
Abstract
Background. This prospective study was conducted to identify a suitable alternative to birth weight and establish its cutoff point to facilitate the identification of low-birth-weight (LBW) infants in Enugu, Southeast Nigeria. Methods. The study involved newborn babies within the first 48 hours of life. Five anthropometric measurements (head, chest, mid-arm and calf circumferences, as well as abdominal girth) were taken using a tape measure while supine length was measured with an aluminum infantometer. Birth weight was also recorded. Linear regression analysis was done to identify the measurement with the highest coefficient of determination with birth weight while its cutoff point was defined using a receiver operating characteristic curve. Standard statistical tests were used to determine the statistical significance of the findings. Results. The LBW prevalence for the study population was 21.41%. Chest circumference had the highest R2 value of 0.83 for the general study population and 0.72 for the LBW infants. The identified cutoff point for chest circumference is ⩽30 cm. Conclusion. Chest circumference is the best alternative to birth weight in identifying LBW babies within the first 48 hours of life in this environment.
Introduction
Low birth weight (LBW) has been defined by the World Health Organization (WHO) as “the weight at birth of less than 2500 g irrespective of gestational age.1,2 This change followed the adoption by the 29th World Health Assembly in 1976 of the new definition and thus replaced the earlier definition of 2500 g or less.3,4 This practical cutoff for international comparison is based on epidemiological observations that infants weighing less than 2500 g are approximately 20 times more likely to die than heavier babies. 4
According to the WHO, 5 the global prevalence of LBW is said to be 15.5%, which amounts to about 20.6 million LBW infants born each year, 96.5% of them in developing countries. It is a major public health problem and has long been used as an important public health indicator. Globally, the indicator is a good summary measure of a multifaceted public health problem that includes long-term maternal malnutrition, ill health, strenuous physical work, and poor pregnancy health care. It is also an important predictor of the health and survival of the newborn, but in many settings (especially where deliveries occur away from health care facilities and without a skilled attendant), many infants are not weighed at birth.4,6 Even when they are weighed at birth, it is not always measured accurately or recorded, reported, and tabulated correctly. Another problem associated with weighing at birth is the nonavailability of functional weighing scales as opined by Raymond et al 7 as well as by Arisoy and Sarman, 8 which is a part of the general paucity of medical facilities seen in resource-limited countries. Also, where available, according to the WHO Collaborative Study on Birth Weight Surrogates, 9 these scales are not sufficiently robust to withstand constant use, thus rendering them malfunctional.
In view of these constraints, several workers in various countries of the world have attempted to identify various alternative anthropometric measurements that can be used to identify LBW babies soon after delivery.10-19 In Nigeria, Ezeaka et al 20 and Olusanya 21 carried out 2 of such studies in the southwestern part, while Achebe et al 22 and Ndu et al 23 conducted similar studies in the southeast. Related studies from here had looked at the birth weights of preterm infants, 24 incidence of LBW,25-28 and birth weights of full-term newborn babies. 29 It is therefore necessary to find out a suitable alternative to birth weight and its cutoff point that can be used as a valid indicator for prompt identification of LBW babies at birth, especially where there are no functional weighing scales, which is common in resource-limited countries such as Nigeria.
Objectives
This study was carried out to identify a suitable alternative to birth weight in identifying LBW babies at birth and determine its cutoff point.
Methods
This prospective, cross-sectional, hospital-based study was conducted at the Maternity Unit, University of Nigeria Teaching Hospital, Enugu, and involved newborn babies delivered in the unit. All the babies were screened before recruitment using these 2 exclusion criteria: (1) obvious physical deformity and (2) uncertain gestational age (GA). The GA was taken to be certain if the mother recalled the date of the first day of her last menstrual period and if the calculated GA (from dates) was confirmed by physical assessment using the model proposed by Eregie. 30 A discrepancy of more than 2 weeks between the GA by both methods led to the exclusion of the baby from the study. Thus, every newborn baby who had no obvious physical deformity and whose GA was certain (using the above-mentioned criteria) was recruited. These babies were consecutively recruited until the required number was obtained.
Sample Size Determination
The sample size for this study was determined using the formula proposed by Naing 31 :

Using z = 1.96, p = 12.64% (from an earlier study in the institution by Chukwudi et al 27 ), and Δ = 5%, the calculated minimum sample size for the study population was 170 newborn babies.
Measurements
The eligible newborn babies were recruited within their first 48 hours of life.10,14,15,32 These measurements were carried out on the babies with a nonstretchable tape measuring to the nearest 0.1 cm and using standard techniques of measurements for head, chest, mid-arm, and calf circumferences, as well as abdominal girth.
