
Abstract
Adolescent mothers are more likely to be dissatisfied with their perinatal nursing care than adult mothers. The purpose of this interpretive descriptive study was to explore adolescent-friendly care from the perspective of hospital-based perinatal nurses. Twenty-seven interviews were conducted with nurses with expertise caring for adolescent mothers. Open-ended questions were used to determine how they adapted their nursing practice when caring for adolescents, how they learned to provide adolescent-friendly care, and the facilitators and barriers to providing adolescent-friendly care. Nurses described two main goals: (a) delivering a positive experience and (b) ensuring mother and infant safety. They accomplished these goals by being nonjudgmental, forming a connection, and individualizing nursing care. The nurses described being mother-friendly, regardless of maternal age, and employing strategies to develop a nurse-adolescent mother therapeutic relationship. This research contributes to our understanding of how hospital-based perinatal nurses engage and support adolescent mothers.
Keywords
Introduction
Approximately 2% (7,858) of infants are born to adolescents (≤19 years old) yearly in Canada (Statistics Canada, 2018). This dyad is identified as an at-risk population because of the prevalence of challenging life circumstances and increased prevalence of poor maternal and infant health outcomes associated with adolescent motherhood. For instance, compared with adult mothers, adolescents have higher rates of smoking, substance use, low education, and income; emergency cesarean sections; very preterm birth; infants requiring intensive care (Fleming et al., 2013); and postpartum depression (Cantilino et al., 2007; Hudson et al., 2000). Adolescents are less likely than adult mothers to intend to breastfeed (80.3% vs. 90.1%) and attend prenatal care appointments (73.5% vs. 85.5%) (Fleming et al., 2013).
Some community-based agencies have implemented adolescent-friendly services to engage youth in prenatal care (World Health Organization [WHO], 2012). Outreach programs that facilitate accessible prenatal care may improve perinatal outcomes for adolescents and their children. For example, adolescents in outreach obstetrical programs gave birth to infants with higher gestational ages (p = .005) and birth weights (p = .002) (Fleming et al., 2012). Adolescent-friendly services have been implemented in the community; however, little is known about adolescent-friendly hospital-based perinatal (antepartum, intrapartum, postpartum, and newborn) care.
In Canada, approximately 98% of pregnant women are admitted to hospital for childbirth (Statistics Canada, 2016). The hospital stay is an opportunity for perinatal nurses to engage with, assess, and teach young mothers about important topics such as breastfeeding and postpartum depression. Adolescents have described the quality of their inpatient perinatal care as dependent on the relationship-building skills of individual nurses. They have identified that some nurses are more skilled in establishing therapeutic relationships than others, thus influencing adolescents’ engagement in care and self-esteem. Adolescents respond to friendly, respectful nursing care by identifying health, learning, and social needs (Peterson et al., 2007). Unfortunately, adolescents have reported being judged by nurses, which negatively impacts their transition to motherhood (Brady et al., 2008; Peterson et al., 2007). Consequently, these mothers may decline care or leave the hospital prior to discharge (Peterson et al., 2007). This missed care, “any aspect of required nursing care that is omitted (either in part or in whole) or delayed” (Kalisch et al., 2009, p. 1510), is problematic as new mothers benefit from nursing support and care.
Peterson et al. (2012) published the quantitative results of a mixed methods study that sought to determine whether hospital-based adolescent-friendly perinatal nurses identified a need to improve the care of adolescents. Nurses completed a key informant survey and identified their peers as having varying abilities in the provision of adolescent-friendly care and that quality of care is negatively influenced when nurses hold poor attitudes toward adolescents. Moreover, these key informants identified the need to improve the nursing care of adolescent mothers. These findings support evidence describing the perinatal experience from the adolescents’ perspectives (Harrison et al., 2017; Peterson et al., 2007).
This article’s aim is to report the findings of the qualitative component of a mixed methods study. The quantitative results were published in 2012 by the authors (Peterson et al., 2012). The objectives of the qualitative component of this study were to describe (a) how and why perinatal nurses in hospital-based inpatient settings adapt their practice when caring for adolescents and (b) the individual nursing behaviors and organizational characteristics of adolescent-friendly care in inpatient perinatal settings.
Method
Study Design
Interpretive description was selected as the methodology for the qualitative component of the mixed methods study as it aligns with constructivism and naturalistic inquiry. The aim of interpretive description is to generate knowledge to inform clinical understanding (Thorne, 2016).
Setting and Sample
Between 2009 and 2010, data collection occurred in three hospitals (four sites) in one city in Ontario. At the time of recruitment, 2% (223) of the 9,400 births from all sites were to adolescents (Better Outcomes Registry & Network, 2011). Sites diverse with respect to patient population, size, internal resources for youth, and context of care were selected. All perinatal units (birthing [N = 3], postpartum [N = 3], and neonatal [N = 3]) at the four sites participated and purposive sampling was used to recruit nurses (Patton, 1990).
Nurses were eligible to participate if employed at one of the participating hospitals on a perinatal unit and were considered adolescent-friendly. A research assistant contacted clinical leaders (e.g., nurse educators, unit managers, clinical nurse specialists) and asked them to identify four to six adolescent-friendly nurses from their units. These leaders obtained consent from nurses to be contacted by the research assistant to learn about the study. In addition, these nurses were asked to identify peers who were expert in adolescent-friendly perinatal care. Participants were recruited until two to four nurses from each unit participated in an interview. Two trained, graduate student research assistants obtained written informed consent from each nurse and conducted the interviews.
