
Abstract
Subcutaneous emphysema, the presence of air under the subcutaneous tissues, often arises in relation to pneumothorax, including iatrogenic pneumothorax. It can arise as a consequence of chest drain insertion and removal. This case report describes worsening of subcutaneous emphysema subsequent to chest drain removal, leading to tardive and life-threatening subcutaneous emphysema. There are few international guidelines describing chest drain removal and there are few reports describing tardive subcutaneous emphysema. These areas need further exploration using evidence-based research in order to develop a consensus on treatment options.
Introduction
Subcutaneous emphysema (SE) is caused by air entering the subcutaneous tissues. SE often arises as a result of pneumothorax, but it can also arise in relation to the transthoracic drainage of a pneumothorax, especially due to poor tube placement, anchorage, blockage, and with side-port migration into the subcutaneous tissue. 1 There are a number of reports describing the development of SE in relation to drain insertion,1–3 but few in relation to drain removal. 4
The British Thoracic Society has guidelines describing chest drain insertion; 5 however, many respiratory societies, including the American Thoracic Society, British Thoracic Society and the European Respiratory Society, do not have guidelines for chest drain removal. Guidelines for chest drain removal exist on UpToDate 6 as well as for some local hospitals. 7
The development of SE in relation to the transthoracic drainage of a pneumothorax can be immediate 3 or rapid, arising within hours; 8 however, this case report describes the tardive development of massive SE.
Case report
A 74-year-old woman, known with severe chronic obstructive pulmonary disease (COPD), was admitted in order to carry out chest drainage of an iatrogenic pneumothorax, consequent to a computed tomography (CT)-guided biopsy of a tumor-suspect pulmonary lesion. The patient subsequently developed SE and was therefore treated with applying suction to the chest drain at 10 cm H20 for a duration of 5 days.
Due to regression of SE, the absence of bubbling and oscillations in the water seal chamber as well as no signs of pneumothorax as shown on a chest x-ray (Figure 1), the chest drain was clamped and after a 3-h observation it was removed.

Chest x-ray taken prior to chest drain removal, showing no obvious signs of pneumothorax.
Five hours later, while coughing, the patient developed massive SE, involving the whole body as well as pneumomediastinum (Figure 2(a) and (b)), with dyspnea, pain, changes in the pitch of her voice and loss of vision. The patient was intubated and the lesion from the previous drain application was opened, resulting in immediate relief of the SE.
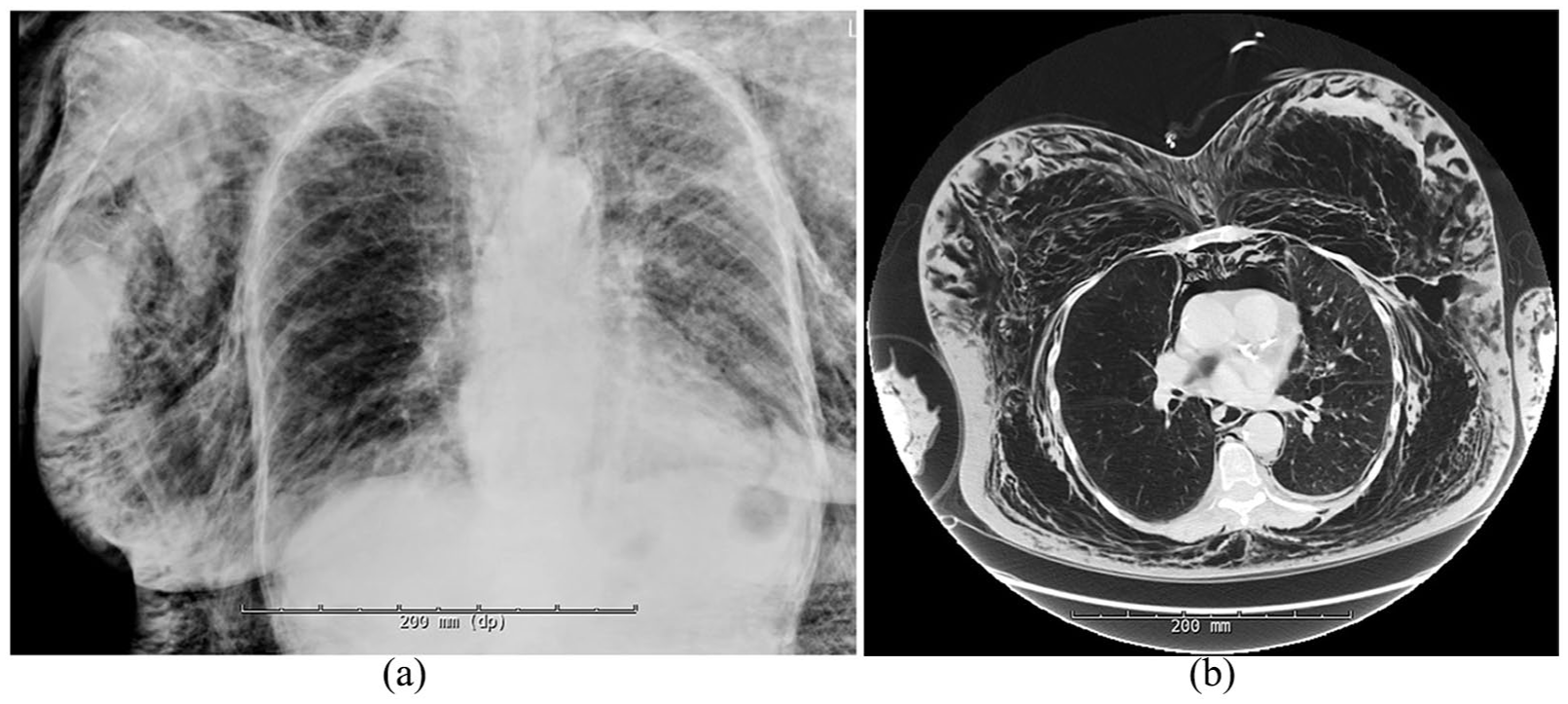
(a) Chest x-ray taken immediately prior to intubation, showing massive SE, and (b) a section of the CT-thorax scan taken immediately prior to intubation, demonstrating SE and pneumomediastinum.
Discussion
Previously, only a few articles have described the tardive development of SE. Tardive SE has for instance been described in relation to abdominal surgical procedures where SE arose after the termination of induced pneumoperitoneum,9,10 up to days after the procedure. This is different to our case, as this relates to the abdominal cavity.
