
Abstract
Pregnancy and parenting in adolescence and the transition home following the hospitalization of an infant in the neonatal intensive care unit (NICU) are two relatively complex phenomena; and whilst each have been consistently explored within the relevant literature, little is understood about the care required when they intersect. Using interpretive description methodology to guide our exploration, we conducted semi-structured interviews with 23 expert providers caring for adolescent parents involved in NICU-to-home transitions to describe this process in their practice. Findings suggest that supporting successful NICU-to-home transitions for adolescent parents relied strongly on understanding the impact of the NICU experience, establishing therapeutic relationships and facilitating supportive partnerships between the NICU and parents as well as the NICU and supportive services post-discharge. Findings highlight the opportunity for more integrated models of care within the NICU and extending into the community to address the complex biopsychosocial care needs of this parent population.
Keywords
Background
Adolescent Parents and the Neonatal Intensive Care Unit
Experiences of pregnancy and parenting in adolescence are associated with maternal factors including lower educational attainment, housing instability, exposure to violence (Al-Sahab et al., 2012), adverse childhood experiences (ACEs) (Hillis et al., 2004; Smith et al., 2018), mental health disorders (Vigod et al., 2014), and higher rates of smoking and substance use (Fleming et al., 2015). Furthermore, this constellation of factors contributes to poorer health and social outcomes among adolescent women and their children, with social determinants of health inequities more likely at the root of negative outcomes than maternal age alone (SmithBattle & Leonard, 2012). However, even when controlling for significant sociodemographic factors, infants born to adolescent mothers (age<20 years) are at an increased risk for preterm birth, low birth weight and congenital anomalies, making these infants more likely to require hospitalization in a neonatal intensive care unit (NICU) shortly after birth (DeMarco et al., 2021; Shrim et al., 2011).
The experience of a critically ill infant in the NICU environment is a frequent source of stress, anxiety, depression and grief; with subsequent need for increased social and professional support for all-aged parents (Caporali et al., 2020; Hynan et al., 2015; Soghier et al., 2020). Additionally, these emotional and psychological outcomes are pervasive and continue well beyond the infant’s discharge from the NICU; with studies reporting ill-effects up to 7 years post-discharge (Beck & Woynar, 2017; Treyvaud et al., 2014). For adolescent parents, these emotional and psychological outcomes associated with the NICU experience intersect with the social, psychological and economic difficulties associated with adolescent parenthood. Therefore, for an adolescent parent, admission of their infant to the NICU exacerbates an already complex situation.
Care in the NICU and beyond post-discharge that is safe, equitable and acceptable for adolescents can be realized by understanding what it means to provide adolescent-friendly care (World Health Organization [WHO], 2012). Whilst community-based and primary care programs have implemented services based on the principles of adolescent-friendly care for the prenatal period, little is known about the provision of adolescent-friendly, hospital-based perinatal care, including within the NICU (Daley et al., 2013; Peterson et al., 2012; Rosenstock & van Manen, 2014). Additionally, adolescent-friendly care for adolescent parents in the perinatal hospital environment is often learnt through provider reflections informed through their personal or professional experiences versus formal adolescent-friendly training experiences (Quosdorf et al., 2020). This lack of consistent adolescent-focused training among providers in perinatal hospital settings could lead to care and services that feel unsafe for adolescent parents and unable to meet their unique needs.
Individuals less than 20 years of age make up approximately 15% of the NICU parent population (de Jongh et al., 2012; Walsh & Goser, 2013) and whilst perspectives related to adult-aged parents in the NICU are well documented (Al Maghaireh et al., 2016), adolescent parenting within the context of the NICU remains poorly understood. This gap in the knowledge base was highlighted in a review by Rosenstock and van Manen (2014); with little addition to the literature since this review was completed. Important to the context of this study, the lack of adolescent-focused literature is most profound when seeking to understand how to support successful transitions from hospital-to-home and community following an NICU stay.
