HIV-Unexposed (HUU) Infants.

t1: comparing HIV-infected infants and HEU infants.
t2: comparing HEU infants and HUU infants.
t3: comparing HIV-infected infants and HUU infants.
Length-for-Age
The mean length-for-age Z score (LAZ) of HIV-infected infants was consistently lower than that of HEU infants from birth through 18 months of age. The differences between the 2 groups reached statistical significance at 1, 12, and 18 months of age (Table 2).
Weight-for-Length
There was no significant difference between the mean weight-for-length Z score (WLZ) among infected infants and those of HEU infants through 18 months of age (Table 2).
Growth Comparison Between HIV-Infected Infants and HUU Infants
Weight-for-Age
The mean WAZ of HIV-infected infants was significantly lower than that of HUU infants, respectively, from birth to 12 months (Table 2). No significant differences, however, were observed at 18 months of age.
Length-for-Age
The mean LAZ of HIV-infected infant was significantly lower than that of HUU counterparts from birth to 18 months (Table 2).
Weight-for-Length
There were no significant differences between the mean WLZ in HIV-infected infants and HUU infants at any time measured except at birth (Table 2).
Growth Comparison Between HEU Infants and HUU Infants
Weight-for-Age
The mean WAZ of HEU infants was significantly lower than that of HUU infants from birth to 12 months of age (Table 2). No significant differences were noted at 18 months of age.
Length-for-Age
The mean LAZ of HEU infants were significant lower than that of HUU infants during the first 6 months of life (Table 2). However, no significant differences were observed from 9 to 18 months of age.
Weight-for-Length
The mean WLZ was significantly lower for HEU infants than HUU infants at all ages except 9 months and 18 months of age (Table 2).
Comparison of Growth Between Male and Female Infants Born to HIV-Infected Mothers
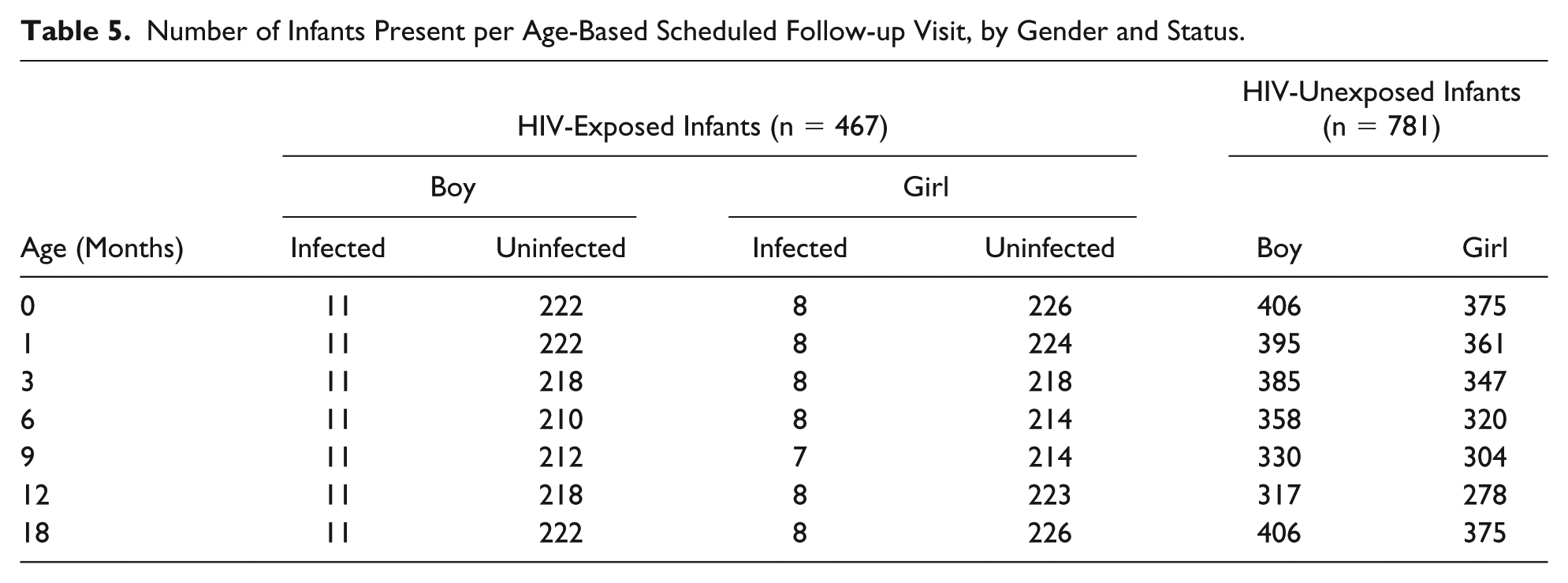
At birth, WAZ was similar between male and female infants born to HIV-infected mothers. However, male infants had significantly lower WAZ than females from 1 month through 18 months of age (Table 3). Moreover, LAZ for males was significantly lower than that for females from birth to 18 months. WLZ for males was significantly lower than that for females from 3 months to 18 months of age. Differences in males’ and females’ gender weight-for-age and length-for-age Z scores were also analyzed in the HIV-exposed (HIV-infected and HEU) infants as compared with HUU infants and summarized in Table 4. Table 5 shows the number of infants evaluated per age-based scheduled follow-up plan, per protocol, by gender, and exposure status.