Head circumference was measured with the tape placed just above the supraorbital ridges anteriorly and the maximum occipital prominence posteriorly making sure that the tape was placed at the same level on each side.8,13,19,32-35
For chest circumference, measurement was made at the level of the nipples at the end-phase of expiration as previously used by in earlier studies.9,36,37
For mid-arm circumference, the left arm was used for measurement, as in earlier studies.12,13,19,38
Calf circumference was measured as previously documented in earlier studies.16,33,38 The left leg was used for this measurement using the level of the maximum calf circumference.
The abdominal girth was measured at the level of the umbilicus at the end-phase of expiration with the baby calm and in the supine position. 39
Supine length was measured using a portable aluminum infantometer with a counter measuring to the nearest 0.1 cm.33,36-38
In line with the methodology of Figueira and Segre, 32 3 consecutive measurements were taken with the average taken as final measurement. Birth weight was measured at birth, to the nearest 50 g, with the nude infant lying on the available scale. This was carried out by the Labor Ward nursing staff on duty (who also served as research assistants and who were previously briefed prior to the study) and was duly recorded. The birth weights of 186 babies (62% of the study population) were cross-checked during examination and corresponded with the recorded birth weights. Zero adjustment of the scale was frequently done to ensure accuracy of the readings.
Data Analysis
Data analyses including linear regression analyses were done using Epi Info Version 3.5.4 package (linear regression was used to calculate the Pearson correlation coefficients (r values) and coefficients of determination (R2 values) between birth weight and each measurement, compute the regression equation for birth weight using each measurement, and construct the scatter plot/regression line of birth weight and the selected measurement. Other statistical tests such as Student’s t test and χ2 test were done to determine the statistical significance of the findings. A P value less than .05 was considered statistically significant. Nonparametric receiver operating characteristic (ROC) curve (using the method of De Long) was used to determine the optimal cutoff point with the highest ([sensitivity + specificity]/2) ratio indicating the lowest total misclassification error as previously documented.12,14,15,21,34,35
Ethical Consideration
Ethical clearance was obtained from the Health Research Ethics Committee of the University of Nigeria Teaching Hospital, Enugu. Informed parental consent was also obtained before any baby was recruited into this study.
Results
Table 1 shows the summary statistics of the study population using weight/gender as well as weight/age categories. A total of 299 babies participated in the study comprising 161 males and 138 females (male-female ratio = 1.17:1; χ2 = 0.308, P = .579). Of the total number of babies, 64 were LBW, giving a prevalence of 21.41% for the general study population. A total of 273 (91.3%) babies were examined within the first 24 hours of life (⩽24 hours) while the other 26 (8.7%) were examined after 24 hours and this was statistically significant (χ2 = 15.765, P < .0001).
Summary Statistics of the Study Population Using Weight/Gender and Weight/Age Categories.

χ2 = 15.765, P < .0001 (significant).
Figure 1 is a graphical representation of the R2 values between birth weight and each of the anthropometric measurements for both the LBW babies (upper bar) and the general study population (lower bar). Chest circumference had the highest R2 values of 0.72 and 0.83 for both groups, respectively. Others measurement are as shown in the Figure 1. Moreover, for the general study population, all the measurements had R2 values of 0.60 and above. All were statistically significant (P < .0006).

Coefficients of determination (R2 values) of the anthropometric measurements with birth weight for both low birth weight (LBW) babies (n = 64) and the general study population (n = 299).
Figure 2 shows the scatter plot/regression line of birth weight on chest circumference.
