
Abstract
To examine gaps in communication versus documentation of weight-management clinical practices, communication was recorded during primary care visits with 6- to 12-year-old overweight/obese Latino children. Communication/documentation content was coded by 3 reviewers using communication transcripts and health-record documentation. Discrepancies in communication/documentation content codes were resolved through consensus. Bivariate/multivariable analyses examined factors associated with discrepancies in benchmark communication/documentation. Benchmarks were neither communicated nor documented in up to 42% of visits, and communicated but not documented or documented but not communicated in up to 20% of visits. Lowest benchmark performance rates were for laboratory studies (35%) and nutrition/weight-management referrals (42%). In multivariable analysis, overweight (vs obesity) was associated with 1.6 more discrepancies in communication versus documentation (P = .03). Many weight-management benchmarks are not met, not documented, or performed without being communicated. Enhanced communication with families and documentation in health records may promote lifestyle changes in overweight children and higher quality care for overweight children in primary care.
Childhood overweight and obesity are pervasive and costly public health problems. 1 Pediatric primary care is an important opportunity to assess and treat these conditions, because school-age children are seen regularly in primary care. 2 Current primary care screening and weight-management strategies, established by Expert Committee guidelines and systematic reviews, have been distilled by the American Academy of Pediatrics Bright Futures Program into a set of specific clinical practices considered to be “benchmarks” of high-quality weight management.3-5 Many of these benchmarks are included in the 2016 Healthcare Effectiveness Data and Information Set (HEDIS) as nationally standardized performance measures to improve the quality of primary care obesity screening and weight-management counseling practices. 6 Performance of weight-management benchmarks, particularly the HEDIS measures, often is determined by chart review; however, it is unclear whether differences exist between provider-parent/patient communication during visits and associated documentation in the electronic medical record (EMR).
Weight-status improvement may be achieved by provider recognition that a child is overweight with performance of weight-management benchmarks (as evidenced by either communication or EMR documentation), education of the patient and family (via communication with or without EMR documentation), or both. Benchmarks that are identified and/or documented by providers, but not communicated to patients and families, may be missed opportunities for communication regarding health risks associated with unhealthy weight status, such as risk for diabetes when acanthosis is identified on physical examination. Such communication may educate and activate parents’ and patients’ own intrinsic motivations to adopt healthy behaviors.7,8 Discrepancies in communication versus documentation—including communication without documentation or vice versa—may affect analyses of quality of care and the association of weight-management benchmarks with weight-status improvement.
The study aims, therefore, were to examine communication and documentation of weight-management benchmarks during primary care visits with overweight and obese Latino children and to determine the frequency of and factors associated with discrepancies in weight-management benchmark communication versus documentation.
Methods
The study design was a cross-sectional analysis of video-/audio-recorded primary care visits and associated health-record documentation in 2 EMR systems (EPIC and NexGen). A convenience sample of providers, participants, and parents was recruited from 2 clinics in Dallas, TX: an academic resident continuity clinic that uses an EPIC EMR and a community-based clinic that uses a NexGen EMR. Participants were recruited from May to October 2012.
Potential subjects were asked to participate in a study to examine provider-patient communication regarding preventive health topics (to mask the study focus on communication about weight). Written informed consent was obtained from providers and parents, written assent from 10- to 12-year-old participants, and verbal assent from 6- to 9-year-old children. The study protocol was approved by the Institutional Review Board at the University of Texas Southwestern Medical Center.
Eligibility criteria for participants were child age between 6 and 12 years; overweight, with a directly measured body mass index (BMI) of ≥85th percentile for age and gender; parental English or Spanish proficiency (measured using standard US Census Bureau questions on the participant’s self-rated ability to speak English) 9 ; and Latino race/ethnicity by parent self-identification, because the parent study’s primary objective was to examine provider communication with overweight Latino children and their families to determine whether differences exist in communication between language-congruent and language-incongruent parent-provider interactions. 10 For providers at the academic center, resident/attending dyads were recruited; at the community-based clinic, only attending providers were recruited. Providers completed surveys without assistance. For participants, English and Spanish surveys were verbally administered by trained, bilingual research staff.