Growth Parameters of Infants Born to HIV-Positive Mothers, Compared by Gender.

Growth Comparison Between HIV-Exposed Infants (HIV-Infected and HEU) and Unexposed Infants (HUU) Infants by Gender, by Z scores.

Number of Infants Present per Age-Based Scheduled Follow-up Visit, by Gender and Status.
Data on mean weight (S1) and mean length (S2) compared with the WHO and Chinese national standards are included in supplemental files (available online). Data on the incidence of wasted, malnourished, and stunted HIV-exposed compared with HIV-unexposed subjects are available in the S3 file. Risk factor analyses for wasted, malnourished, and stunted cases are included in the S4 file. Age-specific rates of wasted, malnourished, and stunted cases were low (0.2% to 1.7%) and were not significant between HIV-exposed and HIV-unexposed infants.
Discussion
We found that HIV-infected Chinese infants in Liuzhou in southwest China demonstrated poorer growth in both weight-for-age and length-for-age than HEU infants particularly from 9 months onward and at 1, 12, and 18 months, respectively. Our findings conform to some prior studies. In the European Collaborative Study evaluating more than 1500 infants born to HIV-infected women, HIV-infected infants were significantly shorter and lighter than uninfected infants with growth differences increasing with age. 5 In the US-based Women and Infants Transmission Study, HIV-infected infants had significant decrements across all standardized growth measures compared with uninfected infants from birth through 18 months of age. 17 In a large PMTCT trial in Uganda, Africa, mean growth of HIV-infected infants was significantly lower than uninfected infants for weight, height, and head circumference and such differences persisted over 5 years of follow-up. 7 A South African study concluded that HIV infection and not mere exposure was associated with low growth velocities early in life. 13 Advanced HIV disease with immunosuppression and high HIV viral load levels have been identified as significant predictors of weight growth failure.18,19 It has also been suggested that reduced dietary intake may play an important role relating to growth faltering among HIV-infected infants. 20 A study from China reported growth improvements after 24 months of antiretroviral treatment among 744 HIV-infected children (median age 6.3 years), with the changes in mean WAZ from −1.06 to −0.60 and in mean height-for-age Z score from −1.71 to −1.30. 21 Therefore, early provision of effective antiretroviral therapy, proper prophylactic measures, and prompt treatment of opportunistic complications, along with age-appropriate nutrition support and education are the keys to improve overall growth among HIV-infected infants.
Our study also demonstrates that growth of HEU Chinese infants was inferior to that of HUU infants in almost all age categories measured in regard to WAZ, LAZ, and WLZ. The exposure to maternal HIV infection not only had the adverse effect on birth weight and length, but may have also had potential deleterious effects on early growth trajectory. In a prospective study in Uganda, there was sustained lower weight and height compared with the WHO growth standards among HEU infants up to 5 years of age. 7 A cross-sectional, population-based survey from Botswana showed that HEU children <1 year and ≥2 years of age had 1.9 and 1.4 times the risk of stunting (ie, LAZ less than 2 SD) compared with HUU children. 22 However, there was no significant difference in risk of wasting (ie, WLZ less than 2 SD) or underweight (ie, WAZ less than 2 SD) for HEU versus HUU children in that study. A longitudinal analysis of 2 cohorts from Zambia indicated that, after adjusting for socioeconomic status and maternal education, HEU children had lower weight-for-age and length-for-age than HUU children and the difference persisted to school age. 8 A retrospective, cross-sectional, single-center study in the United States demonstrated significantly lower birth weight for HEU infants as compared with HUU infants. 23 A multicenter cohort study in the United States showed that HEU infants had lower than average birth weight and length; however, 13% were obese by 2 years of age. 6 In contrast, the European Collaborative Study found that HEU infants and children had normal growth pattern from birth to 10 years of age. 5 Additionally, in contrast, at 9 to 12 months of age, HEU infants had noninferior growth and attained a higher WAZ than HUU controls. 14 Finally, as noted in the introduction, numerous references have begun to suggest that the growth differences between American, European, and African cohorts, and even subcohorts within Africa, of HEU compared with HUU infants and children may be related not to simply maternal HIV exposure but to specific local formula feeding versus breastfeeding practices, along with differences in universal maternal ART and newborn prophylaxis.9-13
