
Abstract
The falciform ligament, a peritoneal fold that anatomically separates the right and left lobes of the liver, may infrequently be a cause of patients’ complaints. In very rare instances, fatty appendages of the falciform ligament may undergo torsion, resulting in fat infarction. Despite its rarity, falciform ligament pathologies often mimic common abdominal issues, leading to misdiagnosis. Herein, we report a case of inflammation and necrosis of the falciform ligament in a 72-year-old female. The patient presented with abdominal pain, a positive Murphy’s sign, and elevated inflammatory markers. Imaging, including a computed tomography (CT) scan, was pivotal in confirming the diagnosis of falciform ligament necrosis. Contrary to the proposed surgical approach (resection of the falciform ligament) in some reported cases, conservative management (including analgesia, hydration, and antibiotics) proved successful in this case. This report emphasizes the importance of considering falciform ligament torsion in upper abdominal pain differential diagnoses and highlights the key role of imaging for accurate diagnosis.
Introduction
The falciform ligament is one of the anatomical structures that separate the left and right hepatic lobes and attach the liver to the inferior diaphragm and the anterior abdominal wall. 1 In very rare instances, fatty appendages of the falciform ligament may undergo torsion, resulting in fat infarction. This specific type of torsion or infarction, more commonly observed in epiploic appendages or the greater omentum and seldom affecting perigastric ligaments (gastrohepatic, gastrosplenic, and falciform), is collectively classified as intra-abdominal focal fat infarction (IFFI). 2 Additionally, falciform ligament necrosis may develop if embolization of the supplying artery or thrombosis of the draining vein occurs. 3
Diagnosing inflammation or necrosis of the falciform ligament is challenging given its rarity, particularly without surgical intervention and histopathologic examination of the ligament samples. It is frequently confused with other common causes of acute upper abdominal pain, such as liver and gallbladder disease. In addition to ischemia, other contributors to necrosis are tumors, cysts, iatrogenic internal hernia through the ligament, and necrotizing pancreatitis.1,4
In the literature, reports found that most cases occurred in females and presented with epigastric and right upper quadrant (RUQ) pain abdominal pain, followed by nausea as the second most common. Laboratory tests may show elevated inflammatory markers. Abdominal CT with contrast offers increased sensitivity in diagnosing and excluding other alternative diagnoses, as it reveals increased density in the fat adjacent to the falciform ligament. These images may display associated inflammatory changes and, occasionally, a “hyperattenuating rim sign” indicating potential vascular compromise. Additionally, a “central dot sign” may become apparent, representing a hyperdense focus suggestive of a thrombosed central vein. 5
Herein, we report the case of a 72-year-old female patient presenting with progressive, continuous epigastric and RUQ abdominal pain, and found to have focal necrosis of the falciform ligament, with complete recovery with conservative management.
Case presentation
A 72-year-old female patient presented with a 3-day history of progressive, continuous epigastric and RUQ abdominal pain radiating to the flanks, aggravated by eating. She also experienced multiple episodes of nausea and non-bloody vomiting. The patient’s past medical history included hypertension. She neither smoked nor consumed alcohol, and she had a history of cesarean section. The physical examination of the gastrointestinal system revealed epigastric and RUQ abdominal tenderness with a positive Murphy’s sign, and normal bowel sounds.
The electrocardiogram showed a regular sinus rhythm with an inverted T-wave in III and V3 leads. Troponin levels progressively elevated (0.017 ng/mL on presentation, 0.031 ng/mL 2 h later, and 0.056 ng/mL after 10 h), prompting referral to cardiac catheterization, which showed normal coronaries.
Laboratory-wise, amylase, lipase, alkaline phosphatase, and bilirubin levels were all within normal ranges. Aspartate aminotransferase, alanine aminotransferase, and gamma-glutamyl transferase were slightly elevated. Inflammatory markers including c-reactive protein and white blood cells (WBCs) were also elevated with predominant neutrophilia (Table 1).
Basic laboratory tests of the patient, before and after treatment.
