
Abstract
Early health care seeking could save neonates’ lives and have a significant role in decreasing neonatal death, while delayed health care seeking has many contributions to neonatal mortality. Therefore, this study aimed to assess maternal health-seeking behavior for neonatal danger signs and associated factors among postpartum mothers in Southeast Ethiopia. A community-based cross-sectional study was conducted on a random sample of 400 women with sick neonates from June 1st, 2020 to 27th, November. A Modified Anderson and Newman behavioral model consisting predisposing, enabling, need, and health system factors were utilized and participants were interviewed by using structured questionnaires. Multivariate logistic regression analysis was used to identify factors associated with maternal health-seeking behavior. Adjusted odds ratios (AOR) were reported with their corresponding 95% confidence interval (CI) to determine the strength of the association. The statistical significance was declared at P < .05. Slightly higher than two-fifths, (44%, 95% CI: 39.2-48.9) of the respondents’ have appropriate healthcare-seeking behavior for neonatal danger signs. Postnatal care follows-up (AOR = 3.5; 95% CI: 2.06-5.80), good knowledge of neonatal danger signs (AOR = 2.78; 95% CI: 1.63-4.73), decision-making power for taking sick neonates to health institution (AOR = 3.02, 95% CI: 1.61-5.67), mothers living with their partner (AOR = 3.00; 95% CI: 1.42-6.31), and health insurance (AOR = 1.82; 95% CI: 1.08-3.06) were significantly associated with having appropriate healthcare-seeking behavior. Healthcare-seeking behavior of the respondents’ was low and indicated by nearly 2 out of 5 respondents’ had appropriate health-seeking behavior for neonatal danger sign. Postnatal care follow-up, health insurance, good knowledge of neonatal danger signs, living with a partner, and decision-making power were predictors of appropriate healthcare-seeking behavior for neonatal danger signs. Emphasis should be given to creating awareness of neonatal danger signs, maintaining postnatal follow-up, and encouraging mothers/caregivers to make immediate decisions for seeking healthcare at healthcare institutions.
The proportion of mothers who sought care at health facilities for neonatal danger signs varied across the globe. In developing countries like Ethiopia, the absence of healthcare-seeking behavior among Ethiopian women causes a lack of early recognition of neonatal danger signs and hence neonatal death at home.
The finding from this study will be helping the policy maker responsible for making strategy to reduce neonatal death happens due to a lack of early care-seeking behavior.
The finding from this study will help the policymaker responsible for making strategies to reduce neonatal death due to a lack of early care-seeking behavior.
Introduction
Health care-seeking behavior is defined as any action undertaken by individuals who perceive themselves to have a health problem or to be ill to find an appropriate remedy. 1 Globally, the neonatal mortality rate is 17 deaths per 1000 live births or approximately 6700 deaths per year, while about 47% of all under-five deaths occurred in neonatal periods in 2019. Furthermore, the neonatal mortality rate was the highest in Sub-Saharan Africa (27 deaths per 1000 live births). 2 One of the third Sustainable development goal (SDG) aims was to end preventable deaths of newborns by 2030. 3 Also, all countries were aiming to reduce neonatal mortality to at least as low as 12 deaths per 1000 live births in 2030, but in Ethiopia, the neonatal mortality rate shows a slight increase from 29 death per 1000 live birth in 2016 to 30 deaths per live births in 2019.3,4
Delayed healthcare seeking contributes much for neonatal mortality. Because the majority of neonatal deaths occur at home, where a few families sought medical care for signs of neonatal illness, and nearly no neonates were taken to health facilities when they were sick. 5 Therefore, a family understanding of health care seeking is essential to minimize potential delays that contribute to neonatal mortality and effectively improve neonatal health. 6 Healthcare-seeking behavior for neonatal danger signs is essential in managing illness and preventing mortality in neonates. 7 Mothers’ and caregivers’ recognition of newborn disease (neonatal danger signs) at home was poor; and/or delayed due to different traditional beliefs or cultural beliefs related to ideas of what causes neonatal illness.5,6,8 -14
