
Abstract

Background
Rhabdomyolysis is a term that describes the rapid breakdown of striated muscle resulting in leakage of the muscle contents, which include electrolytes, myoglobin, enzymes such as creatine kinase (CK), and other sarcoplasmic proteins. 1 The classic triad of symptoms associated with rhabdomyolysis includes muscle pain, muscle weakness, and dark urine. 2 It is characterized by rupture and necrosis of muscle fibers, which is followed by the rapid introduction of calcium ions into muscle cells resulting in a pathological interaction between actin and myosin and activation of cell proteases. A release of cell products in the bloodstream and extracellular space follows and CK is massively elevated. 2 Rhabdomyolysis is of clinical concern because it can cause acute renal failure, disseminated intravascular coagulation, cardiac arrest and arrhythmias, and significant electrolyte abnormalities, all of which could result in significant morbidity or mortality for the patient. This disease process is not limited to adults, but affects the pediatric population as well.
There are many known causes of rhabdomyolysis. These include direct muscle injury, drugs, toxins, trauma, infection, and hyperthermia.2,3 The leading causes of rhabdomyolysis in children are infection, trauma, and exercise. 3 An association between diabetic ketoacidosis (DKA), hyperglycemic hyperosmolar state (HHS), and rhabdomyolysis has been documented; however, the exact mechanism of this association has yet to be established. 1 It has been proposed that the metabolic disturbances associated with HHS predisposes to destruction of muscle cells, mainly by disrupting the Na/K ATPase pump.4,5 Serum sodium, serum osmolality, and blood glucose were the major determinants for rhabdomyolysis in adults with diabetes. 6 These 3 factors were also implicated in children with diabetes who had rhabdomyolysis, in addition to other electrolyte abnormalities such as hypophosphatemia and hypokalemia.7-9
The main objective of this study was to test the hypothesis that rhabdomyolysis in the setting of diabetes is due in large part to abnormalities in serum phosphorus and/or renal failure. We use a case series approach to identify the clinical characteristics of rhabdomyolysis and specific risk factors for development of rhabdomyolysis in children with diabetes.
Methods
We conducted a retrospective review of the electronic medical record of patients admitted with rhabdomyolysis and diabetes from 2004 to 2014 at the Children’s of Alabama, University of Alabama at Birmingham. The research protocol was approved by the Institutional Review Board for Human Subjects at University of Alabama at Birmingham. We used the diagnosis codes for rhabdomyolysis (ICD 9 diagnosis code 722.88) and diabetes (ICD 9 diagnosis codes 250.00, 250.01, 250.03, and 250.02). The initial review identified 12 subjects with elevated CK. The analysis was further refined based on the extent of serum CK elevation. A serum CK level 5 times higher than normal value (normal = 499 U/L for our laboratory) was considered as the diagnostic criteria for rhabdomyolysis for this study.2,4 Patients were excluded if their hemoglobin A1C (HbA1C) was <6.5%. No patients were on statins. Serum osmolality was calculated according to standard formula: 2 × Na (meq/L) + glucose (mg/dL)/18 + BUN (mg/dL)/2.8. 10 HHS was defined as plasma glucose concentration >600 mg/dL, serum bicarbonate concentration >15 mmol/lL, no or small ketonuria, a serum osmolality of >320 mOsm/kg, and stupor or coma. 11
Results
Final analysis included a total of 7 cases of rhabdomyolysis associated with diabetes: 3 patients with type 1 diabetes (T1DM) and 4 with type 2 diabetes (T2DM). One child with T1DM had associated myositis. Two of the patients also had associated pancreatitis (1 patient with T1DM and 1 patient with T2DM). The patient who had T2DM, rhabdomyolysis, and pancreatitis had a diagnosis of Prader-Willi syndrome. Table 1 lists the demographic and clinical characteristics overall and by type of diabetes. All patients with T2DM were of Black race and obese. All the patients with T2DM and rhabdomyolysis presented as “new-onset diabetes” diagnosis as opposed to the patients with T1DM where only 1 of the 3 was a new-onset diagnosis. All 3 patients with HHS had T2DM. Admission blood urea nitrogen (BUN) for patients with T2DM was higher than those with T1DM (44 ± 8.6 mg/dL vs 15.5 ± 6.4 mg/dL, P = .015). There was a trend for significant difference in serum creatinine on admission between patients with T2DM and T1DM (2.9 ± 0.9 mg/dL vs 1.1 ± 0.1 mg/dL, P = .06). The average serum CK on admission for T1DM cases was 2679 U/L, and for T2DM cases it was 4940 U/L (P = .11). Three patients required continuous veno-venous hemofiltration for their renal failure but none required long-term dialysis. During their intensive care unit stay, 3 patients required ventilator support, 1 required Bipap, and 4 required hemodynamic support with pressors.
