
Abstract
Information on risks associated with obesity during infancy specific to Hispanic children is scarce. This retrospective medical record review describes characteristics and parenting practices of Hispanic children age <2 years referred for obesity care at a tertiary hospital over a 6-year period. Data on 29 Hispanic children collected from parent-completed assessment forms and clinician documentation were analyzed. Children were of mean age 16.2 ± 4.9 months; body mass index z scores ranged from 1.5 to 9.4 (mean 4.5 ± 1.7); 45% were male; 97% received public insurance; 38% were breastfed ≥6 months; and 93% had a parent who was overweight or obese. Parenting practices included bottle feeding in bed (50%), regularly drinking sweetened beverages (33%), ≥2 hours of screen time (60%), and having a TV in child’s bedroom (55%). Better understanding of factors that contribute to the development of rapid weight gain of Hispanic children can inform future clinical and public health interventions.
Introduction
Children with obesity often began their pattern of excessive weight gain before entering kindergarten. 1 Rapid weight gain in early infancy has been established as a risk factor for the development of later obesity.2 -4 In infants, higher weight z scores at ~2 weeks of age and having a body mass index (BMI) at 2 months ≥85th percentile are associated with obesity at age 2 years. 5 By age 2, more than 7% of US children present overweight or obesity, and ethnic disparities are already found.6,7 In particular, Hispanic children are at increased risk of overweight or obesity during early childhood. By ages 2 to 5 years, 30% of Hispanic children have overweight (defined as BMI ≥85th percentile), 17% have obesity (BMI ≥95th percentile), 7 and an estimated 3% of 2- to 5-year-old Hispanic children have extreme obesity (BMI ≥120% of the 95th percentile). 8 Once present, obesity is extremely hard to treat. 9 Children with overweight and obesity often continue being affected by obesity into adulthood. Children under 5 years of age with obesity are in need of effective clinical management.10,11
Little is known about extreme obesity during infancy and toddlerhood. Currently, there is no accepted criteria for the classification of excess adiposity in children under 2 years of age.5,12,13 Moreover, infants with weight-for-height z scores >5 may be excluded from analysis in research reports.14,15 As a result, information on prevalence and modifiable factors associated with severe obesity during infancy of ethnically diverse populations is scarce, and identification and treatment is compromised.4,12,15 -17
As a step toward effective interventions for high-risk groups, there is a need to reveal factors associated with the development of severe obesity in Hispanic infants and toddlers. Thus, the aims of this study are (1) to describe characteristics of Hispanic infants and toddlers with obesity referred to our tertiary care clinic and (2) to contrast parent-reported feeding and other child rearing practices in our sample with those reported for a multi-ethnic sample of US infants, and a Hispanic sample of US infants and toddlers. Detailed information specific to populations with increased risk for severe obesity during early ages can aid in early detection of risks and preclude abnormal rates of weight gain in early childhood.
Methods
We conducted a retrospective medical record review of the initial visit of children age <2 years referred for obesity care to the Wellness & Weight Management (W&WM) Program over a 6-year period (April 2007 to July 2013). The W&WM Program is a referral program that provides family-focused care for children of all ages with overweight or obesity. The Program includes physicians, dietitians, physical therapists, and a social worker. During the initial visit, patient information is gathered on medical history, demographics, social history, family history, dietary habits, sedentary and physical activity behaviors, and sleeping patterns. This information is gathered using parent-completed assessment forms and through the interviews conducted by the dietitians and medical providers. The interviews are guided by electronic health record templates. This study was approved by the institutional review board at the Ann & Robert H. Lurie Children’s Hospital of Chicago.
Children’s anthropometric measurements are obtained by clinic staff members using digital scales, and a recumbent infant-length board or a stadiometer, as appropriate. Children are weighed nude or with a dry disposable diaper. Measurement values were to the nearest tenth of a kilogram for weight and to the nearest millimeter for length. Parents self-reported their weight and height during the first visit.
Data Collection
There were 38 patients under 2 years of age who presented for initial visits between April 2007 and July 2013. The electronic health records of these patients were individually reviewed using a structured data form. Records from patients were excluded if they were not of Hispanic origin, or had medical conditions that could significantly influence weight gain or interfere with accurate anthropometric measurements. A total of 29 patients were included for analysis. We excluded 8 infants because they were not of Hispanic origin and 1 Hispanic infant due to history of gross motor delay and hydronephrosis.