Previsit surveys assessed sociodemographic characteristics of the child, parent, and provider. Sociodemographic characteristics assessed for the child included age and gender (all children were Latino by study design). Parental characteristics assessed included age, parental weight and height (by parent self-report), highest educational attainment of adults in the household, and annual household income. Provider characteristics, assessed by self-report, included gender, race/ethnicity, height, and weight (asked with a series of other questions to mask the study’s focus on weight).
Child BMI was calculated using weights and heights measured in the clinic by trained clinical staff via standardized clinical protocols and calibrated instruments. BMI percentiles for age and gender were determined using Centers for Disease Control and Prevention growth charts, and BMI percentile categories were defined using American Academy of Pediatrics–recommended cut-points.3,11 Parent and provider weight status were determined using self-reported weights and heights from previsit surveys. Healthy weight, overweight, and obesity for parents and providers were defined using BMI cut-points of 18.5 to <25, ≥25 to <30, and ≥30 kg/m2, respectively. 12
Visits were recorded using digital video- and audio-recorders placed in discreet locations in examination rooms by research staff prior to visits. All recorded visits were viewed (or listened to, for audio-tapes), professionally transcribed, and analyzed by 3 independent observers. For visits conducted in Spanish, visit transcripts were transcribed twice from Spanish to English by a bilingual medical student and a bilingual research assistant both trained in medical Spanish; discrepancies in Spanish-English interpretation were resolved by consensus.
A data-extraction form was created that specified criteria needed for presence of communication and EMR documentation of 5 weight-management content areas recommended by Bright Futures and the American Academy of Pediatrics (Table 1).3,5 Communication criteria were published previously (as supplemental material). 10 Briefly, criteria for presence of benchmark communication and documentation included the following:
Provider determines/interprets child’s BMI-for-age, determined by direct communication by the provider that the child was overweight and by documentation in the health record of a visit-related ICD-9 code for overweight, obesity, or abnormal weight gain (in the assessment/plan, problem list, medical history, or billing codes).
Provider performs a comprehensive physical assessment, determined by communication and/or documentation (in the visit note, problem list, medical history, or visit-billing codes) regarding the presence or absence of a weight-related physical-exam finding (see Table 1).
Provider identifies whether high weight status is accompanied by another disorder, determined by the following:
a) Provider and patient/family communicate regarding family history or provider documents family history in the visit note (eg, family history had to have been imported into or documented within the visit note, and historical documentation of family history without evidence that it was reviewed on the day of the visit was not considered as documentation of family history). or b) Provider recommends or communicates regarding weight-related laboratory studies and/or documents results, interpretation of results, or plan to obtain studies in either the visit note or visit-associated orders. or c) Provider identifies high blood pressure (defined as a systolic or diastolic blood pressure ≥90th percentile [the cut-point for prehypertension], determined using formulae and regression coefficients found in Appendix B of The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents
13
), because blood pressure is obtained at every visit and the blood pressure percentile for age, gender, and height could be calculated reliably.
Provider sets a treatment goal, determined by the presence of communication and/or documentation of discussion of 4 items:
d) Screen-use behavior (eg, time spent using TV, videos, video games, computers, tablets, cell phones, etc) e) Physical activity f) Dietary changes g) A goal for weight maintenance or loss
Provider communicates and/or documents a plan for long-term maintenance of the treatment program, determined in 2 ways: h) Referral to nutrition/weight management recommended and/or documented in either the visit note or orders associated with the visit i) Recommended and/or scheduled an interval doctor’s visit to readdress weight
Methodology Used to Determine Weight-Management Benchmark Communication and Documentation.