In total, 34 nurses were invited to participate and 27 agreed to take part in the study; seven declined due to their schedules or felt that they did not have enough experience caring for adolescents. All participants agreed that they were skilled in the perinatal care of adolescents (Peterson et al., 2012). Table 1 summarizes the participant characteristics at data collection.
Participant Characteristics (N = 27).

Data Collection
Interviews were conducted to collect in-depth data to contribute to our understanding of hospital-based perinatal nurses’ perspectives of adolescent-friendly care (Creswell et al., 2003). A semi-structured interview guide (Table 2) was used to conduct face-to-face, audio-recorded interviews. The English interview guide was pilot-tested with birthing unit, postpartum, and neonatal nurses (N = 6) and minor revisions were made. Following this process, the interview guide was translated into French. Participants were offered the choice to be interviewed in English or French. Interviews ranged from 18 to 67 minutes and 24 were conducted in English, whereas three were conducted in French. Following each interview, the bilingual research assistant documented their impressions, thoughts, and observations and noted questions that required follow-up in subsequent interviews with the other participants.
Interview Questions.

Ethics
Ethics approval for the mixed methods study was initially received from the authors’ affiliated university (H07-08-01) and each participating hospital site in 2008. In 2017, an application was submitted to and approved by the university for the first author to complete the analysis of the qualitative data (H06-17-25) as part of her master’s thesis.
Data Analysis
The inductive approach to data analysis employed by the authors follows the method described by Thorne et al. (1997). The purpose of interpretive description is to capture “. . . themes and patterns within subjective perceptions and [generate] an interpretive description capable of informing clinical understanding” (Thorne et al., 2004, p. 3). Interpretive description can develop nursing knowledge when used to explore health experiences, such as adolescent motherhood (Thorne et al., 1997).
The second and third authors had initiated a preliminary analysis of the data in 2010. However, to “know” the data and develop a “feel” for the participants and their stories, the first author began by fully immersing herself into the data by conducting multiple readings of each transcript, listening to the audio-recordings, and reviewing the field notes (Thorne, 2016, p. 167). After each initial reading, thoughts and impressions were documented. Each transcript was then re-read and the “sorting and organizing” of the data occurred as passages that answered the research questions were identified (Thorne, 2016, p. 163). The data were interpreted to formulate broader themes and subthemes. NVivo™ was used to manage the data. It was only after the first author had formulated themes and subthemes that she reviewed and reflected on the preliminary 2010 analysis notes. During the analysis process, the first and second authors met weekly and all authors met for a total of 8 hours to discuss the interpretation of data and the findings. These processes strengthened the findings and improved the comprehensive understanding (Polit & Beck, 2012).
Findings
This vignette is one nurse’s story of caring for an adolescent mother. It provides an example of the life circumstances and vulnerability of some adolescents and an understanding of the compassionate work in which nurses must be skilled to establish a therapeutic relationship with them:
A young adolescent, who already had one child who her parents helped care for, found herself pregnant again upon returning to school. When her second baby was born, he was very sick. Mom had mental health struggles, denied the pregnancy, did not seek prenatal care, and used substances. As a result, many members of the health care team judged this young lady before even establishing a relationship with her. I really felt for her. She was a lost kid and really touched me. A few of us volunteered to be her primary nurses so that continuity could be maintained—it was hard. We had to be careful who we assigned to her because some individuals were not as sensitive as others. I saw a young girl who was scared and yet once she was supported and her needs were cared for, she was very attentive and loving towards her baby. Her family stepped up and took care of her. The feelings of the staff changed over time. At first, there was a lot of chatter in the unit about this baby and mom, but as time went by, people started to see how she had transitioned and triumphed. We had faith that she could do it. She showed us that she wanted to do it, and we got the family home together.