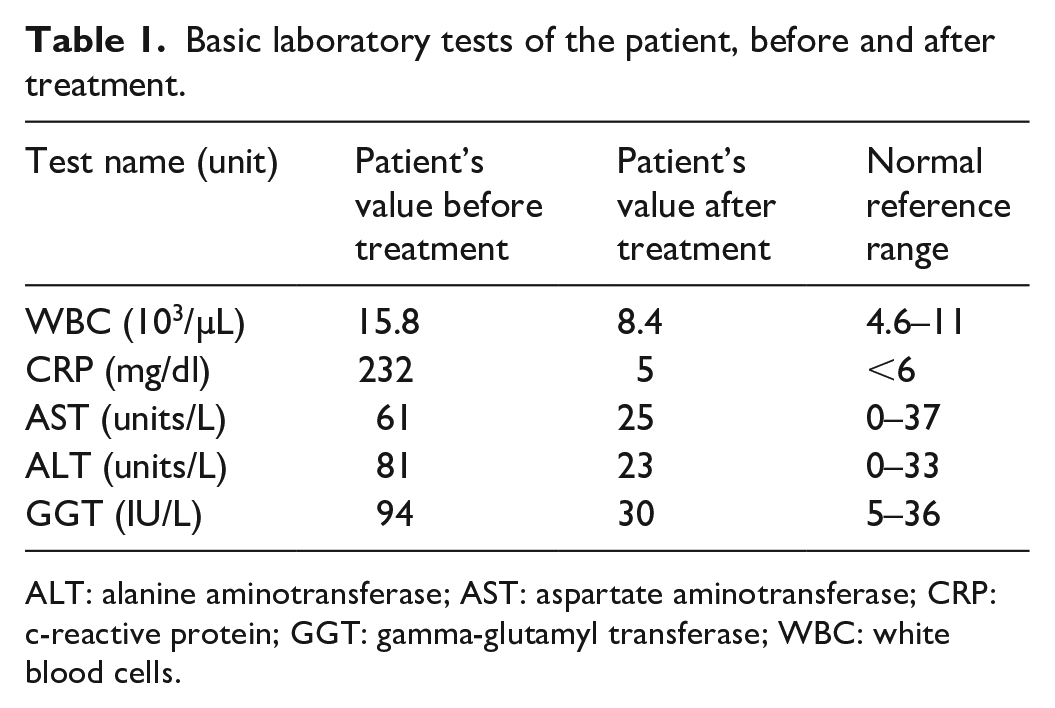
ALT: alanine aminotransferase; AST: aspartate aminotransferase; CRP: c-reactive protein; GGT: gamma-glutamyl transferase; WBC: white blood cells.
Abdominal ultrasound revealed a gallbladder with diffuse reactionary wall thickening measuring up to 9 mm with no gallstones, a thickened falciform ligament, and a normal extra and intrahepatic biliary tree. A subsequent CT scan revealed a heterogeneous hypodense mass of soft tissue in the fissure of the falciform ligament, including fat attenuation areas and inflammatory changes in the adjacent fat planes. These appearances were consistent with inflammation and necrosis of the falciform ligament with no definite abscess collection. The CT scan also showed a normal pancreas and mild enhanced reactionary wall thickening of the gallbladder with no gallstones (Figure 1).

Axial (a) and sagittal (b) computed tomographic images showing fat stranding in the falciform ligament fissure (arrows).
After a multidisciplinary team meeting with the surgical team, the plan was to manage this patient conservatively. She was prescribed adequate intravenous fluids, intravenous meropenem, paracetamol as analgesic, famotidine as stomach protection, and enoxaparin as venous thromboembolism prophylaxis. The patient progressively showed improvement in her symptoms, and normalization of her inflammatory markers, and was discharged home 5 days later in good general condition. Two weeks later, she had no symptoms, and a follow-up ultrasonography showed complete resolution of the previously found thickening of the falciform ligament.
