
Abstract
Background:
Pediatric obesity is a serious and widespread medical condition that is increasing in the United States. Unfortunately, family-based programming to address the disorder fails to successfully reach and engage many children, particularly in low-income communities. To provide more affordable, accessible, and scalable programming options, researchers partnered with pediatricians and the Cooperative Extension Service (Extension) in a Midwestern state to develop a collaborative intervention. Partnering pediatricians referred children and families to a weight management program delivered by a trained Extension paraprofessional. The current study describes family experiences with the program.
Methods:
Researchers conducted a focus group or family interview with 13 program completers to elicit program perceptions, experiences with paraprofessionals, and motivators to continue. The focus group and family interviews were audio recorded and transcribed verbatim for textual analysis. Using thematic analysis, researchers examined patterns across transcripts and formulated emerging themes.
Results:
Key themes that emerged included (1) nutrition guidance, (2) interaction, (3) child influence, and (4) family engagement. Families viewed paraprofessionals as compassionate and competent educators who were instrumental in helping families modify health-related behaviors.
Conclusions:
Results of the current study are important to efforts focused on addressing childhood obesity, particularly in underserved communities where access to healthcare services is limited.
Introduction
Pediatric obesity is among the most serious and prevalent nutrition disorders in the United States, 1 and innovative approaches designed to reach and engage children and families in weight management programs are urgently needed. 2 Although evidence indicates that children from lower socioeconomic backgrounds are disproportionately affected by obesity,3–5 interventions are often not accessible or available in low-income communities. 6 Additional challenges with recruitment and retention among families with limited resources have further prevented widespread implementation.7–9
Community health workers, or paraprofessionals, can reach underserved families with children with obesity to provide education, support, and guidance. Extensive evidence supports their effectiveness in promoting healthy behaviors among adults10–14 and children with chronic conditions. 15 , 16 However, family perceptions of weight management programs facilitated by paraprofessionals, information that is essential to understanding satisfaction and attrition rates, remain unclear.17–19 The Cooperative Extension Service (Extension) is a nationwide, non-formal educational network designed to help people use research-based knowledge to improve their lives. 20 Michigan State University Extension (MSU-E) has employed trained paraprofessionals, supervised by professional staff, to accomplish this mission since 1914.
Researchers in the current study partnered with pediatricians at two clinics in Michigan to recruit children (6–14 years of age) and their families into a weight management program delivered by Extension. Trained paraprofessionals, supervised by registered dietitians, delivered the intervention, which was developed by a team of experts in nutrition and family therapy. The 7-week program included a single one-on-one family session followed by six multi-family group sessions over six consecutive weeks. In addition to education specific to obesity causes and complications, the program included cooking and physical activity in every session; child and family goal-setting and monitoring; and information about family communication, behavior change, body image, nutrition, and accessing community resources. The aim of this study was to describe family experiences with the weight management program.
Method
Study design
This was a qualitative assessment of family experiences with a weight management program delivered by Extension paraprofessionals. Researchers completed the assessment through three family interviews and one focus group with program completers. Family interviews each included members of the same family, whereas the focus group included individuals from multiple families. Each individual participated in either a family interview or the focus group. Program completion was determined by family attendance at a minimum of five sessions.
Recruitment and intervention delivery
Because researchers were interested in reaching children and families that may not otherwise have access to weight management programs, two pediatric offices in low-income areas of Michigan were targeted. Families were eligible to participate if their child was an active patient at one of the partnering clinics, between 6 and 14 years of age, English-speaking, and mentally competent to provide assent. As children who were affected by excess weight or obesity were the focus, families were recruited into the program after a pediatrician had identified at least one of their children as having excess weight or obesity (based on body mass index (BMI) percentile). Although children of a normal weight were allowed to participate, it was only upon specific request and, therefore, constituted a small number of participants.
Clinic-based research assistants introduced the program to eligible children and families and obtained parental consent and child assent. Research assistants then reviewed patient charts and recorded children’s health insurance as well as height and weight to obtain descriptive weight status data. Demographic data, including age, gender, and race/ethnicity, were also collected from patient charts. Caregivers provided their own age, gender, and race/ethnicity through self-report.