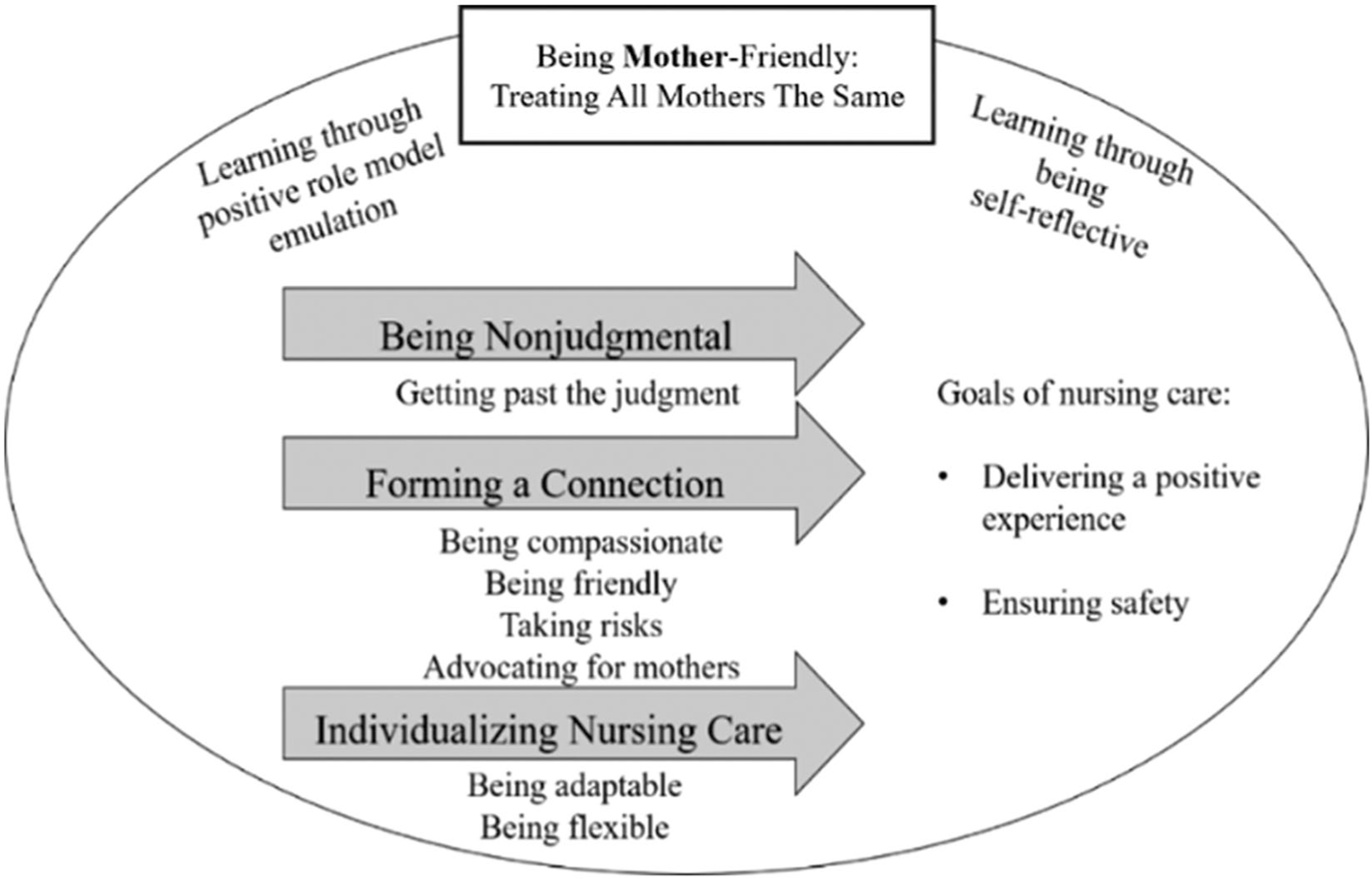
Adolescent-friendly nurses were found to be expert in the relational aspect of caring for adolescent mothers as they embodied a philosophy of care that is being mother-friendly, regardless of age and other life circumstances. Therefore, being mother-friendly was conceptualized as the overarching theme. Three main themes constituted being mother-friendly and can be visualized in Figure 1. The associated subthemes or behavioral characteristics for each of the three themes are also identified. These behavioral characteristics were perceived as having enabled the nurses in the study to accomplish their goals of nursing care, which they strived to achieve for all mothers, regardless of age. The first goal was to ensure that mothers had a positive perinatal experience and the second goal was to ensure that mothers were capable of safely caring for their newborn by discharge. Learning to be mother-friendly is attributed to having positive role models/mentors and being self-reflective on these experiences as well as on other professional and personal experiences.
Themes of adolescent-friendly care.
Figure 2 outlines the facilitators and barriers to the provision of adolescent-friendly care. Each of these issues are embedded within the description of each theme and subtheme as they are reflected when the nurses discuss the ease or difficulty with which they are enabled to enact their philosophy of nursing care within the perinatal context.

Facilitators and barriers of adolescent-friendly care.
Goals of Perinatal Nursing Care
Delivering a positive experience
Nurses described the importance of mothers having a positive experience, the first goal of perinatal nursing care. The nurses demonstrated through their narratives that they genuinely cared about mothers and wanted to make a difference in their lives as new mothers. As one nurse explained, “My goal is to give people a positive experience, no matter what the reason is that they came to the hospital.” Another nurse explained the importance of a positive experience when she stated, “Nurses care about what they do, are passionate about what they do, and want to make a difference. In their hearts, [they] want all women who come here to leave feeling good about their experience.” A positive perinatal experience was enabled when nurses were nonjudgmental, formed a connection with mothers, and individualized nursing care. The provision of nursing care while employing certain behavioral strategies was believed to positively influence the experiences of mothers.
Ensuring safety
The second goal of nursing care was to ensure that mothers were able to safely care for their newborns by discharge. One nurse explained that nurses were “looking not just at the aspect of care while [mothers are] here, but what’s long-term” and consistently asking, “. . . what are their supports at home? Is baby going to be safe? Is mom going to be safe?” The nurses described achieving this goal by recognizing and addressing their parental learning needs. Although these nurses emphasized the importance of providing family-centered care, they identified that their focus was on ensuring that the mother was able to safely care for the newborn.
Being Mother-Friendly: Treating All Mothers the Same
One nurse was intrigued when presented with the term adolescent-friendly and responded, “Adolescent-friendly, hmm, quite a word . . . I don’t think it’s any more adolescent-friendly than it is ‘mother-friendly’.” Nurses described adolescent-friendly care as no different from the care that they delivered to other mothers. Maternal age was described as only one indicator of the potential need for extra effort in establishing a therapeutic relationship and that support and maturity were more influential than age alone. Therefore, nurses preferred to describe care as mother-friendly because they “meet people where they are [at].”