Transition Home from Neonatal Intensive Care Unit
In general, transition to home post-NICU discharge has been explored within the health literature. These studies range in focus from preparing for or facilitating discharge among infant/parent dyads (Boykova, 2016; Lopez et al., 2012); describing the development, implementation and evaluation of discharge programs or interventions (Brodsgaard et al., 2015; Garfield et al., 2016; Toral-Lopez et al., 2016), and documenting parental perspectives, experiences, or emotional responses related to discharge and transition-home both qualitatively and quantitatively (Aydon et al., 2018; Enlow et al., 2014; White et al., 2017). Adolescent parents, however, are not the focus of these discussions; additionally, many of the participants in these studies are significantly older than the adolescent age-group. So, whilst it is possible to apply adult-focused findings to the adolescent population, failure to consider the unique developmental stage of the adolescent parent and the relative complexity of their pregnancy and parenting situation could lead to care that is un-informed and unable to meet their needs and the needs of their infant.
Another limitation of the NICU-to-home transition literature is the principal focus on the situational transition of hospital-to-home; without considering other transitions that overlap and intersect with this transition (Orr et al., 2020). Meleis’ middle-range Transitions Theory helps both researchers and practitioners understand that transitions are periods characterized by uncertainty and disconnectedness, where there are losses of networks and social supports, and therefore individuals experiencing transitions are in a vulnerable state and often require intervention to facilitate healthy transition and enhance healthy outcomes following transitions (Meleis, 2010). Significantly, Transitions Theory describes four types of transitions: (a) developmental (e.g. becoming a parent); (b) situational (e.g. discharge from hospital); (c) health-illness (e.g. illness recovery) and (d) organizational (e.g. structural reorganization) (Schumacher & Meleis, 1994). Recognizing the diversity of transition-related circumstances, and as these types of transitions are not mutually exclusive, the theory emphasizes the added complexity of multiple transitions occurring simultaneously (Meleis et al., 2000). Thus, the transitions of adolescent parents with infants discharged home from the NICU are an example of this complexity; whilst navigating the situational transition of coming home from the NICU, an adolescent parent is simultaneously experiencing the developmental transition to parenthood; the health-illness transition of parenting an infant with complex health needs and/or risk for developmental delay; all within the context of the dynamic and multifaceted developmental transition to adulthood (Orr et al., 2020).
Problem, Purpose and Research Question
The unique social, psychological and developmental contexts in which parenting in adolescence occurs, combined with the complexity of NICU-to-home care transitions, underscores the need for an age-specific understanding of these experiences and supportive care needs post-discharge that is not currently explored in the relevant literature. This understanding could inform practices and policies, beginning in the NICU and continuing beyond the acute care setting, to address the complex biopsychosocial care needs of this unique group of parent/infant dyads and to ensure focused and holistic care. Therefore, as part of understanding this complex phenomenon, we explored how providers caring for adolescent parents involved in NICU-to-home transitions viewed this process in their practice. We asked what can be learnt from providers’ perspectives about transitions from NICU-to-home for adolescent parents and what is the provider’s role in supporting successful transitions?
The provider perspective in applied health research acknowledges that expert practitioners are a significant source of qualitative data related to a particular phenomenon (e.g. a health issue or a disease state) on account of their own professional experiences over time observing, working with or providing care to multiple individuals (e.g. clients, patients, parents) with that specific phenomenon of interest (Thorne, 2016). As researchers and clinicians, we acknowledge the importance of adolescent parents’ experiences in understanding NICU-to-home transitions and data collection from the parent perspective is currently ongoing and will be triangulated with the provider data to further understanding in this field.
Methods
Interpretive description is an applied qualitative research design that aligns with the disciplinary knowledge requirements and pragmatic research aims of the applied health professions (Thorne, 2016). This design emphasizes research questions that are clinically relevant and findings that are application ready, versus those that are too abstract or theoretical to be meaningful, and as such the approach was well suited to guide the methodological decisions for this study. This approach also supports the collection of data from provider participants, as it highlights the role of thoughtful clinicians as rich sources of qualitative data for applied health research. Specifically, the perspectives of clinical experts can offer experiential diversity or variation from having seen multiple cases of a phenomenon over time (Thorne, 2020).