The proportion of mothers who sought care at the health facility for neonatal danger signs varied across the globe. For example, in Asia from 11.3% to 79.23% from 2006 to 2019.15,16 While 47.7% to 35.9% in Africa in 201517,18 and 27% to 97.7% from 2017 to 2020 in Ethiopia.14,19 -24 In a developing country like Ethiopia, the absence of healthcare-seeking behavior among Ethiopian women causes a lack of early recognition of neonatal danger signs, and hence neonatal death occurs at home. 5 Besides this, different studies reported that urban residence, maternal secondary education, the practice of optimal thermal care, place of delivery (institutional delivery) and postnatal care follow-up (having postnatal care follow-up), knowledge of neonatal illness, or danger signs were factors that significantly associated with health care seeking behavior.14,17,22,23
Recognition of why families were choosing to or not choose to seek health care was key while we are on the way to improving newborn/neonates’ health. 24 The model used in this study was the modified Anderson and Newman model that was first developed in the 1960s and has since gone through 4 phases. Andersen and Newman’s 1974 framework of health care services utilization states that individual access to and using health services is based on 3 characteristics. Such as predisposing, enabling, and need factors. 25 Determination of early maternal health care-seeking behaviors on neonatal danger signs and identifying the factors related to health care-seeking behavior for neonatal danger signs are essential for countries like Ethiopia.
In the study area, little is known about the status of healthcare-seeking behavior for neonatal danger signs and its associated factors among postpartum mothers. Thus, this study aimed to assess healthcare-seeking behavior for neonatal danger signs and associated factors among postpartum mothers in South East Ethiopia by using modified Anderson and Newman model for health service utilization.
Methods
Study Area
This study was conducted in Shashamane town Oromia, a regional state, which is located 251 km to the south of Addis Ababa, the capital of Ethiopia. There are 8 kebeles (the least administrative unit in Ethiopia) and 2 government hospitals (1 general and 1 comprehensive specialized hospital), 1 private hospital, 4 health centers, 71 medium private clinics, and 72 private pharmacies in the town. The total town population was 279 814 by 2020, of which 141 150 and 138 665 were males and females. Approximately, there are 12 216 total pregnant women by 2020 (Unpublished Shashamane Town health office’s data).
Study Design, Period, and Sampling Techniques
A community-based cross-sectional study design was employed to assess maternal health-seeking behavior for neonatal danger signs among postpartum mothers in Shashamane town from June 1st, 2020 to November 27th, 2020. The sample size was determined based on single population proportion formula by considering 41.3% the prevalence of healthcare-seeking behavior of postpartum mothers at Tenta district in 2015, 13 at 95% confidence level, 5% marginal error (d), and 10% non-response rate; the result was the sample size of 410. A simple random sampling technique was used to identify participants. For each 8 kebeles’, the list of postpartum mothers was prepared with their addresses using health extension workers’ data. The calculated sample size was proportionally distributed for each kebeles. Six thousand and one hundred eight (6108), the average number of postpartum mothers lived in the town within the last 6 months.
Population and Eligibility Criteria
All post-partum mothers at Shashamane town were source population. While postpartum mothers whose neonates had history of illnesses for at least 1 times within 28 days of their life in the study area were included in the study. Postpartum mothers who were not interested/not willing to participate in the study, unable to communicate due to severe illness, and who lost their bay at birth were excluded from the study.
Variables
Dependent variables
Health care seeking behavior (HCSB) is outcome variable for this study. HCSB was measured using structured interviewer administered tools and finally categorized into—“Have appropriate healthcare-seeking behavior” when participants sought care at health institution within the day they recognize signs and symptoms of diseases on their neonates’ otherwise “Inappropriate healthcare-seeking behavior.” 16
Independent variables
The independent variables are classified based on the Anderson and Newman Behavioral model classified into predisposing factors that consider the socio-cultural characteristics of individuals that exist before their illness. In addition, it considers social Structures like Education, marital, occupation, ethnicity, social networks, social interactions, and culture. From the health beliefs side, it includes values and knowledge of people toward the health care system. Under socio-demographic features, age and gender were included as predisposing factors; enabling Factors (the logistical aspects of obtaining care) were stated also as it includes some variables like means and knowledge of how to access health services, income, health insurance, regular source of care, travel, extent, and quality of social relationships and available health personnel and facilities, and waiting time.
