
Abstract
Newborn skin nodules are usually benign and self-resolving skin condition. Differential diagnosis of such lesions include cysts, hemangioma, abscess, cellulitis, sclerema neonatorum, subcutaneous fat necrosis, neurofibromatosis, benign tumors, or malignant tumors such as rhabdomyosarcoma, infantile fibrosarcoma, or neuroblastoma. We report a case of congenital subcutaneous fat necrosis in a 7-day-old baby presenting with multiple erythematous mass on back.
Case Report
A 7-day-old term male infant presented with multiple, firm, nontender, and erythematous nodules on his back. He was born at 39 weeks gestation via spontaneous vaginal delivery. Maternal prenatal laboratory tests were negative. Maternal medications included prenatal vitamins and ferrous sulfate. The appearance, pulse, grimace, activity, and respiration (APGAR) scores were 7, 7, and 8 at 1, 5, and 10 minutes of life, respectively. Birth growth parameters were appropriate for gestational age. Newborn examination was normal except for subcutaneous nodules on back in the thoracolumber spinal region. At 2 hours of life, he was noted to have tachypnea with grunting and became febrile. So he was admitted to neonatal intensive care unit. He was started on antibiotics and was discharged from the neonatal intensive care unit on day 5 of life.
The patient’s mother reported that she was advised to monitor for “lumps” of his back, which she noticed to be progressively getting bigger since discharge. On day 7 of life, he was brought to the emergency department for evaluation of the lumps (Figure 1). In the emergency department, initial vital signs were the following: a temperature of 37.4°C, heart rate of 132 beats/min, and respiratory rate of 56 breaths/min. Initial laboratory values were as follows: white blood cells 21 900/mm3; hemoglobin 17.7 g/dL; hematocrit 49.6 g/dL; platelets 436 000/mm3 with differential of 1% bands, 41% neutrophils, 19% lymphocytes, 31% monocytes, 1% eosinophils, 1% myelocytes, and 6% metamyelocytes; D-dimer 4.36 mg/L; fibrinogen 378 mg/dL; activated partial thromboplastin time 37.2 seconds; prothrombin time 11 seconds; and international normalized ratio 1.04. Blood culture was obtained. The ultrasound of back showed 18 cm × 18 cm × 5 cm hypervascular bilobed predominantly solid mass, with several small cystic areas within it.

Lump on the back of a newborn.
Diagnosis and Hospital Course
Repeat ultrasound of the back showed long mass-like lesion in the upper back with 2 areas of cystic change and increased vascularity (Figure 2). Head and abdominal ultrasounds did not show any hemangioma or abnormalities. Due to uncertain etiology, magnetic resonance imaging of back was done and showed lobuled heterogeneously enhancing soft tissue mass in subcutaneous region of posterior aspect of distal thoracic spine without obvious spinal canal extension (Figure 3). No obvious arterial supply was noted on limited gadolinium-enhanced magnetic resonance angiogram. Since the findings on ultrasound/magnetic resonance imaging of an apparent vascular mass were not consistent with the physical examination of a firm, noncompressible mass, after getting informed written consent from parents, it was decided to biopsy and potentially excise the mass to rule out malignancy. In the operating room, the fluid-filled cavities seen on imaging were needle aspirated and opaque, and white fluid was obtained (microscopic examination showed neutrophils and macrophages). The mass itself had a yellow, curd-like portion and a gray tissue portion infiltrating the muscle. Fresh frozen section did not demonstrate malignancy, rather fibrofatty tissue with necrosis. However, because of the worrisome appearance, the entire mass was removed. Microscopic examination of the mass showed lobular panniculitis and fat necrosis with histiocytes, multinucleated giant cells, neutrophils, and scattered eosinophils, compatible with subcutaneous fat necrosis (SCFN) of newborn (Figure 4). Calcium level was within normal limit (8.8 mg/dL), and the patient was discharged home after 2 days.

Ultrasound finding of the mass.