Interpretive description design does not necessitate the adoption of extant theoretical frameworks for the positioning of research work and instead uses the knowledge needs of the intended audience to guide the design logic of the project (Thorne et al., 2018). The theoretical forestructure guiding this study design and implementation included leading nursing theories as well as developmental theory related to transitions, parenting and adolescence (see Orr et al., 2020). A nursing disciplinary orientation – in particular, a holistic view of individual, family and community health and a broad understanding of transitions beyond the situational – also contributed to the scaffolding of this study in framing the research questions, participant recruitment, data collection and analysis.
Recruitment
Following ethical approval from the Hamilton Integrated Research Ethics Board (HiREB # 5089) and scientific approval from partnering Public Health Units (PHU), we recruited providers involved in the transition experience of adolescent parents. Recruitment partnerships were established at seven sites; four NICUs located in southern Ontario, Canada and three PHUs covering the same geographic area. Partners distributed recruitment emails to relevant team members; interested participants then received a direct email invitation from the Principal Investigator (EO). The study was also presented at both NICU and PHU research rounds with a recruitment invitation following the rounds. A process of snowball sampling elicited referrals from study participants, who, with permission, were contacted by the Principal Investigator with an email invitation to participate in the study. Participants were assigned a unique study identification number and transcripts were cleared of any personal or organizational identifiers to protect anonymity.
Study Participants
To represent provider perspectives across the hospital-to-home transition continuum, the intended participants for this study were interprofessional team members involved in the care of adolescent parents and their infants both in NICU and community settings. To allow for a broad range of perspectives based on discipline, role, and practice setting, specific criteria for inclusion were not prescribed. Providers were included if they self-identified as a health care or social care provider having had experience supporting adolescent parents with an infant in the NICU. Findings for this study are grounded in the professional experiences of 23 health care and social care providers. Of these 23 participants, the majority were registered nurses (RN) (n = 18) and nurse practitioners (NP) (n = 3); two participants were social workers (SW). Participants represented both the NICU setting (n = 7; level II and III NICUs) and the community or outpatient setting (n = 14; public health programs or neonatal follow-up clinics) and two participants had experience working in both NICU and community settings. Most providers were from southern Ontario; however, other regions of Ontario and Canada were represented. All participants were women and had at least 2 years of practice experience; with four providers having over 30 years of clinical expertise (mean, 17 years; standard deviation, 8.9 years; range, 2–31 years). About three-quarters of the participants (n = 16) held a bachelor’s degree and the remaining participants held master’s degrees. Partial demographic data was missing for one participant.
Participants represented two groups based on recruitment and data collection strategies; 17 were recruited and interviewed for the sole purpose of this study, whilst six additional participants were part of a purposeful extension of the sample to include public health nurse (PHN) participants from the British Columbia Healthy Connections Project (BCHCP) process evaluation (Jack et al., 2015). In the BCHCP study, PHNs delivering the Nurse-Family Partnership® (NFP) – a targeted public health intervention program aimed at improving maternal-child health outcomes for young pregnant and parenting adolescent girls and young women through nurse home visiting (Olds, 2006) – were interviewed eight times between 2014 and 2018. As co-authors of this study (AG & SJ) were also lead investigators of the BCHCP process evaluation, questions related to nurses’ experiences of providing care for clients who experienced hospitalization of their infant were purposefully added to the seventh cycle of one-to-one PHN interviews to provide additional data for this study reported here.
Data Collection
Individual, semi-structured interviews were used as our data collection approach. Written informed consent was collected prior to the scheduled interview, with a verbal confirmation of consent conducted prior to commencement of questioning. Interviews were scheduled at a mutually convenient time and were conducted in-person (n = 2) or by telephone interview (n = 15). Researcher field notes were recorded following the interviews and included relevant contextual information as well as initial analytic impressions. Participants received CAD$15 gift cards as a token of appreciation.
