
Abstract
Background:
Essential newborn care (ENC) encompasses a range of evidence-based interventions aimed at improving neonatal health outcomes and reducing mortality. Despite global efforts to improve neonatal survival, newborn deaths still account for approximately half of all under-five mortality cases, especially in low-resource settings. Adherence to recommended infant care practices remains a difficulty, contributing to avoidable neonatal mortality. In Ethiopia, newborn mortality is a serious public health issue, with an estimated rate of 33 fatalities for every 1000 live births. Therefore, this study seeks to assess essential newborn care practices and their associated factors among postpartum mothers in Tembaro Zone, Southern Ethiopia.
Methods:
A community-based cross-sectional study was conducted in, involving 390 postnatal mothers. Participants were selected using multistage simple random sampling. Data were entered into EpiData version 3.1 and exported to STATA version 16.0 for analysis. We performed binary and multiple logistic regression analysis to find factors related to the outcome variable. To determine the presence of association, an adjusted odd ratio was generated along with its 95% confidence interval. A P-value of less than .05 was used to indicate statistically significant.
Results:
The overall practice of essential newborn care was 57.7% (95% CI: 52.6-62.6). Significant factors of ENC included maternal educational status (AOR = 3.2; 95% CI: 1.45-6.98), absence of home visits by health extension workers (AOR = 0.32; 95% CI: 0.19-0.54), having 2 or fewer live births (AOR = 0.34; 95% CI: 0.20-0.57), lack of antenatal care visits (AOR = 0.48; 95% CI: 0.28-0.81), and insufficient knowledge (AOR = 0.24; 95% CI: 0.12-0.48).
Conclusion:
Approximately half of postnatal mothers practiced essential newborn care. The absence of health extension worker visits, having 2 or fewer live births, lack of antenatal care visits, and insufficient knowledge were negatively associated with essential newborn care practices. Conversely, educational level was positively correlated with essential newborn care practices.
Keywords
Introduction
Essential newborn care (ENC) is a strategic approach to improving the health of newborns through interventions before, during, and after pregnancy, immediately after birth, and during the postnatal period. Enhanced newborn care practices, particularly during the early neonatal period, are critical in reducing neonatal mortality rates.1,2 It’s vital for all newborns, regardless of their birth location or size. Globally, approximately 2.4 million newborns die within the first 28 days of life, and an additional 3 million are stillborn each year. Every minute, 11 newborns die before their fifth birthday. Sub-Saharan Africa accounts for approximately 90% of neonatal deaths (27 deaths per 1000 live births [LBs] in 2017), with approximately half of these deaths occurring at home. 3 Neonatal mortality accounts for approximately two-thirds of all infant mortality and 33% of the deaths of children aged less than 5 years.4,5 Ethiopia also faces a significant neonatal mortality burden, with a reported rate of 48 per 1000 live births 6
The high death and morbidity rates among newborns are attributed to improper the community practices that now exist throughout the region among home-delivered women. 7 Studies in several African countries, including Uganda, Ghana, and Cameroon, indicate that newborn care practices are often inadequate, contributing to high neonatal mortality rates. Common practices such as applying substances to the umbilical cord and early bathing may pose health risks. 8 Similar suboptimal practices are observed across Sub-Saharan Africa. 9 In Ethiopia, 92% of mothers who had a live birth in the past 5 years did not receive postnatal care. Only 7% of women received postnatal care within the recommended 3 days. 10
The predominant cause of neonatal mortality in developing countries is related to conditions of labor, intra-partum, and poor immediate newborn child care practices. 11 According to various studies, several variables have been identified as factors influencing newborn care practices, including maternal occupation, educational attainment, socioeconomic status, home-to-home visits by health extension workers (HEW), maternal knowledge of newborn care, antenatal care (ANC) visits, and place of delivery. 12 Ethiopia is among the Sub-Saharan countries where neonatal care practices are considered substandard or inadequate. 13 The majority of neonatal deaths take place at home and are regularly not documented. Due to a lack of postnatal health care and traditional practices such as delayed breastfeeding initiation, early bathing, and improper cord care contributed to high newborn mortality rates. 14
Although standard newborn care practices are well-established and widely promoted, there is limited data on the prevalence and factors of essential newborn care practices in Ethiopia. Therefore this study aimed to assess magnitude of essential new born care practices and identify key factors affecting the implementation of essential newborn care practices among postnatal mothers in the Kembata Tembaro zone.