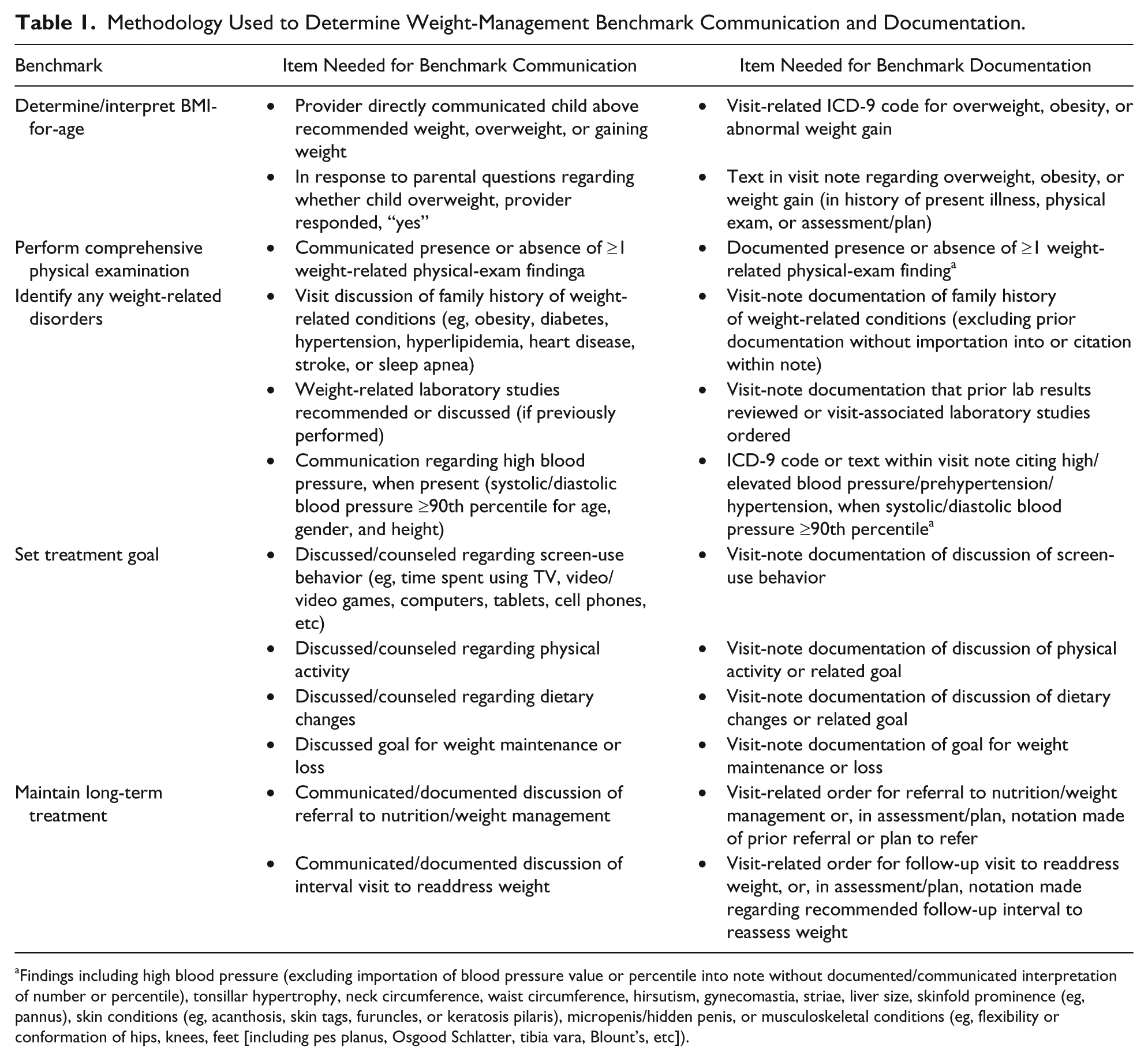
Findings including high blood pressure (excluding importation of blood pressure value or percentile into note without documented/communicated interpretation of number or percentile), tonsillar hypertrophy, neck circumference, waist circumference, hirsutism, gynecomastia, striae, liver size, skinfold prominence (eg, pannus), skin conditions (eg, acanthosis, skin tags, furuncles, or keratosis pilaris), micropenis/hidden penis, or musculoskeletal conditions (eg, flexibility or conformation of hips, knees, feet [including pes planus, Osgood Schlatter, tibia vara, Blount’s, etc]).
Three independent reviewers completed data-extraction forms for all visits, first, using the visit recordings and transcripts, and then, by extracting the corresponding items (described above) from the EMR. Average pairwise coder agreement was excellent (85% to 100%), and kappa scores (calculated using SAS Macro MAGREE) ranged from 0.7 (for documentation of family history) to 1.0 (for communication regarding dietary and physical activity changes).