Following enrollment, the research assistants contacted the local Extension office to provide contact information for families. Extension paraprofessionals scheduled a one-on-one visit in the home or other convenient location to initiate the program. After successful completion of the one-on-one visit, families joined a weekly series of six multi-family group sessions held in the partnering pediatric office buildings.
Family experiences with the program
The week prior to the final session, families were reminded about the focus group discussions that would occur immediately following the final session. At that time, the paraprofessional facilitator verbally invited families to participate with a member of the research team. Although no families refused participation, some were not in attendance during the final session. The researcher who conducted the focus group and interviews (A.S.C.) met families during the first multi-family group session and explained her role in assessing the program. At the time of the study, this researcher was a master’s-level registered dietitian who had previous experience managing community-based programs in low-income communities with a particular focus on the lifestyle management of nutrition-related chronic diseases. She had been trained in qualitative research methods and was working toward her PhD at the time of the study. A focus group guide, developed by researchers prior to the study and pilot tested with children, was guided by literature, research questions, and researchers’ experiences with the topic and population. The focus group and family interviews were conducted at partnering pediatric office buildings between August 2015 and January 2016 and assessed expectations and goals upon enrollment, perceptions of paraprofessional facilitators, motivators to continue participation, information learned, and suggestions for improvement. Only the participants and the researcher were present during the focus group and family interviews. All interviews were audio recorded and transcribed verbatim.
Data analysis
Using a multi-step coding process, guided by thematic analysis, 21 , 22 researchers examined data to uncover and analyze patterns across transcripts, and formulate emerging themes. 23 Two researchers, trained in qualitative analysis, reviewed and discussed the transcripts. The transcripts were then individually coded by these researchers, checked, and discussed until consensus was reached. Initial codes were then grouped into categories and assigned themes. Analysis was an iterative process through discussion and refining of all major themes. Although transcripts were not returned to participants for feedback, whenever there was obscurity during data collection, the researcher (A.S.C.) repeated both question and answer to participants to formally verify responses and ensure the data collected were accurate. All steps and changes throughout the study were documented as ongoing memos by the lead researcher, and all data were coded manually.
All descriptive data related to participant characteristics and weight status were recorded and analyzed using SPSS statistical software (version 23, IBM Corp., Armonk, NY, 2015). Chi-square and Mann–Whitney tests were used to examine differences between program completers and non-completers.
Ethical considerations
Institutional review boards of Michigan State University (study number 14-469) and Hurley Medical Center (study number 708700-2) approved the study prior to commencement of research activities. Written consent was obtained from the children’s legally authorized caregivers and written assent was obtained from children. The study was carried out in accordance with the ethical principles established by the Declaration of Helsinki.
Results
There was difficulty with recruitment throughout the project as no-show rates at partnering pediatric clinics were as high as 50%. Regular reminders from research assistants, clinic staff, and pediatricians were largely unsuccessful. Paraprofessionals experienced additional difficulties with scheduling and attendance at the first one-on-one session. Passive refusal, specifically the failure to respond to paraprofessional calls after enrollment, was the most frequent reason families failed to initiate the program. Paraprofessionals also reported that caregivers refused to answer the door, were not home at the scheduled time, did not have eligible children with them, or asked to reschedule when paraprofessionals arrived. Those who participated in a focus group or interview admitted being uncomfortable with strangers entering their home, sharing that the first home visit was likely a deterrent to participation.
As shown in Table 1, a total of 34 children enrolled in the program with a caregiver and attended the first one-on-one session. The majority of child participants (mean age = 9.48 ± 2.18 years) were African American (53%) or Caucasian (29%), closely reflecting the source population at partnering clinics. Most of the children who initiated the program were affected by obesity (59%) and some (27%) met criteria for having severe obesity. 24 Twelve of the 34 enrolled children (35%) completed the program with at least one caregiver. There was no significant association between program completion and age, gender, race/ethnicity, or health insurance provider; however, there was a significant association between weight status and program completion (Table 1).