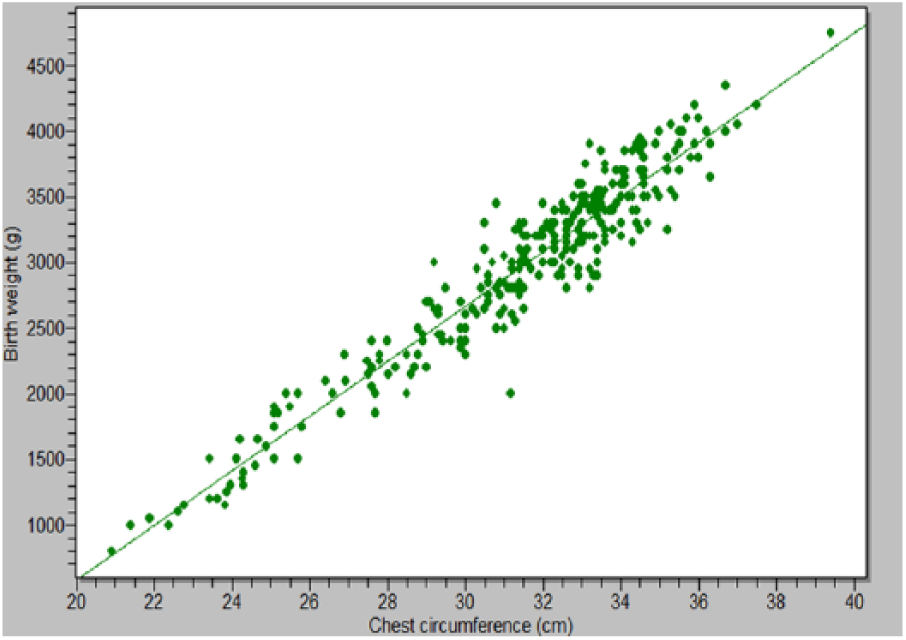
Regression line of birth weight on chest circumference for the study population (N = 299).
Figure 3 is the ROC curve for chest circumference with area under the curve of 0.992 (95% confidence interval = 0.975-0.999, z statistic = 142.708, P < .0001, and Youden index = 0.929). The optimal cutoff point is ⩽30 cm (sensitivity = 98.4% and specificity = 94.5%). Thus, this chest circumference cutoff point can be used for the identification of the LBW infant in this environment.

Receiver operating characteristic curve for identifying the optimal cutoff point for chest circumference.
Table 2 shows the validity indices of chest circumference at various serial cut-off values as indicators of LBW infants.
Validity indices of chest circumference at various serial cut-off values as indicators of LBW infants.

+PPV, positive predictive value; ++NPV, negative predictive value.
Discussion
Newborn babies within the first 48 hours of life participated in this study as reported earlier.10,14,15,32 One issue that may have likely affected our findings was the potential impact of age in view of physiological weight loss in the first 72 hours of life.40-42 In this study, babies older than 24 hours accounted for 8.7% of the general study population and this was statistically significant. This is further strengthened when viewed in light of the observation that the second day following birth appears to be one of the days of maximum weight loss.40,42 For babies within the first 24 hours of life, there was no statistically significant difference between those aged less than or equal to 12 hours and those above that age. This issue of physiological weight loss in the newborn may have informed the decision in the WHO Collaborative Study of Birth Weight Surrogates 9 to examine the newborn babies within 3 to 4 hours of life as well as the 12 hours of life used by Dhar et al. 37
Pearson’s coefficient of correlation (r value) was used in the majority of assessed studies to identify the best alternative to birth weight among the studied variables.10,13,19,21,22,32,34,35 Moreover, the WHO Collaborative Study 9 conducted in 22 countries across Asia, Africa/Middle East, Latin America, and Europe also made use of r values to compare between arm and chest circumferences in identifying the better alternative. Only the study by Achebe et al 22 had used a combination of the r value as well as the R2 value. However, in this study, the coefficient of determination, R2 value, which is a better means for evaluating the strength of a relationship, was used to identify the best alternative to birth weight. That notwithstanding, it has its own limitations (just like the coefficient of correlation) that include the fact that it does not indicate whether a regression model is adequate among others. In the present study, all the 6 anthropometric measurements were highly correlated with birth weight and this was statistically significant.
Based on the observed R2 values, chest circumference had the highest correlation with birth weight for both the general population as well as the LBW babies irrespective of the age of the baby. It is hereby recommended as the best alternative to birth weight in identifying LBW babies in this environment. This finding further reinforces the earlier recommendation of the WHO Collaborative Study 9 and other studies.8,10,12,15,16,19,23,37 Interestingly, it was also discovered that the older the baby (particularly after the first 24 hours of life), the higher the R2 value. This could be due to physiological weight loss, as it has been noted by Martin-Calama et al 40 and Noel-Weiss et al 42 that the second day of life appears to be one of the days of maximum weight loss. We could not find any other study that had looked at the effect of postnatal age on the relationship between birth weight and the anthropometric measurements.
Other studies from several countries have also recommended other anthropometric measurements as suitable alternatives to birth weight as follows: head circumference, Tawfeek 36 in Iraq; calf circumference, Gupta et al 38 and Samal and Swain, 33 both in India; mid-arm circumference, Ahmed et al 13 in Bangladesh, Sood et al 14 in India, Mohsen et al 35 in Egypt, as well as Ghosh et al 17 in Brazil. Moreover, 2 other studies from India 11 and Nepal 34 had recommended a combination of head and chest circumferences as the best surrogates of LBW infants. However, these recommendations were at variance with the outcome of this study.