Demographic and Clinical Characteristics Overall and by Type of Diabetes a .
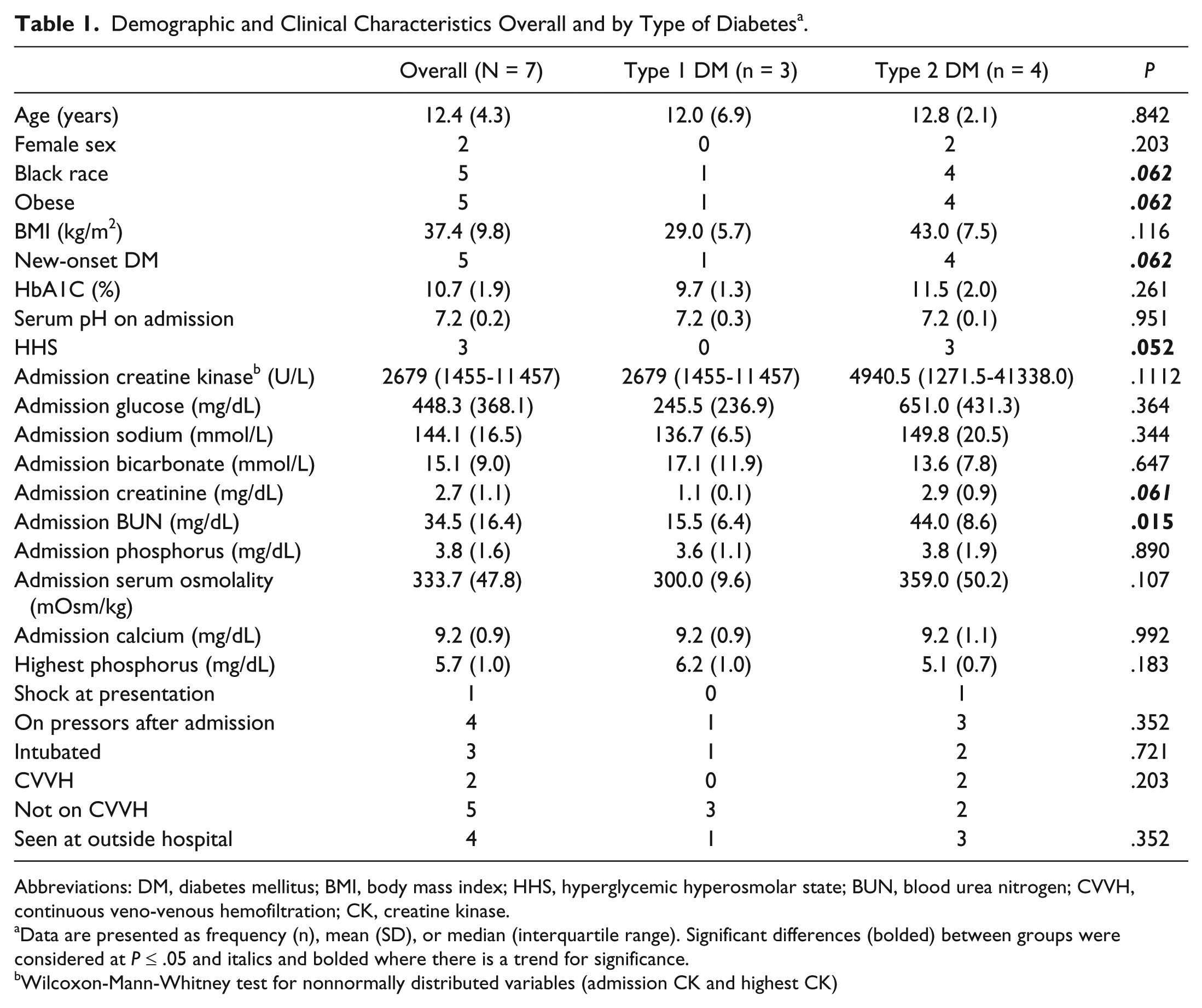
Abbreviations: DM, diabetes mellitus; BMI, body mass index; HHS, hyperglycemic hyperosmolar state; BUN, blood urea nitrogen; CVVH, continuous veno-venous hemofiltration; CK, creatine kinase.