The prevalence of life-threatening or fatal SE is not known, but has previously been described.11–14
As SE can be a consequence of chest drain insertion and removal, it is important that these procedures are carried out correctly. As the availability of guidelines for chest drain removal is limited, evidence-based guidelines should be sought for. This case report suggests that a consequence of not maintaining chest drainage until the complete absence of SE, both clinically and confirmed on a chest x-ray, might be the development of sudden and massive worsening of SE subsequent to chest drain removal. In this case report, the SE was in regression but had not completely resolved before removal of the drain.
According to available guidelines,6,7 the criteria for removing chest drain after a pneumothorax include taking a chest x-ray to demonstrate the lung being fully expanded, the absence of a visible air leak (cessation of bubbling and oscillation) and for no air to accumulate when suction is removed. Some clinicians clamp the chest drain, in order to identify intermittent air leaks that would not otherwise be detected; however, clamping is not universal practice as it is not always deemed as necessary. In the case of chest drainage due to a pulmonary effusion or empyema, the drain can usually be removed when daily fluid output is under 100–300 mL in the last 24 h. The threshold for removal should however be individualized depending on indication for the chest drain as well as on patient factors, such as body mass. There may be pockets of fluid remaining if the patient is clinically well, as long as antibiotic treatment is maintained as the fluid is likely to resolve without further drainage.
Conclusion
In this case report, a patient experienced an iatrogenic pneumothorax and SE subsequent to a pulmonary CT-guided biopsy. After a few days of chest drainage the SE had regressed and there were no longer signs of pneumothorax, and therefore the drain was removed. Several hours after removal, the SE worsened massively and suddenly, leading to life-threatening dyspnea and the need for intubation and a new chest drain. The patient’s symptoms resolved, and she was later discharged.
This case report suggests that a consequence of not maintaining chest drainage until the complete absence of SE, both clinically and confirmed on a chest x-ray, might be the development of sudden and massive worsening of SE subsequent to chest drain removal. In this case report, the SE was in regression, especially clinically, but had not completely resolved before removal of the drain, as shown on a chest x-ray. A recommended precaution to avoid this complication may therefore be confirming the absence of SE on a chest radiograph before drain removal.
It is both rare for SE to develop as late and as extensively as described in this case report. More case reports on tardive and massive SE could aid in the exploration of ideal management options.
This case also illustrates the importance of availability of guidelines for chest drain removal, as they are currently limited.
Footnotes
Acknowledgements
We sincerely thank our patient for the permission to write this case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. The patient has given informed consent to have the case report described for publication.