Interviews ranged from 30 to 65 minutes in length, and all were digitally recorded and transcribed verbatim. A semi-structured interview guide was developed to guide the direction of the interview (see Supplementary File); however, most participants reflected freely on their experiences supporting adolescent parents both in the NICU and the community, touching on the challenges encountered by providers as well as the perceived challenges to parents with little prompting.
Six nurses from the BCHCP process evaluation (of the 12 interviewed) spoke to the experience of supporting a client with a hospitalized infant; these transcripts were included in this study to further extend the understanding of this type of support for vulnerable young parents whilst in the NICU and in transition home.
Data Analysis
We used a concurrent data collection and analysis approach, with data analysis commencing following completion of the first interview. This approach informed the recruitment of participants practicing in specific roles related to the NICU-to-home transitions, (e.g. nurses who practice both in the NICU and the community and hospital-based public health liaison nurses). Consistent with interpretive description, the analytic process was inductive and began with immersion in the data set (transcripts were cleaned by listening to the audio recording, then transcripts were read and re-read to fully familiarize oneself with the data). A constant comparative analytic approach was then applied, comparing similarities and differences both within and across cases; with the intent of our applied research question remaining at the forefront (Thorne, 2016). Developing patterns were defined, described and challenged in analytic memos and relationships between patterns were explored through a process of diagramming (Campbell et al., 2021; Terry et al., 2017; Thorne, 2016). Primary analysis was completed independently by (EO), however, a sample of transcripts were reviewed and discussed among team members (MB, AG & SJ), and developing patterns were discussed as a research team throughout the analytic process.
Findings
Providers interviewed for this study offered critical insights into the NICU-to-home transition experience for adolescent parents. Their ability to reflect on how their own practice, as well as how different contexts of care might influence parents’ experiences both in the NICU and the community, displayed a deep level of compassion and concern for this population. What we learnt from providers, regardless of where they encountered young parents along the NICU-to-home continuum, was that their overall aim was to keep their patients/clients moving forward – whether in health or broader life course goals – throughout the NICU hospitalization and beyond discharge. Thus, our findings are structured in such a way that we first highlight the providers’ goal of successful NICU-to-home transitions for