Measures
The following data elements were collected: patient demographics, date of first visit and number of visits, anthropometric measurements, dietary history, feeding practices, screen exposure, and sleeping habits, including offering the bottle while child was in bed. Data on the family included demographics, household size, family medical history, parent-reported weight and height, and social history, which included family structure and child care arrangements. Information from a parent-completed assessment form was obtained on the perceptions of the child’s mother and child’s father weight status, classified as “underweight,” “about the right weight,” “a little overweight,” or “overweight”.
Analysis
Parents’ BMI was calculated using self-reported weight and height, and their weight status was categorized as overweight (BMI ≥25 kg/m2) and obese (BMI ≥30 kg/m2). The World Health Organization (WHO) growth standards were used to assess infant growth interpretations as recommended by the Centers for Disease Control and Prevention (CDC). 18 According to the WHO child growth criteria infants and toddlers between the 85th and 97.7th percentiles are considered “at risk for overweight” and those ≥97.7th percentile “in the upper bound” (+2 SDs) of the normal range.5,6,19 Children’s anthropometric percentiles and z scores, including BMI, and BMI percentile were computed using Epi Info 3.5.3. 20 Frequencies and descriptive analyses were performed using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp, Armonk, NY).
Results
Demographic and Child Characteristics
The subgroup of Hispanic children who satisfied inclusion criteria represented 76% (29/38) of the <2 year olds seen for obesity care. This is consistent with the ethnic profile of the population served by the W&WM Program. Child ages ranged from 6.0 to 23.7 months, and 45% (13/29) of children were male. Almost all children in our sample (97%, 28/29) were recipients of public health insurance.
All children lived with their biological mothers, and 93% (27/29) also lived with their biological fathers. Mothers’ ages ranged from 18 to 35 years (mean = 25.8 ± 4.7 years), and fathers’ ages ranged from 20 to 49 years (mean = 29.5 ± 6.7 years). Mean years of education for mothers was 10.7 ± 3.4 years (n = 28), and 10.4 ± 3.2 years for fathers (n = 27). At the time of the visit, 44% of children had older siblings (13/29), and only one child had a younger sibling, with total household sizes ranging from 2 to 9 people (median = 4.6 ± 1.5). Child care was provided in 69% of cases by parents. Only a third of children were cared for by relatives other than their parents, which in 77% of these cases were grandmothers.
Calculated mean BMI for mothers was 29.1 ± 7.6 kg/m2 (n = 26), and for fathers 28.4 ± 5.6 kg/m2 (n = 29). A BMI ≥25 kg/m2 was found in 69% (18/26) of mothers and 86% (25/29) of fathers. Furthermore, 59% of children (17/29) had 2 parents with overweight or obesity (BMI ≥25 kg/m2), and 93% (n = 27/29) had at least one parent with a BMI ≥25 kg/m2. Yet responses on the parent report of perceptions of both parents weight status indicated that only 44% of mothers with a BMI ≥30 kg/m2 and 60% of fathers with a BMI ≥30 kg/m2 were perceived as “overweight.”
No parents reported heart problems or high cholesterol, and very few reported chronic conditions such as diabetes (n = 3) or high blood pressure (n = 1). Four mothers (15%, 4/27) and no fathers reported ever having depressive symptoms.
The most common developmental delay concern in children reported by the parent or noted by a clinician was delayed language development, which was noted in 31% of children. Other concerns included motor skill development (14%, 4/28), behavioral problems (11%, 3/29), and picky eating (3%, 1/29). Overall, the physician noted that 38% (11/29) of children had a developmental concern. Only 59% (17/29) of the children returned to the W&WM Program for a follow-up visit, and 28% (8/29) had 3 or more total visits.
The anthropometric characteristics of the children in our sample are described in Table 1 and Figure 1. All children were at the upper limits of weight for age percentiles, but not at the upper limits of height for age percentiles. As illustrated in Figure 1, only 2 children had a BMI below the 99th percentile, with 92.9th and 98.4th, respectively. BMI z scores ranged from 1.5 to 9.4 (median = 4.4), and 38% of children in this sample had a BMI z score ≥5.
Anthropometric Characteristics.

Abbreviations: SD, standard deviation; BMI, body mass index.
World Health Organization standards.
SD not appropriate.