Methods
Study Setting, Period, and Design
A community-based cross-sectional study was conducted in Kembata Tembaro zone between May to June 2022. The Kembata Tembaro zone is one of the administrative zones in South Ethiopia. Tembaro district is one of a districts found in Kembata Tembaro zone, which is located in SNNPR, and its administrative town is Mudulla. It has 21 rural and 3 urban kebeles. It is found 320 km South of Addis Ababa, the capital of Ethiopia. There are 1 primary hospital, 4 health centers (HC), and 22 health posts serving the total population in the district. The study was conducted in selected 9 kebeles of Tembaro district. The lists of selected kebeles has shown in sampling procedure.
Population
Source Population
All postnatal mothers of newborn age less than or equal to 42 days after delivery in Tembaro district.
Study Population
The study population comprised postnatal mothers with newborns aged 42 days or less, selected from the designated Kebeles during the data collection period.
Eligibility Criteria
Postnatal mothers with an alive newborn within 42 days after delivery before study period and residents for at least 6 months in the study area was included in this study. Those mothers who did not able to communicate with the interviewer, seriously ill, and mothers who delivered a baby died before the data collection period were excluded.
Sample Size Determination
The sample size for the study was calculated using a single population proportion formula with the assumptions of 95% confidence interval, 5% of marginal error and considering 40.7% mothers had good essential new born care practices from related study done in Enderta, Northen Ethiopia 15 and adding 10% non-response rate, a total of 408 study participants were estimated for this study.
Accordingly to the sample size calculation the result is 408. Since, the source population (N) is less than 10,000 we used finite population correction formula:


So finally, a total of 390 study participants were used for this study.
Sampling Procedure
A survey was conducted among 390 postnatal mothers with newborns aged 42 days or less, from randomly selected kebeles in the Tembaro Zone. A multistage sampling technique was employed to select the study participants. To obtain the required sample from 9 selected Kebeles, all postnatal women who had given birth within 42 days of the study period were registered to establish a sampling frame. This sampling frame was then used to list the study units within the health posts of the selected Kebeles. The total determined sample size was proportionally allocated based on the population size of each Kebele. Finally, a simple random sampling method was employed to select the participants. In households with more than 1 eligible respondent, 1 was randomly chosen using the lottery method (Figure 1).

Schematic presentation of sampling procedure.
Data Collection Tools and Procedure
The questionnaire was first developed in English and subsequently translated into Ahmaric to improve comprehension for both data collectors and responders. A pre-tested, structured questionnaire was used to collect data. The tool was developed after an exhaustive review of relevant literature.16 -18 The questionnaire included sections on socio-demographic characteristics, health service utilization (such as antenatal care, delivery, and essential newborn care), postnatal care for both mother and newborn, and the mother’s knowledge of newborn care and neonatal danger signs.
Study Variables
The dependent variable was newborn care practices. The independent variables included the following:
Operational and Term Definitions
Those mothers who reported 4 and above out of 6 of mentioned practices were categorized as “
With regard to knowledge related to neonatal danger signs, those mothers who identified at least 4 and above among the 6 listed danger signs categorized as good knowledge on neonatal danger sign and for those who mentioned 3 or less of danger signs categorized as poor /knowledge on neonatal danger sign. 19
Data Quality Control
To ensure uniformity, the questionnaire was translated back into English by a bilingual professional. Finally, the Ahmaric version was employed for gather data. Two days of training were given to supervisors and data collectors on data collection methods, participant approaches, ethical concerns, data quality, and the benefit of gathering real data, as well as their roles and duties as supervisors and data collectors. A pretest of the questionnaire was also conducted. Data collectors conducted a pre-test on 5% of the overall sample size outside of the study’s selected kebeles, which shared the same socio-demographic characteristics as the selected kebeles. Cronbach’s alpha was checked for questionnaires, and the value was .75. The data was reviewed for consistency, clarity, and accuracy before being entered into the software. Proper coding and categorization were maintained to ensure data quality. Additionally, double data entry was performed to validate the data and ensure consistency with the original entries. Cross-questions and pretest questions were utilized to reduce bias.