A critical look at the WHO Collaborative Study 9 may tend to suggest possible racial, geographical, ethnic, or other differences accounting for the findings of that study. Three studies from Nigeria20,22,23 have tended to suggest this. The study by Ezeaka et al 20 was carried out in Lagos, a former federal capital, a cosmopolitan city in southwestern Nigeria in a population that is predominantly Yoruba-speaking. Occipitofrontal, mid-arm, and maximum thigh circumferences as well as supine length were measured. Maximum thigh circumference was identified as the best alternative indicator. The study from Nnewi, southeastern Nigeria, by Achebe et al 22 also identified maximum thigh circumference as the best indicator. The third study by Ndu et al, 23 also in southeastern Nigeria, had looked at chest circumference, occipitofrontal circumference and birth weight only. These Nigerian studies, however, did not include as many measurements as we did in this study. We wonder if their findings would have been the same if they had included the anthropometric measurements we used in this study. Moreover, we also wonder if our findings would have been any different if maximum thigh circumference was added to our list of measurements. This we think should be the subject of further research.
In this study, a cutoff point of ⩽30 cm for chest circumference was identified as the cutoff mark for the identification of LBW infants in this environment. This is also in keeping with the range of 29 and 30 cm recommended by the WHO Collaborative Study. 9 It is slightly higher than the 29.5 cm reported by Kapoor et al 12 from India. Interestingly, it is also in agreement with the following reported values from the named countries: Turkey, <30 cm by Arisoy and Sarman 8 ; Zimbabwe, 30 cm by Fawcus et al 10 ; Bangladesh, 29.5 to <30.5 cm by Dhar et al 37 ; and Nepal, <30.3 cm by Mullany et al. 15 It is lower than the 30.8 cm from Nepal by Sreeramareddy et al, 34 the 30.9 cm by Ndu et al 23 in southeastern Nigeria, as well as the <31.5 cm from India by Rustagi et al. 19
There are 3 significant findings from this study. The first is the supremacy of chest circumference over others as an alternative indicator of LBW within the first 48 hours of life. The second is that irrespective of birth weight or postnatal age, chest circumference still had the highest R2 value. A number of reasons have been adduced to explain this reported supremacy of chest circumference. These include the following: chest circumference could be more easily and reliably measured9,15; identification of the nipple line is easier, making measurement more operationally feasible 9 and replicable. 37 Chest circumference has a larger cross-section with less chance of systematic or random errors in measurement. 43 The third significant finding is the fact that a very simple tool—a tape measure, which is widely available—is all that is required for this measurement. Thus, this can serve as a very useful tool in the hands of primary health care workers for improving the detection of LBW, and therefore, “at-risk” infants, delivered not only at home but also in facilities without functional weighing scales. A color-coded tape would definitely be a very useful tool at the community level for the identification of this subset of newborn babies.
In many situations, a good number of babies are born outside health facilities and are not seen by community health workers until a few days after delivery. It would be interesting to know whether the relationship between birth weight and chest circumference remains the same after the first or second week of life by which time most of these babies would have regained their birth weights or even surpassed them as argued by Martin-Calama et al 40 and Noel-Weiss et al. 42 Unfortunately, we were not able to address this and further research is of absolute necessity.
This study was done in Enugu, southeastern Nigeria, and one important question that we could not answer was whether this cutoff point can apply to babies born in other parts of the southeast. Further research is thus needed in this area particularly of a multicenter and collaborative nature. Another limitation of this study was the noninclusion of anthropometric measurements like maximum thigh circumference and foot length. The use of a weighing scale that measures to the nearest 50 g would have made our figures not precise enough for a good estimate of the relationship between birth weight and the anthropometric measurements to be made. Finally, this study included babies aged over 24 hours with the possibility of physiological weight loss affecting the outcome. Interestingly, there is an ongoing study in 6 tertiary centers in the 5 southeastern states that includes foot length and maximum thigh circumference among other measurements.
Conclusion
Chest circumference is the most appropriate alternative to birth weight in the identification of LBW infants in this environment. The identified cutoff point of ⩽30 cm is hereby recommended for use in Enugu, southeastern Nigeria.
Footnotes
Author Contributions
NKC: studied conception and design; data acquisition, analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval and accountable for all aspects of the study.
HIN: studied conception and design; data analysis and interpretation; critically revised manuscript; gave final approval and accountable for all aspects of the study.
GNA: studied conception and design; data analysis and interpretation; critically revised manuscript; gave final approval and accountable for all aspects of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.