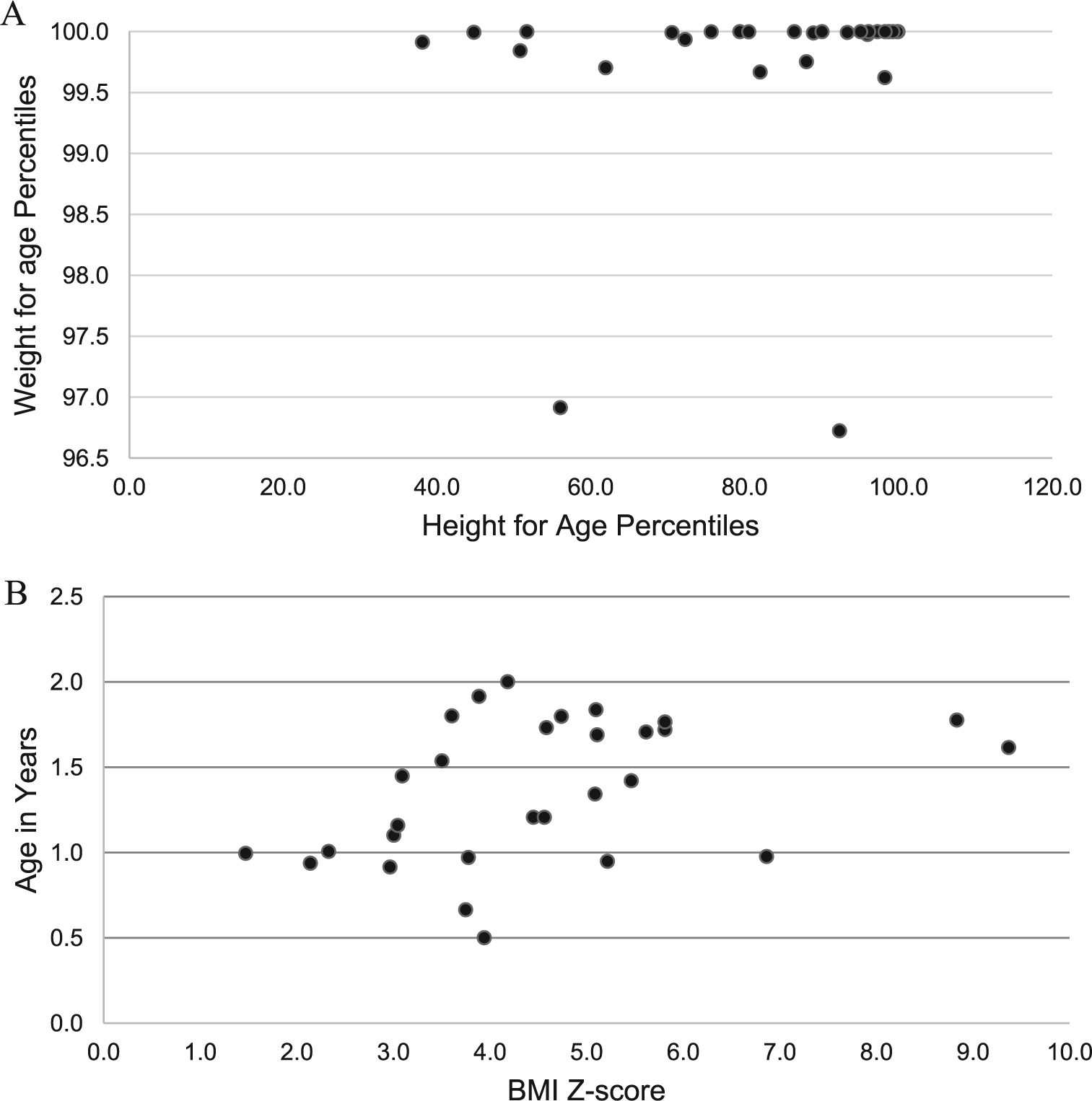
Anthropometric characteristics of W&WM Hispanic young children. (A) Growth interpretations of W&WM Hispanic young children according to World Health Organization standards. (B) BMI z score for age of W&WM Hispanic young children according to World Health Organization Standards.