Descriptive statistics were used to summarize sample characteristics, and for each recommended weight-management content area, the frequency of communication, documentation, communication without documentation, documentation without communication, both communication and documentation, and neither communication nor documentation. Then, for each visit, the number of discrepancies between communication and documentation (either communicated, but not documented, or documented but not communicated) was summed (each visit could have up to 10 discrepancies) and the mean number of discrepancies by provider and child characteristics were calculated. Bivariate and multivariable analyses were used to examine factors associated with discrepancies between communication and documentation of weight-management benchmarks. Covariates were selected using backward-stepwise regression and an alpha-to-stay of <.15. Analyses were conducted using SAS version 9.2 (SAS Institute, Cary, NC).
Results
For children (n = 26), the mean age was 9.5 years old, over half were female, and one fifth were overweight (Table 2). For parents, the mean age was about 37 years, most were overweight or obese, 62% had limited English proficiency, and almost 60% were not high school graduates. For providers (N = 15), almost three quarters were female, 13% were African American, one third were Asian, and 13% were Latino; about one quarter were Spanish proficient, 40% were overweight or obese, half graduated medical school more than 6.5 years prior to the study (the sample’s median time since medical school graduation), equal proportions practiced at academic/hospital-based and community clinics, and approximately half of visits were conducted in English versus Spanish.
Participant Characteristics.

Abbreviations: GED, General Educational Development; IQR, interquartile range.
Benchmarks were both communicated and documented 31% to 85% of the time, communicated but not documented 4% to 19% of the time, and documented but not communicated 0% to 31% of the time (Figure 1). The frequency of benchmarks being neither communicated nor documented (represented in the figure as the area remaining to the right of each benchmark) ranged from 0% (eg, all dietary changes were either communicated, documented, or both communicated and documented) to as high as 35% (for weight-related laboratory studies) and 42% (for referrals to nutrition/weight management). Among children with obesity, for whom lab studies and referrals would be indicated 3, 5, lab studies and referrals were performed 71% and 62% of the time, respectively (vs 40% for both in overweight children). Notably, the HEDIS billing/quality measures that are determined by chart review, “determine/interpret BMI-for-age” and “discuss diet and physical-activity changes,” were communicated but not documented 12% to 15% of the time. The frequency that a benchmark was documented but not communicated to the patient ranged from 0% for discussion of physical activity and dietary changes up to ~30% for presence/absence of an abnormal physical-exam finding and family history. Notably, in 1 in 5 visits, providers documented a child’s goal for weight maintenance or loss without communicating the goal to the family.

Proportion of visits in which weight-management benchmarks were both communicated and documented, communicated but not documented, and documented but not communicated.
In the bivariate and multivariable analysis of discrepancies in communication versus documentation of weight-management benchmarks (when either communication or documentation of benchmarks but not both occurred) the total number of discrepancies per visit ranged from 0 to 7, with a mean of 2.4 (SD ±1.6) discrepancies (data not shown). Discrepancies did not differ by child (gender, race/ethnicity, or age), parent (educational attainment), provider (weight status), or visit (language in which visit was conducted) characteristics in both bivariate and stratified analyses. In the multivariable analysis, only children who were overweight (vs obese) were more likely to have a greater number of discrepancies in communication versus documentation of weight-management benchmarks. On average, visits with an overweight child, compared to those with an obese child, had 1.6 additional discrepancies between communication and documentation, after adjustment for other factors (including child gender; parental English proficiency and age; provider weight status, race/ethnicity, and years since medical school graduation; language in which the visit was conducted; and clinic site).