Need factors are another factor that states perceived need was better to help to understand care seeking and adherence to a medical regime that includes perceived illness/self-reported illness (status and severity of diseases. In addition, health system factors (Distance of health facility, Perceived quality of services, Type of healthcare services) (Figure 1, S.1. Supplemental Material).15,25 -27

Conceptual frame for healthcare-seeking behavior (modified Anderson and Newman model).
Operational Definitions
Health care seeking behavior: Seeking care at health institution (from trained health professional) or (seek care from a traditional healer, spiritual healers and doesn’t took any were) in response to neonatal danger signs to reduce severity and complication after recognizing/identifying the danger signs and perceived nature of the illness. 14 In this study, if participants sought care at health institution within the day they recognize signs and symptoms of diseases on their neonate considered as “Have appropriate healthcare-seeking behavior,” otherwise “Inappropriate healthcare-seeking behavior.” 16
Have decision-making power (if participants make decision by herself and/or with her husband to get medical care and to select treatment place for their ill neonate). Have not decision-making power (if participants do not make decision by herself and/or with her husband to get medical care and to select treatment place for their ill infant). 14 Good knowledge of neonatal danger sings (if mothers were able to list more than 3 out of 9 WHO outlined neonatal danger signs). Poor knowledge of neonatal danger sings (if mothers were able to list at most 3 out of 9 WHO outlined (none of and/or ≤3) neonatal danger signs).17,28
Data Quality Control
A pretest was done in Arsi Negelle town on 5% (21) of the participants after the questionnaire was translated into the Afan Oromo language. According to the results of the pretest, further modification (reordering, rewriting, and regrouping) of the questionnaire was done before the actual data collection. Orientation was given to data collectors and supervisors. Collected data was reviewed and checked for completeness and relevance by supervisors on a daily base.
Data Collection Tool and Procedure
The questionnaire was prepared in English language and translated into the local language (Afan Oromo) and back to English languages to check the consistency. A structured interviewer-administered questionnaire adapted from different literature was used to collect the data.14,15,23,26,27 One MSc holder in clinical midwifery and researcher supervisor and 4 BSc midwives participated in the data collection process.
Data Processing and Analysis
The data were checked for completeness, consistencies, and missing values and then coded, and entered using Epi Data version 3.1. Then cleaned and exported to and analyzed using Statistical Package for Social Science (SPSS) version 26. 29 Descriptive statistics were computed to determine frequencies and summary statistics (mean, median, standard deviation, and percentage) to describe the study population concerning socio-demographic and other relevant variables. Data were presented using tables, graphs, and figures. Both binary and multivariate logistic regression was executed to see the association between independent and dependent variables. All explanatory variables with P < .25 in bivariate binary logistic regression were transferred to multivariate binary logistic regression analysis. Hosmer and Lemeshow’s model fitness test shows the data well fitted the model (P = .64). All statistical tests were two-tailed, and P < .05 used to declare the significance.
Results
Socio Demographic Characteristics of the Participants
From total sample size of 410, four hundred participants were successfully interviewed in this study giving a response rate of 97.6%. Among the study participants, 160 (40%) were in the age group of 25 to 29 years and the mean (±SD) age was 27.45 ± 5.02 years while the mean age (±SD) of the neonates was 17.9 ± 5.7 days.
About 326 (81.5%) of participants were living with their partner while 156 (39%) of study participants had secondary and above level of education. Two hundred seventy three (68.8%) of study participants were unemployed (Table 1).
Socio-Demographic Characteristics of Postpartum Mothers in Shashamane Town, Oromia, Ethiopia, 2020 (N = 400).

Includes mothers who were divorced, single, and widowed.
Includes mothers who were students, homemaker/house wife, farmer, and labor worker.