Feeding, Activity, and Sleep Habits
Feeding, activity, and sleep habits of infants and toddlers are described in Table 2. Most infants in our sample had been breastfed. At the time of the visit, 24% (7/29) of infants were still breast feeding. About one third of parents (9/29) reported that their child consumed soda or sweetened beverages daily, and 71% (20/28) at least one serving of fruit and one serving of vegetables daily. There were 46% (10/22) of children with one or more fast food meals weekly; one child had fast food daily.
Feeding, Behaviors, and Sleep Habits of W&WM Hispanic Young Children and Young Children in National Samples.

Abbreviation: NA, data not available.
Compared to the FF&CW 1999-2003. 27
Compared to The Kaiser Family Foundation Report on US children media exposure. 29
Compared to ECLS-B (9-month-old children). 30
Compared to 2011-2012 NHANES (2- to 11-year-old children). 31
Compared to 2004 National Sleep Foundation Sleep in America Poll. 28
Information on sleep habits and screen time is displayed in Table 2. Parents reported child usual bedtimes ranged from 7:30
Parents reported their child watched an average of 2 hours of television daily (±1.7 hours; median = 1.5 hours; range = 0-6.9 hours). Many children (55%, 11/20) had a television in their bedroom, and 48% (11/23) had the television on always or occasionally during meals.
Discussion
Most of the Hispanic infants and toddlers in this sample had severe obesity. These children had risk factors similar to what has been reported in studies of older children and young children with less severe obesity.15,21,22 In an article reporting characteristics of 1- to 4-year-old children with obesity referred to this same obesity tertiary care program, the group with most severe obesity more often had a history of maternal obesity, sleeping problems (late bedtimes and snoring), and higher intake of juice as compared to the group with less severe obesity. 23
Parental obesity, specifically a high maternal prepregnancy BMI, has been described as a risk factor for infant obesity.15,24 Nearly all of the children in our sample had at least one parent with overweight or obesity, most often their fathers. Medical providers caring for infants should be aware of the role parental obesity presents with respect to the risk for excessive weight gain of their Hispanic infant patients.
Table 2 presents our data and data from national samples of infants and toddlers, including data limited to national samples of Hispanic infants and toddlers. National data on nutrition behaviors are from the Feeding Infants and Toddlers Study 2002 (FITS2002). FITS2002 is a comprehensive dietary survey containing data of 24-hour dietary recall of parents and caregivers of infants and toddlers in the United States.25,26 Data from other national studies that report prevalence of various health behaviors not collected by FITS2002 are also presented; studies include the Fragile Families and Child Wellbeing Study (FF&CW) 1999 to 2003 cohort, 27 the National Sleep Foundation Sleep in America Poll, 28 The Kaiser Family Foundation Report on US Children Media Exposure, 29 the Early Childhood Longitudinal Study, Birth Cohort, 30 and the National Health and Nutrition Examination Survey (NHANES), 2011-2012. 31
A few similarities and differences between our patients and national samples bear recognition. A similar proportion of W&WM patients and those from national samples were ever breastfed. Among the children in the W&WM Program who were breastfed, 38% were breastfed for 6 months or longer, which is notably longer than reported for the national samples.
Reported vegetable consumption by children in the W&WM Program was similar to the vegetable consumption reported by the comparison reference of Latino children. 26 Notably, the vegetable consumption reported by both samples of Latino children, children in the W&WM Program and the national reference of Latino children, were lower than the national comparison reference. In contrast, fruit consumption by W&WM children appears to be higher than the fruit consumption reported by the comparison reference of Latino children, and similar to the national consumption referenced. 26 Although a concerning trend in lower intake of vegetables can be noted among Latino children, findings may be attributable to confounding factors. One possible explanation may be related to the differences in age of each of the samples. The mean age of children in the W&WM sample was 16.2 months, compared to 13.4 in FITS indicating a potential difference in food intake related to older age. 26 Additional alternative explanations may be over- or underreporting intake, lack of knowledge or misunderstanding of serving sizes, and social desirability biases.
Concerning findings were the high intake of soda and sweetened beverages reported for children in the W&WM Program. A third of the children in the W&WM sample were reported to consume soda and sweetened beverages, while this consumption was reported to be 3% and 6% in national samples of US children and Hispanic children, respectively. 26 High sweetened beverage consumption has been found to be a key factor in the development of obesity. 10 In addition, 46% of W&WM children reported eating fast food at least once per week, compared to 8.7%, and 8.4% of 2- to 11-year-old children from national samples of children and Hispanic children, respectively. 31 Previous studies of Hispanic women who immigrated to the United States have identified changes in food and eating practices since immigrating. 32 It is possible that strategies parents use to adapt to a different culture or environment could explain higher intake of soda, sweetened beverages and fast food among the W&WM Hispanic children.