Discussion
This is the first study, to our knowledge, to examine the relationship between directly observed provider-patient communication regarding weight-management benchmarks and associated EMR documentation. A novel study finding is that many benchmarks of quality weight-management care are not met during primary care visits with overweight Latino children—particularly, referrals to nutrition/weight management and performance of recommended laboratory studies. Although the study was not designed to identify the reasons for failure to achieve benchmarks, there are several potential explanations. Providers may not always recognize that a child with a BMI-for-age ≥85th percentile is overweight. 14 For those who recognize that a child is overweight, studies suggest that some providers may believe that there is little that can be done in primary care to improve the child’s weight status.15,16 Alternatively, the provider previously may have addressed weight management with the family. Lack of incentives or financial reimbursement also could play a role—notably, the benchmarks with the highest rates of performance were the HEDIS measures that are used by health insurance companies to determine quality and billing. 6 Finally, certain benchmarks (eg, weight-related laboratory studies and referrals to nutrition or weight management) may not have been indicated for children who are overweight (but not obese) without risk factors or comorbidities. 3
Importantly, study data suggest that many benchmarks are documented without being communicated—notably, weight-related physical-examination findings, family history, and goals for weight maintenance or loss. For clinicians, these findings are important because improved communication with patients and families about these benchmarks might affect their motivation to make healthy lifestyle changes.7,8 For researchers and quality specialists, the findings indicate that benchmark documentation may not be a valid indicator of provider communication with patients/families. Possible reasons why objective items, such as physical-examination findings and family history, might not be communicated include time constraints, 17 identification of an abnormal vital sign (such as high blood pressure) during EMR documentation after a patient has left, or importation into the EMR of family history items that were collected and documented at a prior visit and not discussed during the visit recorded in this study. Less clear is why goals for weight maintenance or loss would be documented without being communicated. Perhaps EMR-based “smart” phrases might promote benchmark documentation without communication if, for example, the assessment/plan automatically populates when specific diagnoses are entered (eg, selecting an ICD-9 code for obesity leads to population of a plan such as “recommended weight loss or weight maintenance”). Further qualitative studies are needed to better understand where and why discrepancies exist in both documenting and communicating weight-management benchmarks.
Data also suggest that many benchmarks are communicated but not documented—especially the HEDIS measures. This finding has important implications when using EMR documentation for quality improvement, particularly if benchmark communication proves to be associated with weight-status improvement or other outcomes. For example, in secondary data analyses (using documentation as a proxy for communication), the impact on outcomes of benchmarks that are communicated but not documented would be underestimated. Thus, providers may want to pay particular attention to both communicating and documenting weight-management benchmarks, and health services researchers should note that benchmarks may be documented less frequently than they are communicated.
Certain study limitations should be noted. All participants were Latino, because the parent study’s primary objective was to examine communication by language congruency. 10 Participants also had relatively lower educational attainment and were recruited from urban community and academic clinics in Dallas, Texas. Thus, study findings may not generalize to non-Latinos, populations with higher parental educational attainment, private practices, or other regions of the country. The sample size was relatively small, which may account for the lack of statistical significance in children with overweight versus obesity who received lab studies and referrals to nutrition/weight management despite larger-magnitude differences; the focus of the study, however, was on describing specific discrepancies in directly recorded communication content and corresponding EMR documentation, because this has not been previously studied. It is not clear whether weight-management quality benchmarks are associated with prospective weight-status improvement; however, this is the aim of a prospective communication study that currently is underway.
The study has several noteworthy strengths. It is the first to use video-/audio-recordings to directly observe communication of weight-management benchmarks during primary care visits and compare it to corresponding EMR documentation. In conducting the study, specific methods to define and determine benchmark communication and EMR documentation were developed and tested for interrater reliability; these methods can be used prospectively to examine the impact of recommended weight-management clinical practices on weight-status improvement of overweight children. The sample included Latino participants (with and without limited English proficiency) and parents from low-income, low-educational-attainment households. High proportions of children from households such as these are disproportionately affected by overweight/obesity.18,19
Conclusion
The study findings suggest that, during primary care visits with overweight Latino children, many benchmarks of quality weight-management care are not met; are communicated, but not documented; or are achieved without being communicated, especially for overweight (vs obese) children. Improved communication with families regarding healthy weight status and weight-related health risks could help promote healthy lifestyle changes in overweight children. Enhanced communication and documentation of quality benchmarks for weight management might prove useful in achieving higher quality in the care of overweight children in primary care.
Author Contributions
CBT: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SEB: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SM: Contributed to conception and design; contributed to acquisition and analysis; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
GF: Contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors, and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute, the National Institutes of Health, or the Agency for Healthcare Research and Quality, the funding agencies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported in part by Award # K23HL118152 from the National Heart, Lung, and Blood Institute (to Dr Turer), Award # UL1TR001105 from the National Center for Advancing Translational Sciences of the National Institutes of Health, and Award #R24HS022418 from the Agency for Healthcare Research and Quality.