Description of children, by level of participation.
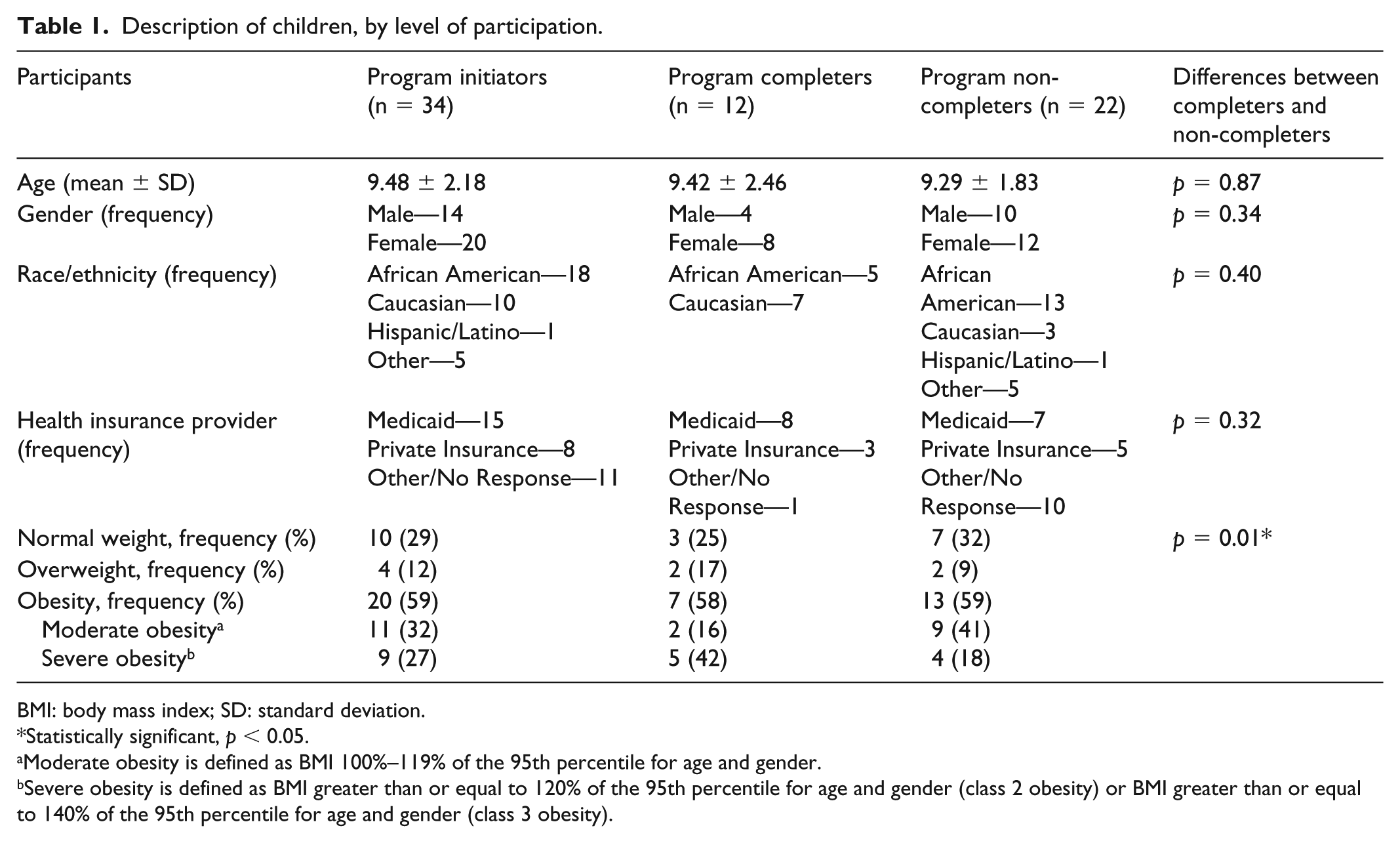
BMI: body mass index; SD: standard deviation.
Statistically significant, p < 0.05.