Findings from recent systematic reviews on the effectiveness of obesity prevention interventions delivered during infancy and early childhood may help better understand if addressing the issues we identified in our sample can lead to an effective prevention approach. Most of these interventions have focused on diet, with fewer addressing feeding practices and parenting behaviors. Interventions focused on parent behavioral changes including infant feeding practices and responsiveness to infant feeding ques show promising parental behavioral improvements. 33 In contrast, interventions for infants and toddlers supporting changes in diet quality, including delaying introduction of solids, and complementary foods, as well avoidance of sugar and sweetened beverages have had modest or inconsistent weight outcomes and limited capacity preventing weight gain.33,34 Clinicians may need to consider multiple approaches to have success preventing excessive weight gain during early childhood.
Compared to the children in the FF&CW sample, children in our sample had higher rates of taking a bottle to bed. Usual intake from the bottle while in bed among infants and toddlers has been associated with the development of obesity,27,35,36 tooth decay, and early childhood caries. 37 Recommendations to avoid feeding with a “bottle to bed” primarily promote prevention of dental problems. Since infants and toddlers consume most calories from liquids, clinical recommendations to avoid the use of the bottle while in bed potentially could prevent excessive weight gain. However, there is inconsistent evidence demonstrating weight changes due to modification of this practice. 38
A television in the bedroom was reported more often in our sample than for other national samples of children aged <2 years. 29 More than half of the W&WM children had a TV in their bedroom. The young age of children, household size, and high prevalence of co-sleeping could help explain the higher rate of TVs in the children’s bedrooms. Interventions targeting obesity prevention among infants that have promoted reductions in screen and television exposure have reported reductions in screen time. 33
This study has several limitations. First, this study focuses on an unrepresentative sample of infants and toddlers; thus, the specificity and limited sample size prevents us from being able to make generalizations to the pediatric Hispanic population. Confirmation of our findings are needed. Nonetheless, findings from our study may be helpful in the identification of early obesogenic behaviors that lead to excessive weight gain in Hispanic infants and toddlers. Identification of behaviors that increase risks for severe obesity can help focus prevention efforts. We only present information from the initial visit to the program. Future research should consider examining children’s growth patterns and long-term health consequences of severe obesity during early childhood. Finally, besides the measurements collected for clinical examinations, data were collected from documentation of the clinical encounter and from surveys completed by parents at the time of the children’s initial visit to the W&WM Program, which means information could be affected by social desirability and self-report biases. Particularly, parents are likely to under- or overreport children’s dietary intake. 39
Conclusion
This study provides important information on Hispanic infants and toddlers referred to a tertiary care clinic for obesity care. We are not aware of any other similar report. This study adds to the literature by bringing attention to a population frequently excluded from growth and nutrition-related studies due to young age or extreme obesity. Better understanding of factors that contribute to the development of abnormally high weight of Hispanic infants can inform clinical and public health interventions aiming to reduce childhood obesity and limit health disparities among Hispanic minorities.
Author Contributions
LA: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AOP: Contributed to conception; contributed to acquisition and analysis; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AJA: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
HJB: Contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Authors’ Note
The funding agencies did not have any role in the study design, data collection, analysis, or interpretation of data, nor had any role in writing the manuscript, or the decision to submit the paper for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LA was supported by the Robert Louis Katz Medical Research Foundation, and the Agriculture and Food Research Initiative of the US Department of Agriculture, National Institute of Food and Agriculture, under the Illinois Transdisciplinary Obesity Prevention Program Grant (2011-67001-30101) to the Division of Nutritional Sciences at the University of Illinois. Drs. Ariza and Binns’ research time was supported by a Cooperative Research Agreement between Ann & Robert H. Lurie Children’s Hospital of Chicago and the Williams Heart Foundation.
Ethical Approval
All procedures performed in this study were approved by the institutional review board at the Ann & Robert H. Lurie Children’s Hospital of Chicago. This study was in accordance with the ethical standards of the Ann & Robert H. Lurie Children’s Hospital of Chicago, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.