Treating all mothers the same revealed a philosophy of nursing care. Nurses described providing care in a friendly manner to all mothers. When asked how her care differed depending on maternal age, one nurse explained that she “treat[s] them like every other mother in the unit” because “they’re a mother first . . . regardless of what your life experience[s][are] you’re a mum and I’m going to support you in that and respect that title for you.” The nurses revealed a sameness to the care that they provided to all mothers. Nurses qualified this notion by describing the need to provide equitable care, given that mothers of any age may require a greater effort from nurses to establish a therapeutic relationship. One nurse explained, “Their experiences are real. Their pain is real. Everything is the same as you would treat anyone else. They just have a more difficult story, and they can be more challenging” [but] “they don’t deserve less just because their life may be a little more chaotic than the normal.”
It is not that the nurses treat all mothers equally, but they described providing equitable care by putting forth more effort in establishing therapeutic relationships with mothers who are more challenging to engage. Although some nurses attributed expertise with adolescents to treating them in the same way that they care for all mothers, they also recognized that adolescents need additional supports and teaching. One nurse articulated this nicely when she stated, “treat them as adults but with [the] understanding that they don’t have enough years under their belt to have experiences they need.”
Learning to be mother-friendly
Some nurses in this study explained that they did not formally learn to provide adolescent-friendly care. The following nurse could not explicitly identify how she developed expertise in caring for adolescents: “It’s a gut feeling a lot of the time. I can’t really think of any formal teaching that I’ve had, other than my experience(s).”
Learning through positive role model emulation
Some nurses explained that they learned to care for adolescents by “mentoring; it’s watching other people do it” and having role models in their units who were “very good with these mums.” The nurses explained that seeing “what worked and what didn’t work with a mum” helped them learn to care for and engage with these mothers. The presence of staff that were role models facilitated adolescent-friendly care since they
look upon caring for adolescents as something that’s really cool to do and a challenge and really rise to the occasion to make the care exceptional . . . adolescents are leaving feeling empowered and with their baby feeling strong as mothers.
Learning through being self-reflective
Although these nurses described mentoring as having contributed to their knowledge of caring for adolescents, they revealed that it was their reflection on these experiences that resulted in learning. Nurses described that by reflecting on their experiences, both personal and professional, their adolescent-friendliness developed and evolved. “Reflecting on our own personal beliefs and values is a huge skill, [helping us] to know our own limitations, our own judgments.”
Although some nurses articulated that significant life or clinical experiences contributed to their expertise, it was their ability to reflect on these experiences and subsequently learn from them that mattered. This process of learning to be mother-friendly, and hence adolescent-friendly, was described by one nurse who shared what she had learned from her own experiences as a mother of teenagers who
made choices for themselves that pulled me into a world that I never thought I would ever experience . . . those experiences have really helped me open up and understand. Now when I see a teenager, I have such compassion.
She demonstrated that she reflected on her experiences and, as a result, her clinical practice was influenced because of her evolving beliefs.
Being Nonjudgmental
“The most important [adolescent-friendly behaviour] would be for [nurses] to be empathetic and nonjudgmental . . . age does not dictate a person’s ability to be a good mother.” The nurses emphasized the importance of being respectful and accepting mothers of all ages and backgrounds. Being nonjudgmental was strongly evident in the nurses’ stories in which they remained open to life circumstances, personal choices, and family dynamics. Mothers of all ages with vulnerabilities can experience judgment and stigma from providers:
Don’t be judgmental. Just [be] non-biased. Give them the same care you would give every other family. It’s not just teen moms that get judged; it’s families that come in that are low income—you see a bit of that judgment and stigmatism apply to those cases as well. I became a nurse to take care of people and regardless of what this person’s life is like or who they are on the outside, I’m here to [take] care of [them].
Many nurses described that having a child was a personal choice. For example, one nurse explained, “You have to be nonjudgmental, that’s really important. It’s not my life, it’s their life; it’s their choices. My opinion doesn’t matter.” Nurses described the importance of wholeheartedly accepting and supporting mothers and their decisions:
I can’t decide if you’re 13 and wanted [to] get pregnant . . . You can’t change these decisions. What you can do is improve on it for them, or try to help them cope with it in the best way possible.
Being nonjudgmental requires nurses to move beyond the judgment of each mother’s choices regarding pregnancy within complex contexts and focus on the goals of perinatal nursing and their philosophy of nursing care.
Getting past the judgment
The nurses admitted that they make judgments about mothers. However, they acknowledged their biased reactions, described having reflected upon them, and actively worked at being nonjudgmental by engaging in activities that help them to move past the judgments. One such strategy was to shift focus away from prejudicial and stereotypical issues to thoughts of the individual’s needs as a new mother. To identify and meet mothers’ individual needs, nurses focus on a relational ethic of care, which necessitates forming a connection to build trust so that they can get to know the adolescent: “I think that I’m fairly tolerant, nonjudgmental, open. I try not to personalize it. I try and step out of my feelings and just focus on the mum.”
The nurses’ narratives also demonstrated nonjudgmental attitudes toward their colleagues who struggled to provide adolescent-friendly care. One nurse, who was cross-trained in all three units, recognized the uniqueness of her colleagues, similar to the uniqueness of mothers, and acknowledged that “everybody brings their own baggage to the table, as a nurse.” Some nurses have difficulty remaining respectful and nonjudgmental because of this “baggage”; however, regardless of “whatever experience we’ve had, we try to be professional.” Another nurse elaborated that “we all bring our values and beliefs to work with us” and that some individuals, including herself, had a “hard line” about what they were able to move past or not. This figurative “hard line” was described as the boundary at which one’s values and beliefs influenced their practice and may create challenging situations. It is because of this “hard line” that some nurses cannot remain nonjudgmental.