Moderate obesity is defined as BMI 100%–119% of the 95th percentile for age and gender.
Severe obesity is defined as BMI greater than or equal to 120% of the 95th percentile for age and gender (class 2 obesity) or BMI greater than or equal to 140% of the 95th percentile for age and gender (class 3 obesity).
Seven of the 12 children who completed the program, representing five families, also participated in the qualitative assessment with their caregiver. One focus group was conducted with a total of five participants representing two families; two separate family interviews were conducted with three members each; and one family interview was conducted with two members. As shown in Table 2, child participants (mean age = 9.14 ± 2.79 years) were primarily female (67%). All of the caregivers who participated were women and half were African American. The duration of the focus group and family interviews ranged from approximately 40–60 min.
Descriptive characteristics of focus group participants (N = 13).

SD: standard deviation.
After successfully completing a focus group and family interviews with 13 participants, researchers terminated enrollment and data collection based on a joint conclusion that no additional concepts were being observed. According to previous research on thematic analysis, data can often reach saturation during sampling. 25 Researchers present the findings of the following recurrent themes that emerged: (1) nutrition guidance, (2) interaction, (3) child influence, and (4) family engagement.
Theme 1: nutrition guidance
The majority of caregivers indicated that they enrolled in the program with their children because they needed someone outside of the home to provide guidance with regard to healthy eating, particularly for their children. Many shared daily struggles with the home food environment, noting specific challenges with finding healthy recipes that their children would consider acceptable (Subtheme 1.1). Some further mentioned food preparation challenges in the home.
I was really looking for someone outside of me to let them know there are other ways to eat ’cause I do it all day long. I give them the food they should eat, but they would rather have some pizza. (Caucasian mother of male (age 11) and male (age 9)) My husband is way past 250 pounds. He is the major cook in the house and was reared with a lot of greasy foods. So, we have to eat what he cooks. (African American mother of female (age 14))
Many caregivers admitted that they were unaware of what their children should be eating and needed assistance in both learning about proper nutrition and teaching children how to improve eating habits (Subtheme 1.2). Some described concern with weight status and a desire to assist their children in achieving a healthy weight.
It’s hard to find out what’s missing from what you eat. Sometimes it’s better for somebody on the outside to see. (African American grandmother of female (age 6)) I wanted my daughter to learn positive things, so she won’t be as big as me when she gets older. (Caucasian mother of female (age 10))
When asked why they chose to attend the program, most children responded that they enrolled primarily because their parents encouraged them to do so. Some also shared that they expected the classes to involve a facilitator who would tell children what to eat (Subtheme 1.3).
I thought it was going to be this lady telling you what to do and what to eat. (African American female, age 14) I thought it was going to be like a gym room, and they would tell you what to eat. (Caucasian male, age 11)
Theme 2: interaction
Interaction with paraprofessional facilitators surfaced as a meaningful component of the program. Caregivers talked about each of the paraprofessionals and their active involvement in the classes as well as the strong positive impression they made on participating children (Subtheme 2.1). Many discussed how their children would talk about the facilitators at home, reminding families about new information learned while attending the program.
She (paraprofessional facilitator) was friendly with the kids. She didn’t just give them the (fitness) tools, she showed them different ways to use them. Like, “Here’s a jump rope. Now, you don’t just use it as a jump rope, we can use it to jump back-and-forth or do relay races.” She got up and showed them and did it with them. (Caucasian mother of male (age 11) and female (age 6)) I think she (paraprofessional facilitator) was very personable. Not only that, she could relate very well to them. My daughter loved her and talked about her all the time. (African American mother of female (age 14))
Caregivers and children also discussed the importance of family interactions, both with their own families and with other families who participated in the program (Subtheme 2.2). Many caregivers talked about engaging more with their own children during the program, particularly in relation to health and nutrition. In addition to regular program attendance, some caregivers explained that they spent more time shopping for healthy foods, preparing meals, and engaging in physical activity with their children while they participated in the program. Others shared how they learned to manage struggles in their own family through interactions with other program participants.