Magnetic resonance imaging of the mass.
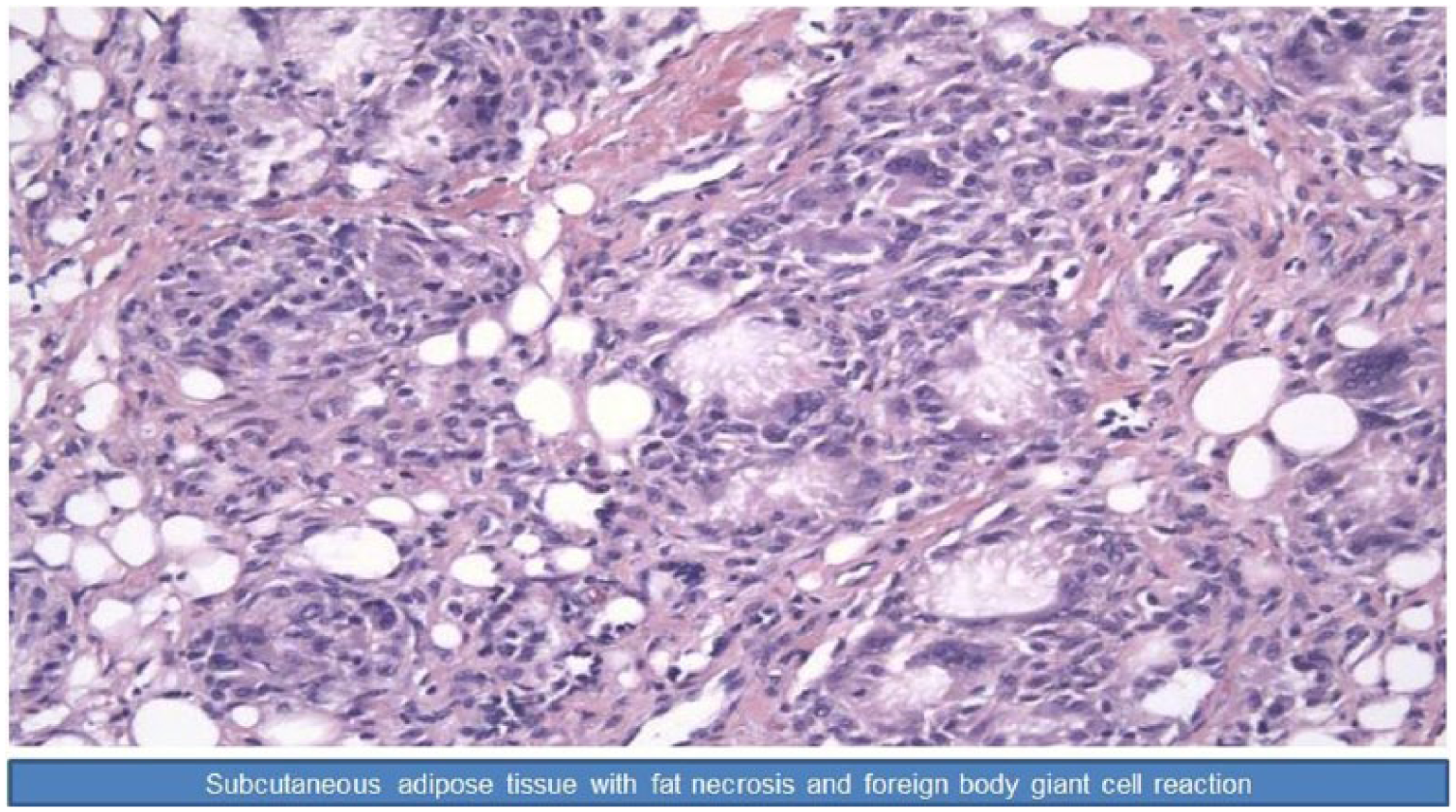
Histopathological slide of the tissue.
Discussion
Newborn skin nodules are usually benign and self-resolving. However, it is important for pediatricians to distinguish between benign condition from those that need immediate attention and subsequent close follow-ups. Therefore, it is crucial to keep a broad differential diagnosis when encountering a skin nodule in newborn. Initial differential diagnosis include cysts, hemangioma, abscess, cellulitis, sclerema neonatorum, SCFN, neurofibromatosis, benign tumors, or malignant tumors such as rhabdomyosarcoma, infantile fibrosarcoma, or neuroblastoma. In this case, the patient presented with a lesion diagnosed as congenital SCFN of the newborn.
SCFN is a rare self-limited inflammation and necrosis of adipose tissue occurring in the first few weeks of life in term or postterm infants of either gender. 1 Though its exact etiology is unknown, it has been described to be associated with maternal or birth complications, such as perinatal asphyxia, meconium aspiration, macrosomia, maternal diabetes, obstetric trauma, and therapeutic hypothermia.2-4 Acquired form of SCFN has been thought to be due to tissue necrosis and formation of granuloma secondary to poor tissue perfusion. 5 However, there are very few case reports of congenital SCFN in the literature.
SCFN can present as erythematous to purplish or yellowish, firm plaques or nodules of various sizes ranging from as small as <1 cm to as big as >10 cm. Some lesions may become cystic and fluctuant as fat liquifies.1,2 It can occur anywhere on the body but has mostly been reported on face, shoulders, buttocks, thighs, and calves. 6 Some lesions have been reported in clusters and some in single. 4 Clinical examination could suggest a diagnosis, but definitive diagnosis can only be made by biopsy. Histologically, SCFN has been reported to have a mixed of immune cells including lymphocytes, multinucleated cells, histiocytes in the background of fat necrosis, and fibrosis.4,6
SCFN usually resolves without major complications. However, a few serious sequelae have been reported, which include hypercalcemia, hypoglycemia, hypertriglyceridemia, and thrombocytopenia.1,3-5,7 Hypercalcemia, in particular, has been shown to be commonly associated with SCFN. It is proposed that granulomatous tissue in SCFN has the capacity to activate vitamin D3 as well as produce extrarenal calcitriol, both of which lead to hypercalcemia. 1 Hypercalcemia can present as lethargy, irritability, hypotonia, vomiting, and dehydration and can lead to significant complications such as nephrocalcinosis. 4 In this case, the lesion was removed surgically, and the patient was discharged home with the recommendation of calcium monitoring.
Conclusion
Congenital SCFN of newborn is a benign and self-resolving skin lesion occurring in first few weeks of life. It is usually diagnosed during clinical examination; however, definitive diagnosis can only be made by biopsy. Calcium level should be monitored in the baby as this condition could be associated with hypercalcemia.
Footnotes
Author Contributions
MSA: Contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MM: Contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AR: Contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
IB: Contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
PA: Contributed to conception and design; contributed to acquisition, analysis, or interpretation of data; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Wayne State University Institutional Review Board does not require notification or approval for publication of case reports.