Data are presented as frequency (n), mean (SD), or median (interquartile range). Significant differences (bolded) between groups were considered at P ≤ .05 and italics and bolded where there is a trend for significance.
Wilcoxon-Mann-Whitney test for nonnormally distributed variables (admission CK and highest CK)
Table 2 illustrates laboratory characteristics on the day the patients had the highest serum CK. Serum sodium, BUN, phosphorus, and serum osmolality were significantly elevated in patients with T2DM, and the difference between their values and those of T1DM were statistically significant (P = .008, P = .008, P = .025, and P = .01, respectively). We subsequently analyzed the correlation between serum CK on admission and descriptive and clinical characteristics (Table 3). There was marginally significant correlation between serum CK on admission and higher sodium levels (P = .08). Admission serum bicarbonate was associated with a higher admission serum CK in patients with T2DM (r = 0.96, P = .04). There was no significant association between other variables and CK on admission.
Clinical Characteristics Based on the Day of Highest Serum Creatine Kinase a .
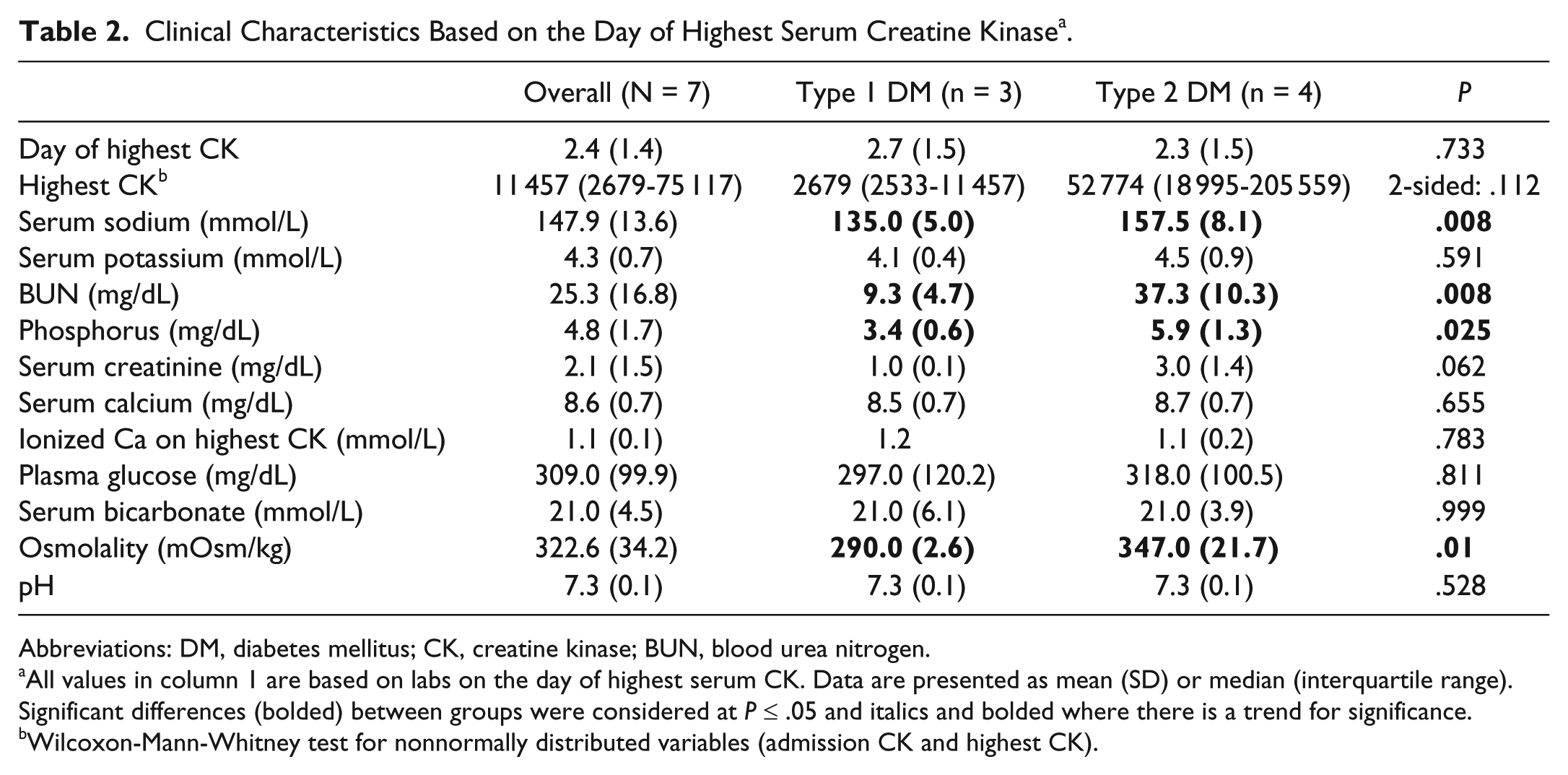
Abbreviations: DM, diabetes mellitus; CK, creatine kinase; BUN, blood urea nitrogen.