Data Analysis and Processing
After coding, updating, cleaning, and entering the data into Epi Data version 3.1, it was exported to STATA Version 16 for analysis. Binary logistic regression was used to evaluate the relationship between each independent variable and the outcome variable. Model fitness was assessed using the Hosmer–Lemeshow goodness-of-fit test. All variables with a P-value of less than .25 in the bivariate analysis were included in the final multivariable analysis to control for potential confounders. A variance inflation factor (VIF) greater than 10 was considered evidence of multicollinearity. Statistical significance was determined by a P-value of less than .05, with a 95% confidence interval.
Ethical Approval and Consent to Participate
The study was approved by the Ethics Review Committee (Ref no: ERC/670/2022) School of graduate Study, Wachemo University, Ethiopia. The informed consent with a written signature was obtained upon the agreement from participants after purpose of study had been explained. There were informed to withdraw at any time and/or to refrain from responding to questions. Study participants were also informed that all the data obtained from them could be kept confidential using code instead of any personal identifiers. Furthermore, the research procedures were conducted in accordance with the principle expressed in The World Medical Association’s Declaration of Helsinki.
Results
Socio-Demographic Characteristics
In this study, 388 participants responded to the questionnaire with a total responses rate of 99.5%. The majority of participants, 227 (58.5%), were between the ages of 25 and 34 and the mean age of study participants were 29.5 (±4.9 SD). Approximately two-thirds of the respondents, 270 (69.6%) had received formal education. In regard to occupation, 357 (92%) of the participants were housewives. More than two-thirds 344(89.8%) of husbands have a formal education (Table 1).
Socio Demographic and Economic Characteristics of Women in Postnatal Period, in Tembaro District Southern Ethiopia, May to June 2022 (n = 388).

Amhara, Dawuro, Wolayita.
Divorced, single.
Maternal and Child Health Services
Among the respondents, 342 (88%) had attended antenatal care (ANC) follow-up. Of these, 196 (57.3%) had fewer than 3 visits, 146 (42.7%) had 3 or more visits, and 36 (7.6%) had 5 or more visits. During ANC follow-up, the majority, 322 (53.0%), received advice on essential newborn care (ENC). A total of 364 (59.9%) delivered in a health institution, and 354 (58.2%) received immediate postnatal care. The majority of the newborns, 344 (56.6%), were male, and 516 (84.9%) of the mothers did not experience any complications during delivery. Sixty-four (16.5%) of the participants delivered at home, and 251 (64.7%) of the households were visited by health extension workers during the postnatal period. Additionally, 201 (51.8%) of the participants had given birth to 1 or 2 live children, while 187 (48.2%) had given birth to 3 or more children (Table 2).
Obstetrics Factors and Health Service Utilization of Women in Postnatal Period, in Tembaro District South Ethiopia, May to June 2022 (n = 388).

Knowledge of Respondents on Newborn Care Practice
There were about 6 knowledge related questions used to assess knowledge status of mothers toward essential newborn care practice. Mothers who correctly answer more than 50% of the knowledge-related questions are classified as having good knowledge of newborn care practices and accordingly majority, 83% of them have good knowledge on newborn care (Figure 2).