With the success of PMTCT, the HEU population is likely increasing worldwide necessitating specific health monitoring including growth and nutrition. Low weight and weight loss has been associated with acute malnutrition, whereas chronic malnutrition has been linked to poor length gain and inferior neurocognitive development. 13 The causes for growth faltering, if present, seen among HEU Chinese infants in our study are likely to be multifactorial. There is evidence that antiretroviral drug use during pregnancy is associated with in utero growth deficits. 24 The lower weight among HEU infants in that study was corrected during the first 6 month of life; this is also evidenced in our study as WAZ in HEU infants improved with age. A report from South Africa indicates the possibility of a transient immunodeficiency state in a group of HEU infants that led to serious infectious morbidity, and this could further affect their growth. 25 Certainly, poor maternal health and maternal nutritional status as the result of HIV infection has been shown to be associated with adverse fetal as well as early infancy growth. 26 Last, low socioeconomic status commonly seen among HIV-affected families could bear a negative impact on maternal health as well as access to care, which could ultimately impair infants’ growth. The fact that majority of HIV-infected mothers in our study had only primary or middle school education, half were not employed, and approximately two thirds were of ethnic minorities may place them at socioeconomic disadvantages. Additionally, it is concerning that 17% had no antenatal care therefore missing the opportunity to receive proper HIV care for her own health and for the prevention of HIV transmission to her infant(s). A systematic review of PMTCT programs in China indicates several levels of barriers to the prevention programs including the lack of supporting policy and multisector cooperation, the knowledge gap in HIV prevention, the lack of training among providers, discriminatory attitudes toward HIV-infected persons, and the accessibility to health care system; thus, the government’s role in multisector coordination and the acceptability and accessibility of the service are critical to the success of PMTCT in China. 27
Several limitations exist in this study. First, premature infants and low-birth-weight infants were excluded. Therefore, the growth deficits among HIV-exposed infants reported in this study could be underestimated. Second, no data on medical conditions or HIV treatment besides HIV infection status of infants and women were available. Such information may have helped explain differences in growth in the study. Third, the comparison of demographic and socioeconomic variables between HIV-infected infants and HEU infants is difficult due to the small sample size of HIV-infected infants. Fourth, the data collection of the study population and the control population (HUU mother-infant pair) was conducted through different systems and different time periods, although from the same geographic location, but may give an advantage to the control group. Moreover, we do not have the detailed infant feeding information that could significantly influence the different growth patterns. Last, the results of our study which was conducted in southwest China may not be generalizable to other regions of the country where socioeconomic settings may be different.
Conclusion
We demonstrated poor growth among HIV-exposed Chinese infants, including HIV-infected and HEU infants, compared with HUU infants. The growth deficits identified in this study emphasize the heightened vulnerability of infants born to HIV-infected Chinese women, regardless of whether the infants become infected or not. The results highlight the need for early nutritional monitoring, counseling, and long-term follow-up and support for HIV-exposed Chinese infants and their families through policy making and community-based services. Moreover, there is a critical need for early identification of HIV infection among pregnant women in China in order to initiate proper HIV care for her own health as well as for her unborn child.
JCC, DYZ, and ZN conducted the original studies and designed the follow-up study. YZ and XMH were responsible for data cleaning and wrote the first draft of the manuscript. JL collected and logged all data of this study. BW and YZ carried out the statistical analysis. EM reviewed initial statistical results and requested further analysis be completed in some areas. EM and CR critically reviewed and revised the manuscript including the re-write, and all authors were given the opportunity to complete critical review of the manuscript. CR was responsible for an initial complete re-write of the manuscript for this revision. BW also rewrote and revised the prior abstract, analysis and results sections. All authors have read and approved the final draft.
Supplemental Material
S3_TABLES_FILE_(1) – Supplemental material for Growth of HIV-Exposed Infants in Southwest China: A Comparative Study
Supplemental material, S3_TABLES_FILE_(1) for Growth of HIV-Exposed Infants in Southwest China: A Comparative Study by Ji-Chang Chen, Yu Zhang, Chokechai Rongkavilit, Bo Wang, Xue-Mei Huang, Zheng Nong, Jing Liu, Dingyuan Zeng and Eric McGrath in Global Pediatric Health
Supplemental Material
Supplemental_4_(S4)_file_of_Multivariate_analyses – Supplemental material for Growth of HIV-Exposed Infants in Southwest China: A Comparative Study
Supplemental material, Supplemental_4_(S4)_file_of_Multivariate_analyses for Growth of HIV-Exposed Infants in Southwest China: A Comparative Study by Ji-Chang Chen, Yu Zhang, Chokechai Rongkavilit, Bo Wang, Xue-Mei Huang, Zheng Nong, Jing Liu, Dingyuan Zeng and Eric McGrath in Global Pediatric Health
Footnotes
Acknowledgements
We thank all participants in the study. We are grateful to Dr Chengjuan Liu for the contribution in participants’ scheduling. We thank Dr Honghui Li, Dr Suying Liang, and Dr Qiongli Su for conducting infant physical examination.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.