Health Service Uptake of the Study Participants
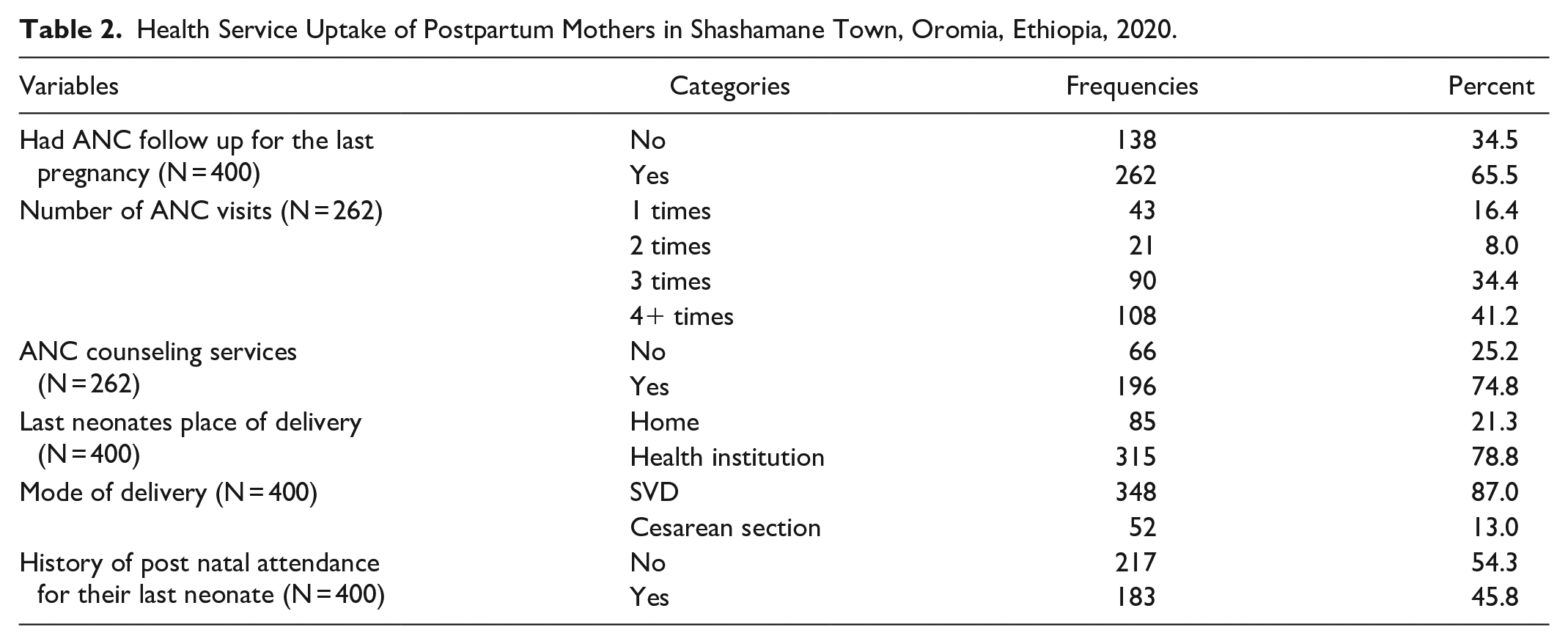
Nearly two third, 262 (65.5%) of study participants had antenatal care follow up for their last pregnancy. Spontaneous vaginal delivery (SVD) was the most 348 (87%) reported mode delivery by the study participants. One hundred eighty three (45.8%) of the study participants had history of postnatal follow up after the birth of their last neonates (Table 2).
Health Service Uptake of Postpartum Mothers in Shashamane Town, Oromia, Ethiopia, 2020.
Knowledge/Recognition of Neonatal Danger Signs by Respondents
From total study participants; nearly half 205 (51.3%) of participants have good knowledge of neonatal danger signs (able to mention more than 3 out of 9 WHO neonatal danger signs). About 222 (77.1%) neonatal danger sign mentioned by participants was unable/stop feeding/poor feeding (Table 3).
Knowledge and Types of Neonatal Danger Signs Mentioned by Postpartum Mothers About NDSs in Shashamane Town, Oromia, Ethiopia, 2020.

Magazines, Facebook, Telegram.