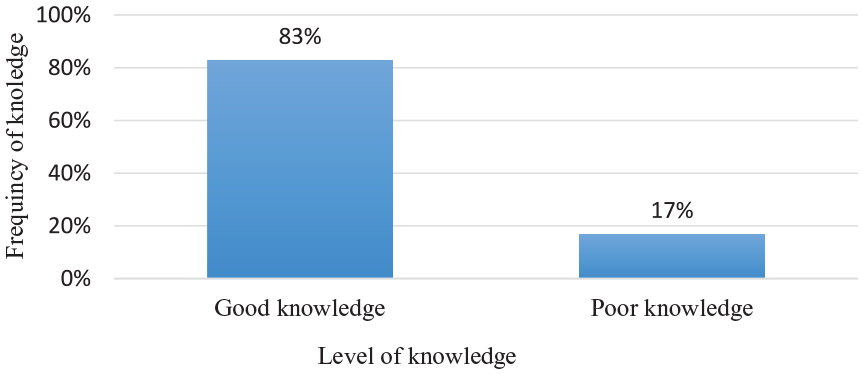
Knowledge status of mothers in postnatal period on essential newborn care practice in Tembaro district, South Ethiopia, May to June 2022.
Out of the total 388 respondents, more than three-fourth, 337 (87%) of them stated that they had the information about newborn danger signs and mothers who have good knowledge on poor sucking, 275(75.7%) followed by fever, 246 (73%; Table 3).
Shows That the Knowledge Level of Mothers on Each Newborn Danger Sign in Tembaro District, South Ethiopia, May to June 2022.

Essential Newborn Care Practice
In this study, 224 (57.7%; 95% CI: 52.6-62.6) of mothers practiced good essential newborn care. Of the responders, 324 (83.5%) reported early breast feeding, 303 (78%) safe cord care, 300 (77.3%) thermal care, 308 (79.4%) delayed bathing, 251 (64.7%) immunization, and 263 (67.8%) at-home eye care (Figure 3 and Table 4).
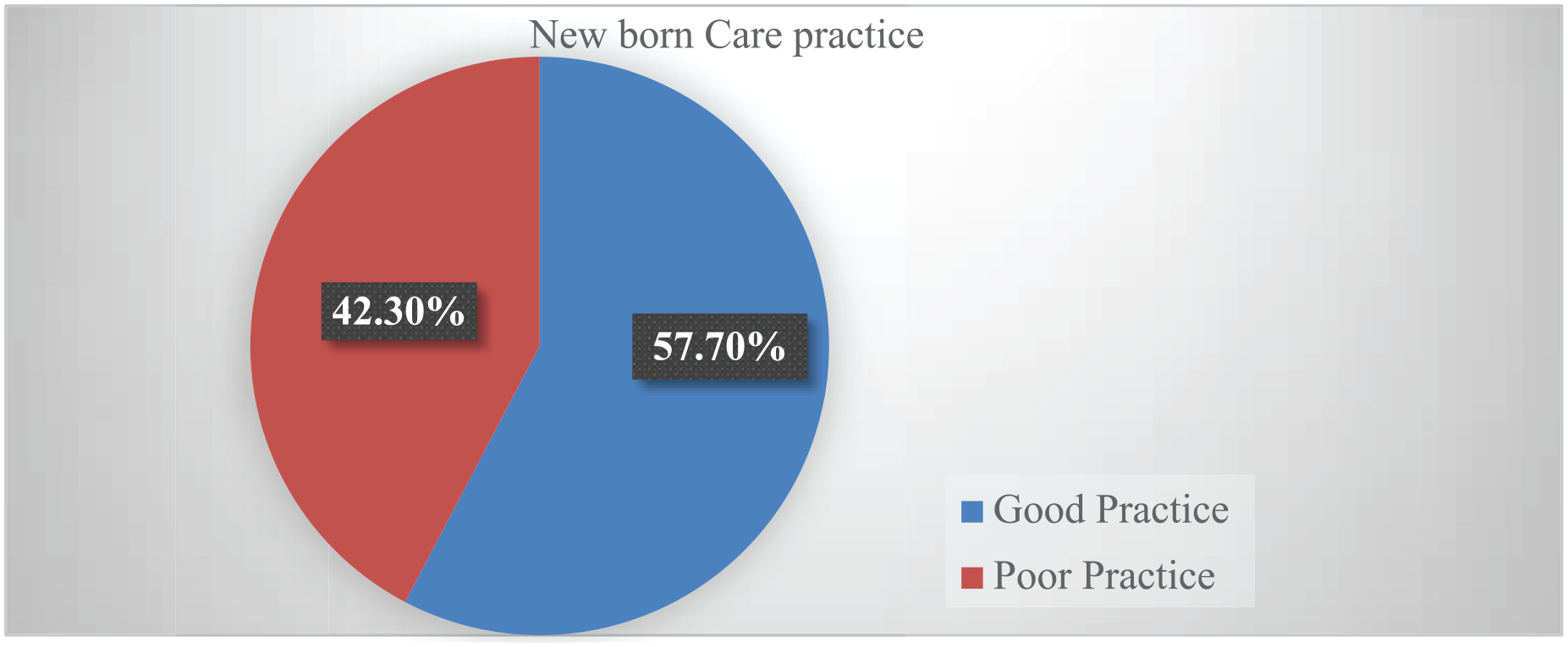
Overall newborn care practice among mothers in postnatal period, in Tembaro district, south Ethiopia, May to June 2022.
Mothers Practice on Essential Newborn Care in in Tembaro District, South Ethiopia, May to June 2022.

Factors Associated With Essential New-Born Care Practices
In this study, maternal educational level, health extension worker home visits during and after pregnancy, number of live births, number of antenatal care visits, and knowledge of newborn care practices were factors significantly associated with good essential newborn care practices.