With the little pedometer thing, we went for more walks together. ’Cause usually, I just take the baby with me, and the boys sit home. We were able to do a few more things together because my younger son wanted to see his numbers go up. (Caucasian mother of male (age 11) and male (age 9)) I liked the interaction and working together. I really loved it for my daughter. She saw the struggle the other parents and children have and how you work together and can actually meet … just that interaction, I thought was great. (African American mother of female (age 14))
Theme 3: child influence
Researchers sought a deeper understanding of the specific program components that motivated families to continue participation in spite of persistent barriers. Although all caregivers and children indicated that the program was an enjoyable experience for their families, most caregivers said that their strongest motivator for continued participation was their child’s desire to attend (Subtheme 3.1).
I felt bad because I really wondered if we needed to keep going to this. I mean, ’cause I have a lot of stuff going on myself. But for her, it was like she wanted to come. So, it made me think that we are going. We are going to do this! (Caucasian mother of female (age 10)) She looked forward to coming every week. I mean, it was a big to-do. She would count down from Saturday. So, she really enjoyed it. (African American grandmother of female (age 6))
Caregivers and children agreed that the activities, such as cooking and weekly goal-setting, persuaded families to continue participating in the program (Subtheme 3.2). Caregivers specifically discussed goal-setting sheets that were used in each session and highlighted their importance as children developed health-related goals and tracked progress. In addition, caregivers enjoyed watching as their children learned about nutrition through hands-on activities, such as cooking, both in class and at home.
The kids loved the goal-setting. That was something they could do on their own. We wrote out the goal, and at the end of the night, they put a sticker on it. (Caucasian mother of male (age 11) and female (age 6)) She gave us measuring cups and a brush to wash fruit and stuff. Those things were helpful ’cause I can tell them to measure, and we can do it together. So, it was more hands-on. I felt like those things worked and helped. (Caucasian mother of male (age 11) and male (age 9))
Caregivers also seemed motivated to continue because the program was viewed as having a positive influence on eating and shopping habits (Subtheme 3.3). Most credited the classes with introducing their children to new and unfamiliar foods that they were willing to try during class and at home.
We went to the store and bought stuff we tried here. They actually liked the food they tried here … I don’t think they would have even tried it at home. Being here and everybody watching them, they tried the food. (Caucasian mother of male (age 11) and male (age 9)) I went to the store, got a lot of tomatoes and a lot of lettuce and everything. I used to drown my salad in with a lot of salad dressing, and I don’t do that anymore. Our eating habits started changing. (African American mother of female (age 14))
Theme 4: family engagement
Caregivers talked extensively about family engagement and learning. Many caregivers who attended the sessions discussed not only changes in their own health-related behaviors but also changes in the health behaviors of children and adults in the home who did not attend the program. Caregivers shared that their entire family, those who attended and those who did not attend, changed health behaviors as a result of participating in the program (Subtheme 4.1).
Since the class, he (father) has a membership at the YMCA, started drinking water more, and listening to her (paraprofessional facilitator). He never came (to the class), but we talk about it so much when we are home that it’s beginning to slowly rub off on him. (African American mother of female (age 14)) Our goal may have been to eat from three food groups at every meal. And the entire six weeks, he (father) would be like, “Okay, did we actually eat from the three food groups? I did, how about you?” So, we really did it as a family thing. (Caucasian mother of male (age 11) and female (age 6))
Similarly, children discussed a noticeable change in caregiver behaviors related to health and nutrition while participating in the program. Some discussed increases in exercise, while others talked about how caregivers chose more fresh foods or ate out less during the program. Children recognized caregiver support during the program, both from those attending and not attending the program (Subtheme 4.2).
They (caregivers) would make me do my goal, especially my mom. We dance all the time! (Caucasian female (age 10)) My mom has been eating with me, and my mom and my dad and me have signed up for the YMCA … They (caregivers) became more conscious, and they decided to start eating out less and buying more organic food. (African American female (age 14))
Discussion
This was the first study to examine family experiences with a weight management program targeting children and their families delivered through an Extension system. Because the program was less intensive than traditional multidisciplinary hospital- or clinic-based programs, researchers and pediatricians anticipated that patients referred to the program would be mildly affected by excess weight without associated comorbidities. However, the fact that the majority of the children referred to the program were affected by obesity, with some meeting criteria for having severe obesity, is concerning. This overrepresentation of children who had obesity or severe obesity may have been the result of limited programming options in the targeted communities coupled with a recent increase in prevalence of extreme obesity in children. 6 , 24 Recognizing these challenges, partnering pediatricians advocated for the program and encouraged patients and families to participate.