Health Care Seeking Behavior for Neonatal Danger Signs
From total 400 mothers whose neonates have got illnesses for at least once since their birth to 28 days of life; about 176 (44%, 95% CI: 39.2-48.9) of them have appropriate health care seeking behavior (sought care at health institution within a day they have seen symptoms on neonates). However, regarding place of care sought about 153 (38.5%) of the respondents were sought care at public or private hospitals while about 137 (34.3%) of them took their sick neonates to health center; but 32 (8%) of them sought care from private clinic regardless of time they sought care (Table 4).
Health Care Seeking Behavior Among Postpartum Mothers in Shashamane Town, Oromia, Ethiopia, 2020 (N = 400).

Non health facility includes traditional, spiritual healers, and mothers who didn’t seek any care. bHealth facility includes mothers who seek care at public/private hospital, health center, and private clinics.
Multiple responses.
About 303 (75.8%) of the respondents have decision-making power, however the major decision maker for health care seeking of their seek neonates were both mothers and fathers 223 (55.8%) (Figure 2).

Decision makers for seeking care for their sick neonate among postpartum mothers in Shashamane Town, Oromia Region, 2020 (N = 400).
Factors Associated With Health Care Seeking Behavior for Neonatal Danger Signs
Variables like knowledge of NDSs, health insurance, ANC follow-up for the last pregnancy, post-natal care follow-up, decision-making power, marital status, mother occupational status, average self-responded monthly income, last neonates place of delivery, last neonate birth order, educational status of mothers were included in the multivariable logistic regression model. However, having postnatal care follow-up, good knowledge of neonatal danger signs, decision-making power, living with a partner, and having health insurance were significantly associated with having appropriate healthcare-seeking behavior. Given that, postpartum mothers who have postnatal care follow-up were 3.5 times higher odds of having appropriate healthcare-seeking behavior than those who have no postnatal care follow-up (AOR = 3.5; 95% CI: 2.06-5.80). Similarly, postpartum mothers who have good knowledge of neonatal danger signs were 2.8 times more likely to have appropriate health care seeking behavior than those who have poor knowledge of neonatal danger signs (AOR = 2.78; 95% CI: 1.63-4.73).
Also postpartum mothers who have decision making power had 3.02 times higher odds of appropriate health care seeking behavior than those who have no decision making power (AOR = 3.02, 95% CI: 1.61-5.67). Moreover, postpartum mothers who were in marriage or ever live with their partner were 3 times higher odds of having appropriate health care seeking behavior than those who were out of marriage or live without their partner (AOR = 3.00; 95% CI: 1.42-6.31). Besides, postpartum mothers who have health insurance were 1.8 times higher odds of having appropriate health care seeking behavior than those who have no health insurance (AOR = 1.82; 95% CI: 1.08-3.06) (Table 5).
Factors Associated With Health Care Seeking Behavior of Postpartum Mothers for Neonatal Danger Signs at Shashamane Town, Oromia, Ethiopia, 2020.

Mothers who were divorced, widowed/not live with their partner.
Includes mothers who were students, homemaker/house wife, farmer, and labor worker.
P-value ≤.001. **P-value <.05.
Discussion
Maternal healthcare-seeking behavior for neonatal danger signs is essential in managing illness and preventing mortality in neonates since the majority of the mothers were caregivers of the neonate and/or newborn. 7 Mothers’ recognition of newborn, and/or neonatal danger signs at home was poor; and/or delayed due to low maternal educational level, knowledge of neonatal danger signs, different traditional beliefs or cultural beliefs related to ideas of what causes neonatal illness.5,6,8 -14 Therefore, this study assessed the maternal healthcare-seeking behavior for neonatal danger signs and associated factors among postpartum mothers in South East Ethiopia. It showed that 44% (95% CI: 39.2-48.9) of postpartum mothers had appropriate healthcare-seeking behavior.