All values in column 1 are based on labs on the day of highest serum CK. Data are presented as mean (SD) or median (interquartile range). Significant differences (bolded) between groups were considered at P ≤ .05 and italics and bolded where there is a trend for significance.
Wilcoxon-Mann-Whitney test for nonnormally distributed variables (admission CK and highest CK).
Simple Correlation Analysis Between CK on Admission and Descriptive and Clinical Characteristics a .

Abbreviations: CK, creatine kinase; DM, diabetes mellitus; BMI, body mass index; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; HHS, hyperglycemic hyperosmolar state; BUN, blood urea nitrogen.
Significant correlations (bolded) were considered at P ≤ .05 and italics and bolded where there is a trend for significance.
Nonnormally distributed variables were log-transformed.
Table 4 illustrates the associations between other variables and CK on admission. Overall, females had higher CK (r = 0.81, P = .016); there was trend for positive association between black race and higher serum CK (r = 0.72, P = .068). In patients with T2DM, serum bicarbonate was positively associated with higher serum CK (r = 0.99, P = .01).
Simple Correlation Analysis Between Highest CK Values and Descriptive and Clinical Characteristics a .
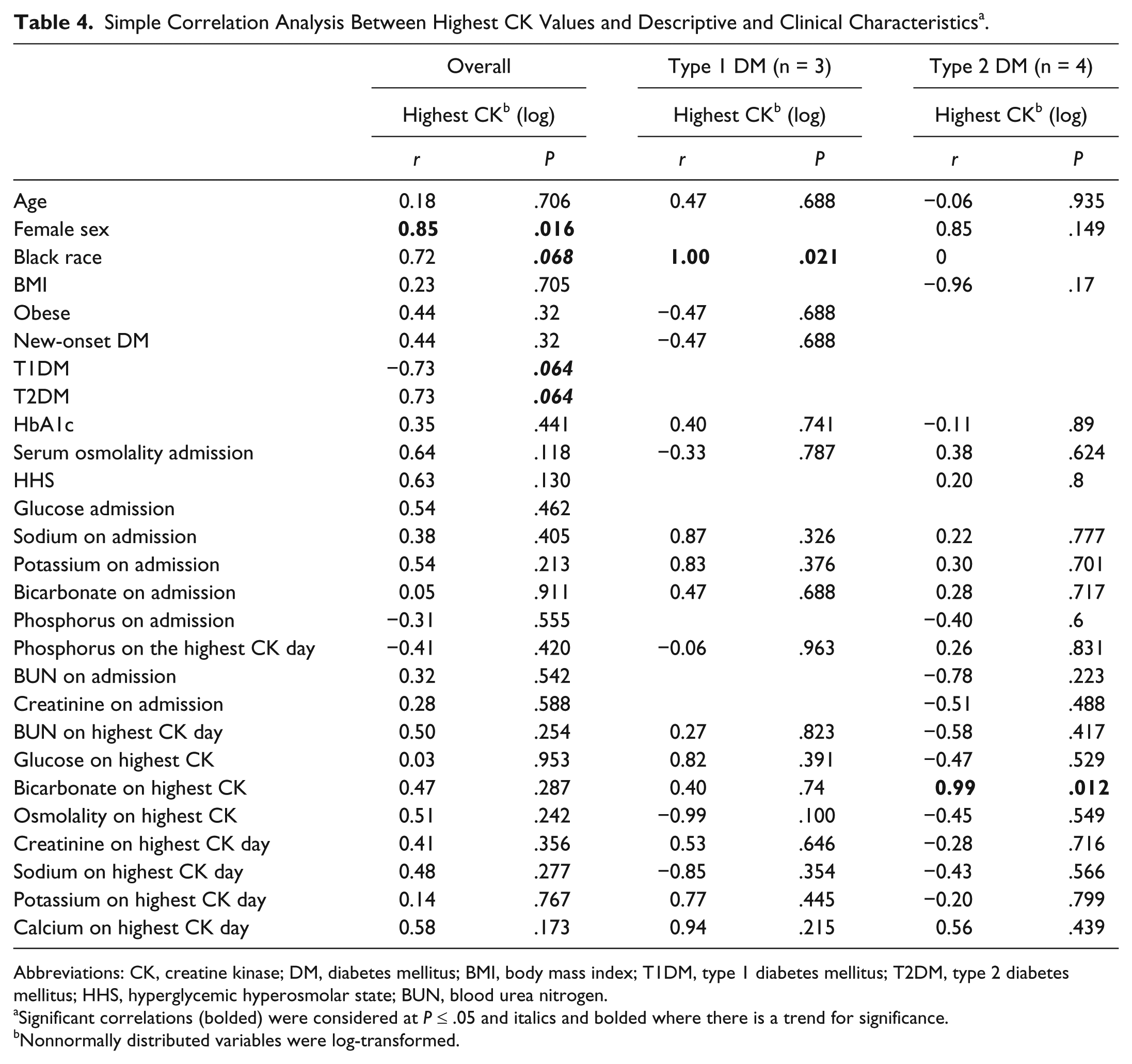
Abbreviations: CK, creatine kinase; DM, diabetes mellitus; BMI, body mass index; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; HHS, hyperglycemic hyperosmolar state; BUN, blood urea nitrogen.
Significant correlations (bolded) were considered at P ≤ .05 and italics and bolded where there is a trend for significance.
Nonnormally distributed variables were log-transformed.
Discussion
Rhabdomyolysis, even though rare, is of great clinical concern in patients with diabetes as it can cause significant morbidity or mortality. Our study compared clinical and laboratory characteristics of patients with T1DM and T2DM who developed rhabdomyolysis.
Admission BUN and creatinine for patients with T2DM were higher indicating that subjects with T2DM presenting with evidence of acute renal failure are at increased risk for developing rhabdomyolysis. Most patients with diabetes who develop rhabdomyolysis were black, obese, and had “new-onset diabetes.” Although not statistically significant, serum CK was higher on day of admission in those with T2DM than in those with T1DM. We surmise that severity of acute renal failure, level of dehydration, and degree of acidosis on admission are likely contributing to the development of rhabdomyolysis.