Forming a Connection
Nurses described the hospital stay as a key time to assess mothers’ infant care skills, well-being, knowledge, and supports. It is through nurses’ nonjudgmental and respectful attitudes that adolescents can engage with nurses and form a connection. Nurses described challenges connecting with adolescents due to adolescents’ limited life experiences and previous poor health care provider interactions. Although extra effort was often required to connect with them, nurses emphasized that extra effort could also be required for any new mother.
Many nurses described the importance of establishing a rapport with adolescents (and their families) as they considered this connection to be essential to the therapeutic relationship. Yet, they also described the challenges they could encounter when attempting to connect:
[B]ecause [adolescents] don’t have the life experiences to lean on, they’re very vulnerable. But they have a shell sometimes that makes it a little harder to connect with, but if we can just be open to them, there’s a lot of grace underneath.
The shell to which this nurse referred manifests in a variety of behaviors. Some adolescents and/or their family members enacted in a way that made forming a connection challenging, and sometimes impossible, despite efforts made by adolescent-friendly nurses. Some behaviors identified were associated with alterations to the adolescents’ physical appearance, which seemed to reinforce the social stigma that was often associated with adolescent mothers, such as the display of multiple piercings, tattoos, and clothing choices. Other behaviors were associated with attitudes that could include swearing, use of threatening- or intimidation-like actions, or rule-breaking such as disappearing from the unit, smoking, and substance use.
However, the nurses also provided examples of behaviors in which adolescents and/or their families engaged and facilitated the nurse–mother therapeutic relationship. These behaviors contradicted the biases that stigmatize adolescents. For example, adolescents who displayed inquisitiveness and eagerness to participate in the care of the newborn were perceived to be less of a challenge when attempting to form a connection. In addition, familial involvement and nurturing support extended toward their daughter, as well as the adolescent’s higher levels of maternal maturity and developmental level were factors perceived as positive influences in forming connections. Nurses stated that when these factors were present and combined with compassionate nursing, a therapeutic relationship could form more easily.
The nurses said that having time and patience were essential elements for building trust with adolescents, in order that these new mothers could let their guards down enough to enable nurses to get to know their unique needs and the best ways to meet these needs. The nurses described that adolescents often required them to “prove” themselves: “I think [adolescents are] more on their guard and you have to prove to them that you’re on their side before they let you into their little circle.” Many nurses discussed the importance of establishing trust with adolescents: “It’s important for the nurses to try and get to know the adolescent as well as she can and establish trust early so that she can support her.” Another nurse explained, “You just need to be patient; you know, sometimes you need to just sit in the room with them quietly and with nobody talking.” She then added, “We just have to be willing to communicate with them on their level and have lots of time for them.”
Being assigned to the same patient over a period of time was described by the nurses as a facilitator to mother-friendly and adolescent-friendly care as it provided an ongoing opportunity to develop a therapeutic relationship with adolescents and their families. Continuity of carer, with the provision of time it offers, enables nurses to perform a more holistic assessment of their patients’ support and what is needed:
[B]eing that a lot of the babies that we see in the NICU are there long-term, we have the ability to have that time to get to know the parents, again regardless of age. For adolescent-friendly care, that time allows the nurses to get to know mom or dad or the support system and really get to know who or what they can do to help them to get to a point where they’re able to care independently for the baby and take them home.
Some nurses described an association between their ability to establish a therapeutic relationship combined with a true desire to form that connection. One nurse explained that “knowing how to connect with that mom sometimes just requires patience and the experience of having built relationships with several moms over several years [because then] you can go into it with a little bit more confidence.” She elaborated on this relational aspect of care by explaining that to be an adolescent-friendly nurse, a true desire to form a connection needed to be combined with one’s experiential learning of caring for adolescents: “You are not just coming in here to do your job and get out; you truly want to build a relationship with that family [to] meet [their] needs.”
Being compassionate
The nurses emphasized the importance of having compassion for mothers and its role in the development of a therapeutic relationship. One birthing unit nurse described compassion in caring for an adolescent mother when she stated, “This little gal really opened up well. She talked; there was eye contact; there was touch between myself and her, between her mum. It was a very warm and very accepting environment that she laboured and delivered in.”
One nurse explained that she felt that
it’s important for me to tell them, “You can succeed. This is not an ending. This is a beginning.” You don’t need to be told, “You shouldn’t have been pregnant in the first place.” You need to be told, “What you’re doing is brave.”
This nurse’s compassion was evident as she described empowering adolescents. Treating individuals with compassion and facilitating a positive experience amid vulnerabilities and suffering, recognized as common among adolescents, was described by this birthing unit nurse:
A nurse that’s giving you information, is positive, holding your hand, and says, “Look, I’ll stay with you, I’ll be here, I’ll tell you if something’s wrong” makes a big difference than somebody who just leaves you there on a cold table by yourself and doesn’t explain anything. It makes a difference—more so for people who are already vulnerable.