Mothers who had completed college-level education or higher were found to have a statistically significant association with essential newborn care practices. Those who had completed college-level education or higher were 3.18 times more likely to practice newborn care when compared with mothers who had no formal education (AOR = 3.18, 95% CI: 1.45-6.98).
Mothers who had not been visited at home by health extension workers during and after pregnancy were 68% less likely, and mothers who had visited health institutions 3 times or fewer during their pregnancy were 52% less likely to practice essential newborn care, (AOR = 0.32, 95% CI: 0.19-0.54) and (AOR = 0.48, 95% CI: 0.28-0.81) respectively.
The odds of poor essential newborn care practice were 66% among mothers who had 2 or fewer live births and 76% among mothers who had poor knowledge about essential newborn care, (AOR = 0.34, 95% CI: 0.20-0.57) and (AOR = 0.24, 95% CI: 0.12-0.48) respectively (Table 5).
Factors Associated With Essential Newborns Care Practices of Women in Postnatal Period, in Tembaro district, South Ethiopia, May to June 2022.
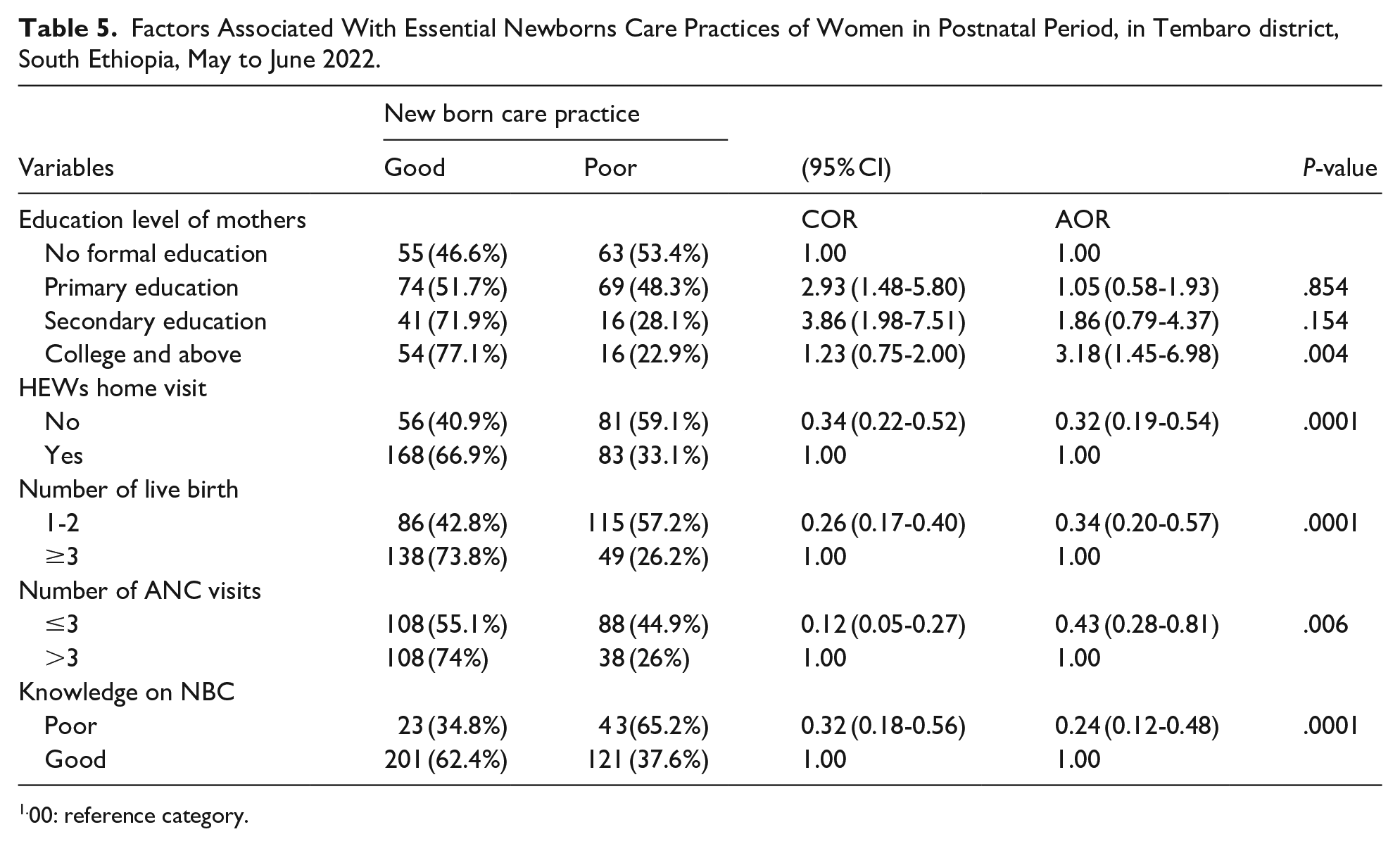
1.00: reference category.
Discussion
The prevalence of essential newborn care (ENC) practices in this study was 57.7% (95% CI: 52.6-62.6). This is considerably higher than the rates reported in studies from Damot Pulasa Woreda (24%) 20 and the rural districts of the Gedeo Zone (24.1%). 21 The observed differences may stem from variations in study settings, timeframes, and healthcare service availability, all of which can influence newborn care practices. Conversely, the ENC prevalence in this study is lower than the 81.1% reported in the Tigray Region, Northern Ethiopia (81.1%). 19 This disparity may be due to differences in socioeconomic conditions, healthcare infrastructure, maternal education, and awareness levels between regions. Additionally, geographical factors may influence access to healthcare services and maternal health-seeking behaviors. These findings highlight the importance of context-specific interventions to enhance ENC practices and improve neonatal health outcomes. In this study, maternal education level was found to have a significant associated with newborn care practices among postnatal mothers. Women who had completed college or higher education were more likely to engage in essential newborn care practices compared to those with no formal education. This finding is consistent with research conducted in Uganda 22 and in the rural district of Gedeo zone, Ethiopia. 21 Educated women are likely to possess a better understanding and knowledge of essential newborn care, leading to increased confidence and improved caregiving practices.