Because researchers chose two vulnerable communities, challenges with recruitment and retention were expected. 26 , 27 Similar to previous studies, regular reminders from research assistants, clinic staff, and pediatricians proved largely unsuccessful. 28 , 29 Failure to initiate the program was most commonly due to nonresponse to paraprofessional calls following enrollment. It is noteworthy that focus group and interview participants described feeling uncomfortable with strangers entering their home, suggesting the home visit was a deterrent to participation. This finding differs from previous research demonstrating that including home visits in child obesity management programs increases accessibility and dosage. 30 , 31
Despite attrition, caregivers who enrolled in the program with their children were highly motivated to do so. One major theme surrounding motivation upon enrollment was caregiver need for guidance to support healthy eating. Previous studies have indicated that parents perceive gaps in nutrition knowledge as an impediment to healthy eating. 32 , 33 Caregivers in the current study recognized a need for external guidance and struggled with finding healthy foods that their children would accept. In addition, caregivers and children reported different expectations and goals when initiating the program. This finding is similar to earlier research regarding family-based weight management programs. 19 , 34 Although children shared only positive feedback following program participation, most recalled a reluctance to enroll because of the expectation that their food preferences would not be considered and they would, instead, be given food mandates. This finding is important as it may have negatively impacted program enrollment and initiation. Although empirical evidence demonstrates that parent–child dyads as a unit of intervention is more effective than focusing only on the child, 35 it is important to understand that caregivers and children likely have different reasons for attending weight management programs.
Family support is essential to children’s weight control. 36 , 37 However, upon enrollment, most caregivers expected the program to specifically target their child. Caregivers credited the program with teaching families the critical importance of working alongside children to change behaviors of the entire family during the course of the program. In addition, most caregivers and children indicated that the information learned in the program was received by family members who did not attend.
Finally, the majority of Caucasian children who initiated the program also completed (70%), compared with only 28% of African American children. This result is similar to previous studies that indicate particular challenges with recruitment and retention of racial/ethnic minority participants in clinical trials. 38 In addition to documented barriers to participation, such as insufficient health insurance, few transportation options, long work hours, and perceived discrimination, 39 , 40 negative perceptions about research participation as well as mistrust of the research community are pervasive among ethnic/minority groups. 41 These well-documented challenges likely presented additional barriers to participation among African American children and families in the current study. 42
Study limitations, in addition to attrition, should be noted. Our sample was small, but researchers were interested in eliciting the unique experiences of families struggling with childhood obesity. In addition, the results reflect experiences of families who completed the program. It is important to recognize that the perspectives of the families who did not complete the program may have differed from those who completed.
Conclusion
The results of this study are important to efforts focused on addressing childhood obesity, particularly in underserved communities. Caregivers and children noted paraprofessional interactions as an essential component of the program, suggesting that paraprofessionals can uniquely benefit communities where access to healthcare services is limited. In an effort to improve enrollment and retention, highlighting activities for children, such as cooking and goal-setting, may be effective in reassuring children that the intervention is considerate of their needs. Future research will incorporate family suggestions in an effort to address barriers to participation.
Footnotes
Acknowledgements
Researchers would like to acknowledge the support of partnering pediatricians Mona Hanna-Attisha, Gwendolyn Reyes, Onyinye Nweke, and Meena Ramani.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Michigan State University Institutional Review Board (IRB#: 14-469).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by graduate funding provided by Blue Cross and Blue Shield Foundation of Michigan.
Informed consent
Written or verbal assent (appropriate for age) was obtained from children and written informed consent was obtained from the legally authorized representatives of all minor subjects prior to study initiation.