When asked about caring for and supporting adolescents, one nurse explained that “extra special kindness is the medicine that I give: I just really want to be super kind to them so that they will be open and receptive when I want to take care of them or teach them something.” This “special kindness” was common among nurses who described the generosity of spirit that many adolescent-friendly nurses embodied. Nurses referred to adolescent-friendly care as compassionate, generous, respectful, nurturing, and being “open, nonjudgmental, and really coming from your heart.”
Being friendly
Nurses described having friendly interpersonal relations with adolescent mothers as a behavioral strategy to build trust, which was needed to establish a therapeutic relationship. One nurse described that “getting [adolescents] to talk about their life by asking them questions about school and friends and what they do outside of their home and what their interests are, tends to make them more trusting.” Being able to build trust was perceived as a crucial component of adolescent-friendly care. When asked to describe adolescent-friendly care, this nurse focused on trust:
I think adolescent-friendly is care that opens the door for adolescents to trust and to feel supported and that they can express their needs in whatever way they feel they need to with their provider. So that there isn’t a barrier between the adolescent and the provider, there’s flexibility, trust, openness, respectfulness where the adolescent doesn’t feel judged and feels that she can be open.
Taking risks
Many nurses described the need to engage in risk-taking behaviors to facilitate the building of a trusting relationship with adolescents. These risks included such actions as bending some organization- and unit-based policies, pushing their own boundaries and level of comfort with confronting negative adolescent behaviors and setting acceptable limits, and heightening the timing and types of nursing care approaches they employed to engage the mother. The nurses explained that to be able to take risks, one must be confident in one’s own nursing knowledge and critical judgment, with a willingness to bear the consequences of risk-taking. One nurse provided an example of risk-taking as “[having] to ask those hard questions” in relation to substance use during the perinatal period. She described that although it is challenging to do, it is important to be patient and honest with adolescents by “[taking] the time to sit down with them and talk about it openly . . . if it’s been disclosed a few times, then you know they’re willing to talk about it.” She acknowledged that the risk of asking the hard questions may only pay off depending on how the nurse “come[s] across and how you can get them to open up.” Being honest, considered to be a form of risk-taking within the context of caring for adolescents with trust issues, was a common behavioral strategy of being adolescent-friendly. The nurses recognized the importance of being able to ask the hard questions and to be honest and upfront, yet supportive, in the way that they responded due to adolescent mothers’ vulnerabilities:
[I]t’s a very scary world out there, and if somebody doesn’t try to support you in a positive way―because I think a lot [of the reason] these people are pregnant at 13 or [in their] teenage years is because [of a] lack of support―because of that, you need to be that much more there for them and to be honest and upfront with them.
The nurses acknowledged that when caring for adolescents, it was important to “pick your battles, because you’re not going to win them all.” One nurse provided the example of encouraging adolescents to consider breastfeeding, quitting smoking, and returning to school:
Maybe you’re not going to win all three of those. Pick the one that you think most likely . . . If she’s not going to quit smoking [come] hell or high water—maybe you can get her to breastfeed. Maybe that’s the one that you work on. You find where you think she’s most responsive and try to get her to see that as a better choice.
Another nurse described the care of adolescents as “need[ing] an extra bit more creativeness. It’s more creative care and trying to break down the barrier.” This notion of creative care was supported by other nurses who provided examples of taking risks by creatively interpreting the rules and policies. These nurses disregarded criticism from their peers, thus risking their relationships with their colleagues who had negative attitudes toward adolescents. However, these nurses took calculated risks with their practice and were able to distinguish when to do so and when not.
Advocating for mothers
Being an advocate for mothers required that nurses foster interdisciplinary teamwork. One nurse explained how teamwork helps her to be adolescent-friendly:
[T]eamwork helps. Social work, I like to get involved as soon as I can . . . I use the whole team as much as I can, depending on where [the mother] is in her labour . . . you treat them the same as you would anyone else; if I notice that she might be put on the back burner, I’ll definitely advocate and get the whole team to come see her.
The availability and accessibility of an interdisciplinary team, with positive attitudes toward adolescent mothers, was described as a facilitator to adolescent-friendly care. One nurse described the importance of
having a good strong adequate support network for them before they deliver . . . social work is available for them, the nutritionist is available for them, triage is available for them if they have a concern or a problem.
This nurse elaborated that involving the entire health care team promoted the holistic view of health for the adolescent that is essential for these vulnerable mothers: “Constant assessment of their emotional and psychological needs during the whole process, not just that 12 hours that we have them for. Access to care, that’s it.”
Just as the interdisciplinary team can have positive influences on adolescent-friendly care, negative attitudes or outlooks of individual team members can pose a barrier to care and make being an advocate more challenging. One nurse described the impact of the business-oriented nature of some providers and the lack of holistic care:
There are a few [providers] that you kind of think it’s unfortunate that these girls get paired up with them. They are very business-oriented. They’re very matter-of-fact. They don’t consider it their job to do any of the social work stuff.
Many nurses explained that their units had limited adolescent-specific teaching resources regarding the labor, birth, and delivery process and community resources. This lack of resources made it more challenging for nurses to advocate for adolescent mothers in their discharge teaching and to connect them with a support network upon being discharged home:
[T]here’s no resources at hand that can point us to where we can give this information to the mums easily . . . that would help―having more resources on the unit that we could provide the mums, or even to provide us so we can have a better follow-up in the community . . . I’m really not aware of what’s out there for these mums once they leave.