Women who did not receive visits from health extension workers during and after pregnancy were less inclined to engage in proper newborn care practices compared to those who had such visits. This finding is consistent with research conducted in Ethiopia 23 and Nepal. 24 This correlation could be attributed to the potential impact of health extension worker visits in providing crucial guidance and support for newborn care practices to mothers.
Mothers who had 2 or fewer live births showed a lower likelihood of engaging in newborn care practices compared to those with 3 or more live births. This result aligns with studies carried out in Lawra District, Ghana, and Uganda, indicating that first-time mothers were less inclined to exhibit good newborn care practices in comparison to mothers with multiple children.25,26 The consistency in these findings could be attributed to the fact that mothers with 3 or more children may prioritize their newborn care practices more due to their experience with caring for multiple children.
Additionally, frequency of ANC visits during pregnancy was associated with newborn care practices. Mothers who attended health institutions 3 times or fewer were less likely to engage in newborn care practices compared to those who had more than 3 visits 23 and in the Tigray Region of Northern Ethiopia. 19 This is may be attributed to the likelihood of women receiving ongoing guidance on newborn care practices during ANC visits if they attended 3 or more times.
In this study, women with poor knowledge demonstrated lower likelihood of practicing essential newborn care compared to those with better knowledge. This finding aligns with studies in Sindh, Pakistan, 27 and Nepal, 28 which also showed a significant relationship between women’s knowledge of essential newborn care and their actual practices. This association may be due to the tendency of women with insufficient knowledge and awareness to be less inclined to engage in these practices.
Conclusion
This study showed that the level of good essential new-born care practices was found 57.7. Factors such as maternal education, home visits by health extension workers, number of live births, ANC visits, and maternal knowledge on newborn care were identified as independently associated with newborn care practices. It is imperative for primary healthcare providers to consistently deliver essential newborn care and educate mothers on this subject during pregnancy services and home visits.
Limitation of the Study
The cross-sectional design of this study was a limitation because it measured exposure and outcome at the same time. It does not demonstrate a cause-and-effect rela-tionship. Despite the implementation of standardized questionnaires and a shortened recall period to mitigate recall bias, it remains an unavoidable limitation in the study.
Footnotes
Acknowledgements
We would like to acknowledge Wachamo University College of medicine and health science for approving the research project. Furthermore, our special appreciation goes to data collectors for their genuine effort to bring reliable data. Finally, we would like to wholeheartedly acknowledge study participants without them this work could not be realized.
Acronyms and Abbreviations
ANC: Antenatal Care, BF: Breast Feeding, EDHS: Ethiopian Demographic and Health Survey, ENC: Essential Newborn Care, ENCP: Essential Newborn Care Practice HC: Health Center, HEWs: Health Extension Workers, LBs: Live births, MCH: Maternal and Child Health, NBC: Newborn Care Practice, NMRs: Neonatal Mortality Rates, SBAs : Skill Birth Attendants, SD: Standard deviation, SDG: Sustainable Developmental Goals, SNNPR: Southern Nations, Nationalities and People’s Region, SPSS: Statistical Package for Social Sciences WHO: World Health Organization
Ethical Considerations
The study was approved by the Ethics Review Committee (Ref no: ERC/670/2022) School of graduate Study, Wachemo University, Ethiopia.
Consent to Participate
The informed consent with a written signature was obtained upon the agreement from participants after purpose of study had been explained. There were informed to withdraw at any time and/ or to refrain from responding to questions. Study participants were also informed that all the data obtained from them could be kept confidential using code instead of any personal identifiers. Furthermore, the research procedures were conducted in accordance with the principle expressed in The World Medical Association’s Declaration of Helsinki.
Consent for Publication
Not applicable.
Author Contributions
AA: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
DD: contributed to conception and design; contributed to acquisition and analysis; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
TS: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
TL: contributed to conception and design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AS: contributed to conception and design; contributed to acquisition and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
FM: contributed to conception and design; contributed to analysis; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AE: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analyzed during this study are included in the manuscript.