This finding is consistent with the studies done in parts of Ethiopia 41.3%, 14 43.2%, 22 Nigeria (47.7%), 17 and India (41.8%). 10 However, it is higher than the other studies conducted in Ethiopia (27%, 19 32.0% 23 ), India (23%), 30 Nigeria (35.9%), 18 and Nepal (11.3%). 15 The possible reason for these differences in appropriate healthcare-seeking behavior might be due to the higher sample size in this study than the study done in Northern India and Western Nepal. Despite this; differences in postnatal care follow-up might be the reason; that is in the study done in Wolkite town majority (80%) of the respondents have no postnatal care follow-up for their last neonates; which restrains their chance of getting counseling on neonatal danger signs.21,23
The other possible difference might be the difference in the educational level of the study participants; which is the majority (86.8%) of study participants have no formal education in the study done in Anedid district. 19 This might be due to that the mothers who had formal education had more knowledge about neonatal danger signs, and where to seek care and when to seek care than those who had no formal education. 21 Besides, having good knowledge about neonatal danger signs were related to having appropriate health care seeking behavior. 23 Additionally, some socio-demographic factors like place of residence; in the previous studies except study in Wolkite town (include only town) 23 ; others include the rural part in which there is a constraint of health care seeking and the probability of utilizing and believing traditional health is higher than an urban community. 5
The current finding was lower than the study finding done in other parts of Ethiopia (83%, 31 72.7%, 32 81.2%, 33 52.3%, 34 97.1% 20 ) and Odisha (79.23%). 16 The possible differences might be due to differences in study setting (community-based vs health facility based); educational level; higher educational level/more than half of participants had secondary and above the educational level in the study done in Debre Markos; which is not in this study. However, in the study done in the urban slum of Bhubaneswar, Odisha; all participants were literate. Given that, a higher educational level is related to good knowledge of neonatal danger signs and health care seeking on time. 21 The other possible difference might be the difference in outcome variable definitions.
Another possible reason might be the difference in post-natal care follow-up (89%) of participants in the study done in Tiro Afeta while about 45.8% in this study) which in turn helped the participants to have a chance of counseling about neonatal danger signs and health care seeking. Similarly, the difference in antenatal care follow-up might be the possible reason. Supported, the Majority (more than 88%) of the study participants in the study done in Bahir Dar and Fiche town had antenatal care follow up. This might give them a high possibility of getting counseling on neonatal danger signs, and having antenatal care follow-up was related to having good knowledge of neonatal danger signs.23,34 The other possible reason might be due to the higher sample size noted in the study done in Dire Dawa and the difference in the outcome variable definition.
This study also found that having postnatal care follow-up was a strong predictor of having appropriate healthcare-seeking behavior. This might be due to the opportunity of postnatal counseling on newborn illness (neonatal danger signs) that can improve the mother’s knowledge and attitude on the neonatal danger signs, in which knowledge of neonatal danger signs is the entry point for healthcare-seeking behavior. Similar to this study finding, a study in Wolkite town and Fiche town found that having postnatal attendance showed a significant association with having appropriate healthcare-seeking behavior for neonatal danger signs.23,34
Besides this, in the current study, having good knowledge of neonatal danger signs was significantly associated with having appropriate healthcare-seeking behavior. Similarly, studies in Ethiopia and Nigeria showed that knowledge of neonatal danger signs indicates a strong association with having appropriate healthcare-seeking behavior.17,22 This might be because having good knowledge of neonatal danger signs helps mothers to decide where to seek care and when to seek healthcare. 35
This study also revealed that postpartum mothers who have decision-making power were more likely to have appropriate healthcare-seeking behavior than their counterparts were. Similarly, a study in Debretabor and Tenta district found that maternal autonomy to decide on health care seeking was associated with health care seeking behavior.14,35 This is supported, with that, autonomous mothers were more likely to have good knowledge of neonatal danger signs, and autonomous mothers, were expected to influence their husbands to seek care early. 35
This study also showed that having health insurance indicates an association with having appropriate healthcare-seeking behavior. This might give them the chance to get counseling on neonatal danger signs that help them in health care-seeking neonates. 36 Furthermore, this might be because mothers who have health insurance were more likely to utilize maternal and child health services. 37
Besides, living in marriage/living with their partner was also significantly associated with having appropriate healthcare-seeking behavior. The possible reason for this association might be due to partners actively involved in maternal antenatal care follow-up, facility delivery, and postnatal follow-up associated with maternal knowledge of neonatal danger signs, in which knowledge of neonatal danger signs is the critical point for having healthcare-seeking behavior. 38
Limitation of the Study
This study is not out of limitation; variables like the perception of mothers, service quality, and severity of illness, not assessed in detail in this study; because it might be difficult to extract maternal and family perception, believes, understanding, and reason regarding the health care seeking behavior at a point of time. Additionally, health professionals or health institution factors like, quality of health services, health facility accessibility and functionality did not studied in detail since that might need qualitative and quantitative study.