Individualizing Nursing Care
“Every situation is different, so I don’t say because she’s young she’s not going to do this . . . I approach every client differently.” The participants described individualizing nursing care for all mothers as essential to recognizing and being sensitive to the unique needs and situation of each mother. Although the nurses described their philosophy of care as providing the same care for all mothers, they adapted the strategies they use to connect with mothers to each situation and the needs of the mother, her infant, and the entire family.
The uniqueness of each mother is evident when considering adolescents and their development. Adolescent mothers of various ages “are at different developmental stage[s] so it is important to assess and recognize what stage they’re at and to meet your care to those needs.” Many nurses asserted that age does not determine maturity or parenting abilities because “. . . some adolescent moms are more mature than adult moms and some of the adolescents are more interested and engaged than other parents . . . care has to be adapted in the situation.”
Being adaptable
Virtually every nurse described the importance of adapting care to meet the individual needs of each mother and her situation while remaining nonjudgmental and respectful in the care approach. One nurse explained,
. . . if you are the type of person that is able to very quickly see beyond age, socio-economic status, or certain demographic information [and] to be able to very quickly get to know that mother as an individual [then] that enhances your ability to really cater the care to meet her needs, and her role as a mom.
One neonatal nurse stated that being adaptable was a facilitator to adolescent-friendly care. Although she described the importance of adapting adolescents’ care, she argued that this was not unique to maternal age:
You adapt your care, your care plan, and all of the teaching. You may find a very mature adolescent that you can chat with straight-up with a specialist and not have a problem, and you may end up with an adult who’s got some emotional or psychological situations where they’re at a level of an adolescent, and you have to adapt to that.
Being flexible
Demonstrating flexibility was described by the nurses as essential to their nursing care, specifically to adolescents. One nurse stated the following: “How do I describe adolescent-friendly nursing care? It has to be quite a bit more flexible when it comes to dealing with adolescent mothers than older mothers.” The behavioral strategy of being flexible and adapting care was supported by the following nurse:
[T]o provide good care nurses have to be able to be flexible, like to meet people where they’re at learning needs wise or support needs wise and help them along to where they know they need to be. When we say who provides good care, who provides bad care, I think it’s nurses that are able to meet people where they are and be supportive in the teaching that needs to happen versus some that are more rigid.
When asked about policies that may influence adolescent-friendly care, the majority of nurses identified the visitation policy. This policy was a barrier as it restricted the number of visitors that a mother could have at a given time. The nurses recognized that social support was essential for adolescent mothers; therefore, flexibility regarding the number of visitors was common among the participants. One nurse explained that
. . . if they wanted their three best friends and their mother with them for [labour and birth], then that’s what they wanted. And sometimes that requires some negotiation with your [charge nurse] and asking them to trust you to police that.
Being flexible often required the nurses to take risks.
Discussion
Adolescent-friendly perinatal care was described as being mother-friendly; that is, the nurses identified that regardless of vulnerabilities, such as young age and life circumstances, they treat all mothers the same. Being mother-friendly is the philosophy of care that is embodied by adolescent-friendly nurses and because of this, these nurses are perceived to excel at caring for and connecting with adolescent mothers. As a result of this philosophy, nurses treat adolescents in the same way as other mothers, but have the understanding that adolescents are more vulnerable due to limited life experiences.
Interestingly, this finding is congruent with the adolescents’ perspective. Adolescent mothers have identified that they want to be treated as a new mother instead of an adolescent with an infant (Low et al., 2003; Peterson et al., 2007). Adolescents expect their nursing care to be similar to the care of other new mothers because they do not consider their needs to be any different (Peterson et al., 2007). This demonstrates the uniqueness of the inpatient perinatal nursing context as mothers and nurses alike have described adolescent-friendly care as being the same as the care delivered to other mothers. In other health contexts, adolescent-friendly care is delivered in a different way such as with shortened wait times, with or without appointment, and with swift referrals to improve the acceptability of health care (WHO, 2002). Although treating all mothers the same was an overarching theme among the nurses’ narratives, they described this to mean providing equitable rather than equal care to mothers. Care is considered equitable as nurses identified putting forth more effort in therapeutic relationships when it is more challenging to connect.
Societal stigma and negative health care provider attitudes are a barrier to adolescents accessing health services (Burgess et al., 2004; Escarce, 2005). There is evidence that when adolescent mothers sense judgment and/or disrespect, they may decline nursing care or leave the hospital before discharge (Peterson et al., 2007). The nurses in this study identified that they were able to remain respectful by placing their own personal values and beliefs aside when delivering nursing care. Patients have described key elements of respect as including empathy, care, autonomy, providing information, recognizing individuality, demonstrating dignity, and attending to needs into nursing care (Dickert & Kass, 2009). Interestingly, in relation to the concept of adolescent-friendly and thus mother-friendly care, the themes that were derived from the interview data align with these elements. For example, the nurses described the importance of compassion and having empathy, connecting with mothers, remaining nonjudgmental, and individualizing nursing care.
The nurses ultimately described a relational ethic of care, that is, the situation of ethical action in a relationship (Bergum & Dossetor, 2005), as their philosophy of nursing care. Relational ethics regards the manner in which individuals engage and connect with one another. Austin (2008) describes that being open to all individuals and their life circumstances is essential to ethical action. This description of relational ethics is therefore easily applicable to providing adolescent-friendly perinatal nursing care. Mutual respect, open communication and dialogue, engagement, and an interdependent environment are core concepts in relational ethics and were mentioned in the participants’ descriptions of adolescent-friendly and mother-friendly care.