Several electrolyte abnormalities were present on the day of the highest serum CK value. Serum sodium, BUN, and phosphorus were significantly elevated in patients with T2DM as opposed to patients with T1DM. This suggests that frequent monitoring and careful control of serum electrolytes throughout the first few days of admission can reduce the severity and incidence of rhabdomyolysis. We did not find any association between initial phosphorous and serum CK elevation as we hypothesized. This could be due to the fact that the majority of the patients were evaluated and treated at outside hospitals (n = 4) prior to obtaining a serum phosphorus concentration.
Serum CK was highest in females in both T1DM and T2DM categories. Blacks and T2DM patients had a trend for having higher CK relative to whites and T1DM, respectively. Finally, severity of acidosis was not a factor for highest CK in black individuals.
Data from 41 diabetic adults with rhabdomyolysis revealed that serum sodium, osmolality, and blood glucose were the major determinants for occurrence of rhabdomyolysis. 6 Data from previous pediatric case reports show the determinants of rhabdomyolysis in children with hyperglycemic crisis included severe hyperglycemia, high osmolality, and hypophosphatemia. 11 A case report on 2 adolescent males with HHS and rhabdomyolysis suggests that the level of dehydration and inadequate fluid resuscitation lead to development of rhabdomyolysis. 10 Our study also indicates that preemptive implementation of appropriate fluid management and laboratory monitoring may prevent rhabdomyolysis and the known complications of acute renal failure, disseminated intravascular coagulation, or cardiac arrest in children with diabetes and HHS/DKA.
The major limitation of our study is the small number of patients. The incidence of rhabdomyolysis in adult patients in a diabetic state is estimated at 10%. 12 The incidence has not been outlined in children; however, there are studies demonstrating urine myoglobinuria in 10% of children with DKA. 12 This suggests that rhabdomyolysis might be underrecognized in pediatric patients. With improved recognition of this potential complication of DKA/HHS, along with the knowledge of risk factors outlined above, we could decrease morbidity and mortality related to rhabdomyolysis. Another limitation is the retrospective nature of the study that limits the availability of patient data that would be informative to gain further insight into the pathophysiologic mechanisms.
Author Contributions
SM: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LH: Contributed to design; contributed to interpretation; critically revised manuscript; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AA: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.