Conclusion
The overall health care seeking behavior in this study was low. Having postnatal care follow up, having health insurance, living with partner/in marriage, having decision making power about where, when, and how to seeking care for their sick neonates, and good knowledge of neonatal danger signs were factors having a statistically significant association with having good health care seeking behavior.
Emphasis should be given in creating awareness toward neonatal danger signs, maintaining postnatal follow-up, and immediate decision making for seeking health-care at health institutions, encourage partner accompanies and health care providers on counseling more on the importance of postnatal follow-up and health care seeking at health institutions was recommended in general. Creating women’s/families’ awareness through religious leader (whom they trust more), women campaigns, increasing counseling at ANC, family planning, and labor and post natal wards for women there for the services at each wards. Similarly counseling or creating awareness about neonatal danger signs should be considered before, during, and after pregnancy time. In addition to this, further study (qualitative) that will study maternal perception, believes toward neonatal danger signs, and attitude recommended.
Supplemental Material
sj-docx-1-inq-10.1177_00469580221143629 – Supplemental material for Maternal Health Care Seeking Behavior for Neonatal Danger Signs and Associated Factors Among Post-Partum Mothers in Southeast Ethiopia: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580221143629 for Maternal Health Care Seeking Behavior for Neonatal Danger Signs and Associated Factors Among Post-Partum Mothers in Southeast Ethiopia: A Cross-Sectional Study by Degefa Gomora Tesfaye, Girma Geta, Chala Kene, Kenbon Seyoum, Yohannes Tekalegn, Fikreab Desta, Biniyam Sahiledengle, Daniel Atlaw, Neway Ejigu and Wogene Negash in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
First and for most I would like to thank the almighty God for giving me this chapter of my life and help me for conducting this research. Secondly, I would like to express my gratitude to Hawassa University for funding this study. Next to this, I would like to thank my friends for their greatest suggestions and support throughout this thesis work. Lastly, but not least my heartfelt thanks goes for Shashamane town health office and study participants.
List of Abbreviation and Acronyms
ANC: Antenatal Care; AOR: Adjusted Odds Ratio; CD: Cesarean Delivery; CI: Confidence Interval; COR: Crude Odds Ratio; EMDHS: Ethiopian Mini Demographic Health Survey; ETB: Ethiopian Birr.; EHSTP: Ethiopian Health Sector Transformation Plan; HI: Health Institution; NDSs: Neonatal Danger Signs; PMTCT: Prevention of Mather To Child Transmission; PNC: Post Natal Care; SDG: Sustainable Development Goal; SVD: Spontaneous Vaginal Delivery; UNICEF: United Nations Children’s Fund; SPSS: Statistical Package for Social Science; WHO: World Health Organization.
Authors’ Contributions
All authors (DG, GG, CK, KS, YT, FD, BS, DA, NE, and WN) has made substantial contribution in the conception, study design, execution, and acquisition of data, analysis, and interpretation; took part in drafting and revising the article critically for intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
Hawassa University institutional review board (IRB) approved the research and gave approval letter (IRB/094/12). A formal letter of cooperation obtained from Hawassa University Department of Midwifery to Shashamane town health bureau. A support letter obtained from the Shashamane town health bureau to each Kebeles in Shashamane town. Informed verbal consent obtained from all study participants by reading the written Informed consent form, before starting the interview. All the study participants were assured that the data was anonymous, informed about the purpose of the study, the variety of information needed from them and they can refuse/stop.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.