According to adolescents, adolescent-friendly nurses are skilled in the relational aspect of nursing care (Harrison et al., 2017; Peterson et al., 2007). Caring and the therapeutic relationship is central to nursing care and greatly contributes to the health and well-being of patients (Benner & Wrubel, 1989). The purpose of the therapeutic relationship is to meet the health care needs of the patient, and the nurses in this study described the importance of building trust to form a connection with adolescent mothers. Nurses described the ability to form a connection with adolescents as essential to being able to provide individualized care. The nurse–patient therapeutic relationship enables nurses to plan, deliver, and evaluate care in an individualized, person-centered manner (Gordon, 2006).
The nurses in this study described individualizing the care that they provided to all mothers. Mother-friendly, and hence adolescent-friendly, care was described as maternal, patient-centered care that is provided in a respectful, nonjudgmental, and relationship-centered manner. Perinatal nursing care was described by the nurses as needing to be mother-friendly, specifically in the case of adolescents. Nurses described that this approach develops from a foundation of respect and responsibility.
Implications and Recommendations
Individual nurses can improve the inpatient perinatal experience of adolescent mothers (Peterson et al., 2007). Although adolescent-friendly training is a recommendation for all health care providers (WHO, 2002), the nurses in this study could not identify any adolescent-friendly training that they had received and they described learning to be mother-friendly by reflecting on their own personal and professional experiences. Perinatal units can foster learning to be mother-friendly among their interdisciplinary team by (a) providing workshops where the stories of adolescent parents or parents with other vulnerabilities are shared to foster reflection, (b) providing opportunities for mentorship of students and nurses who have identified the need to improve their interactions with mothers with vulnerabilities, and (c) conducting debriefing sessions of more challenging cases to foster reflection (Johns, 2002, 2010).
Moreover, to promote mother-friendliness at the individual level, it is recommended that perinatal health care providers receive training in and employ trauma-informed care (Harris & Fallot, 2001). A trauma-informed care approach is recommended because there is a strong relationship between adolescent pregnancy and trauma such as abuse, intimate partner violence, substance use, and mental illness (Hillis et al., 2004). The nurses in this study did not explicitly state that they employed a trauma-informed approach to the care of adolescent mothers; however, in their narratives, they shared stories of adolescents who had experienced trauma and thus they described the importance of delivering care in a sensitive and supportive manner.
At the unit level, mother-friendliness can be promoted in two ways. First, it is recommended that perinatal units employ a liaison nurse to keep in-hospital nurses informed and up-to-date about community-based resources and referral programs. The nurses in this study identified the need for education and information regarding community resources and supports as they had limited knowledge of the programs available for adolescent mothers. The liaison nurse is an effective way of creating links between hospitals and community programs in various health care settings (Hofmeyer & Clare, 1999; Jowett & Armitage, 1988). The liaison role has the potential to support the referral process for adolescent mothers to community-based programs in the postpartum period upon discharge from hospital. Second, continuity of carer was identified as a facilitator to mother-friendly care and nurses recommended that perinatal units implement a primary nursing model of care. There is evidence that relational continuity has been associated with a positive birth experience (Mattila et al., 2014), the feeling of safety during labor (de Jonge et al., 2014), and breastfeeding (Wan et al., 2011).
This study has made novel contributions to the evidence regarding adolescent-friendly care from the perspective of hospital-based perinatal nurses. The findings support the need for future research to design and test interventions to (a) promote self-reflection among perinatal nurses and (b) improve hospital-based perinatal nursing care through the reduction of health care provider stigma and the betterment of attitudes to facilitate connecting with and engaging mothers from vulnerable populations.
Strengths and Limitations
A study strength is the number of interviews conducted and the richness of the data collected from expert adolescent-friendly nurses. Although the first author did not collect the data, she became fully immersed through re-reading the data collected and listening to audio-recordings. The original research members involved in data collection and the initial preliminary analysis remained involved.
The data collection for this study occurred between 2009 and 2010 and there was a delay in completing analysis and publication. However, key stakeholders and adolescents from community-based agencies have confirmed that negative health care provider attitudes toward adolescent mothers continue to negatively impact the quality of perinatal care that adolescent mothers receive (B. MacKillop, Personal Communication, October 3, 2018; Harrison et al., 2017). In addition, the study findings were presented at three conferences and many health care provider audience members shared similar experiences and thoughts about adolescent-friendly care thus supporting the study’s trustworthiness (Polit & Beck, 2012).
Conclusion
The expert nurses participating in this study embody a philosophy of providing the same care for each mother regardless of age and life circumstances. However, these nurses use various strategies to form connections with mothers who initially resist engaging with health care providers. The therapeutic relationship permits nurses to more accurately assess mothers with vulnerabilities and to individualize care to more effectively meet the needs of each mother and family. Our findings describe (a) how and why perinatal nurses adapt their practice when caring for adolescents and (b) the individual nursing behaviors and organizational characteristics of adolescent-friendly care in inpatient perinatal settings. The findings of this study complement the quantitative research published by Peterson and colleagues (2012) by providing greater depth to our understanding of expertise in the nursing care of adolescent mothers. Peterson et al.’s (2012) key informant survey results raised the question: “Are some nurses expert in the care of adolescent mothers because they are expert in the care of all mothers?” This study has revealed that nurses who are expert in the care of adolescents are expert in this care as they embody a philosophy of care that is being mother-friendly, regardless of age and life circumstances.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.