Discussion
The falciform ligament is a thin fibrous structure composed of a double-fold peritoneum, embryonically derived from the ventral mesentery, a part of the ventral foregut. It connects the ventral abdominal wall and the liver, dividing it into the unequal right and left lobes. 1
While the falciform ligament is a scarce source of pathologies compared to other intra-abdominal structures, cases of falciform ligament hematomas, abscesses, lipomas, cysts, and tumors have been reported. 1 This article presents a case report of spontaneous necrosis and inflammation of the falciform ligament, an infrequent entity with few reported cases in the literature. Due to its rarity and proximity to more commonly diseased structures, it is almost always initially misdiagnosed as another pathology, most frequently as acute cholecystitis or cholelithiasis. 6
The physical findings in these patients further increase the likelihood of misdiagnosis; they usually present with signs and symptoms of typical gallbladder colic, including right hypochondriac and epigastric pain. Some patients, like our patient in this report, show a positive Murphy’s sign, a very sensitive sign of acute cholecystitis (sensitivity around 80%, and specificity more than 90%), 7 making it crucial to keep in mind falciform ligament necrosis even in the presence of such a specific sign for acute cholecystitis.5,8 Most patients present with nonspecific blood test results, which usually include mild elevations in inflammatory markers and WBCs.4,6
A CT scan is the gold standard for diagnosis; however, it is not uncommon to be missed, as it depends on radiologists recognizing the features of areas of fat density with focal inflammatory changes in the falciform ligament area, which helps to avoid the unnecessary need for laparotomy or laparoscopy to confirm the diagnosis as occurred in most of the reported cases.4,6 The CT scan findings in different types of IFFI (“hyperattenuating rim sign,” with or without the “central dot sign”) are nearly similar. If these findings appeared close to the colon, they raise the suspicion of epiploic appendagitis, while if they appear in the perihepatic region they prompt consideration of fatty necrosis affecting the falciform ligament. 2 On the other hand, omental infarction (another type of IFFI) appears on CT scan as a soft tissue mass anterior to the right colon. 9
Recommendations from IFFI studies suggest conservative and supportive treatment as the best initial approach unless the patient experiences a worsening clinical picture or unresolving inflammation.4,2 Our patient was successfully treated conservatively with appropriate hydration, analgesia, and antibiotics, with a close follow-up by the surgical team, and showed good clinical, laboratory, and sonographic improvement. Most cases in the literature were treated surgically, mostly due to misdiagnosis as gallbladder diseases. 6 Of the reported cases, approximately 50% of patients managed conservatively needed surgical treatment (resection of the falciform ligament through laparoscopy or laparotomy) later on due to the failure of conservative therapy or the possibility of the presence of necrosed and gangrenous tissue that had to be removed.5,2
Undoubtedly, necrosis of the falciform ligament is an uncommon pathology that can imitate various upper abdominal disorders. However, its distinctive yet nuanced characteristics on CT scans play a crucial role in facilitating early diagnosis. Given the optimum management is conservative, consideration of such a differential can avert unwarranted surgeries in such patients. 4
Conclusion
The diagnosis of falciform ligament necrosis, while uncommon, should be considered in the list of potential causes for abdominal pain. Identifying this condition can be challenging, given that its symptoms and alterations in laboratory tests closely resemble those seen in more prevalent conditions such as cholecystitis and pancreatitis. Therefore, reliance on imaging tests, especially CT scans, is imperative for a thorough analysis of differential diagnoses, including the possibility of falciform ligament necrosis, which would result in the adoption of a conservative management approach, averting unwarranted surgeries.
Footnotes
Acknowledgements
We express our deep gratitude to the medical ward staff, as well as to Dr. Ali Salman from the radiology department at our hospital, for their invaluable support in completing this report.
Author contributions
All Authors contributed equally to the report (reviewing the literature, writing the case presentation, and discussing the case information). All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was sought and obtained from the IRB board at An-Najah National University, with a reference number Med. Dec. 2023/77. A written informed consent was taken from the patient herself to publish the case anonymously.
Informed consent
A written informed consent was taken from the patient herself to publish the case anonymously.