adolescent parents or mobilizing forward, then we illustrate each of the three patterns from our analysis that support this overarching goal: understanding impact, establishing therapeutic relationships and facilitating supportive partnerships. Finally, we explore the influence of NICU, home and community contextual factors related to successful NICU-to-home transition. Mobilizing forward is depicted in Figure 1 and illustrates the relationships between the described patterns as well as the overall directionality of our findings. Mobilizing forward.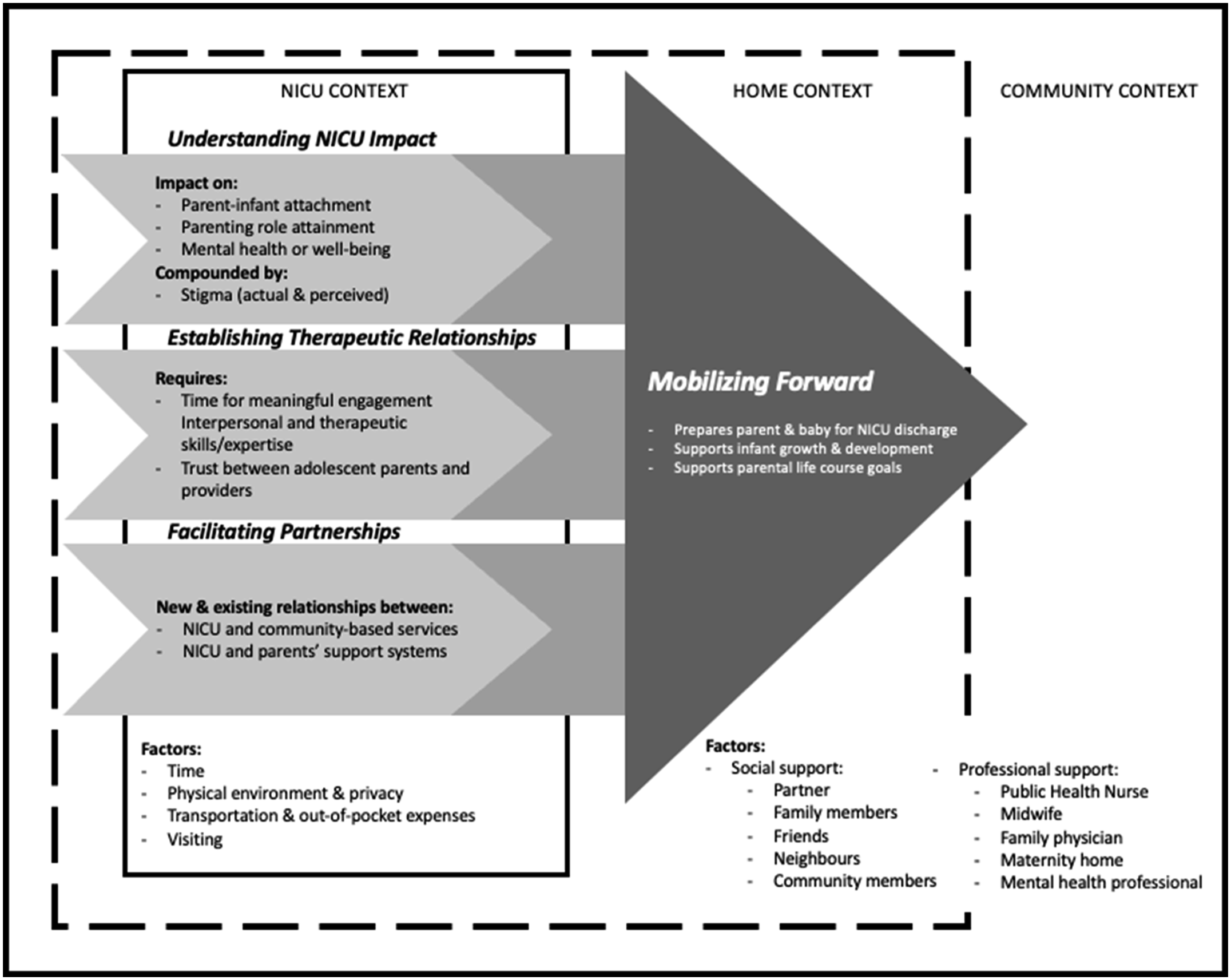
Mobilizing Forward
Providers consistently spoke to their role in supporting the transitions from NICU-to-home and community for the adolescent parents they cared for. The overarching goal across the providers’ accounts was ‘mobilizing forward’, or making progress toward certain health and life goals for both parent and infant. For the NICU nurse, these goals were often connected to the health or stability of the infant in relation to readiness for discharge from the NICU, for example achieving a goal weight for the infant, establishing a specific feeding method or intake volume. Mobilizing forward from this perspective was also associated with the ability of the parent to care for their infant. Whilst NICU nurses did not ignore the importance of safe and supportive home environments prior to discharge from the NICU, ensuring these were in place was primarily the role of the NICU social worker. For example this NICU social worker explained the importance of ensuring social support for adolescent parents as discharge from the NICU approached: To make sure that they have the supports when they leave right ... so they have a good support system at home and in the community who can assist them moving forward. Especially in the home. Right. Or close to the home. And if they’re living on their own. You know ‘who is going to be living in the house with you? Who’s going to be supporting you? Who’s going to be assisting you?’ Kind of talking to them about postpartum and isolation and moving them toward understanding that you kind of need to have a support system to move forward.
The variances in what mobilizing forward looked like to providers or how this was achieved were not just appreciated across disciplinary perspectives (i.e. between nursing and social work); nurses in distinct roles or programs also described this overall goal differently. For example PHNs and nurses involved care post-NICU discharge (e.g. neurodevelopmental follow-up) had a broader and more long-term perspective of successful transitions when compared to NICU nurses. These nurses were concerned with outcomes including growth and development for infants and general health and life course markers for parents. One PHN, who worked in a home visiting program, explained So, we care about [parents] too, so getting them mobilized with their schooling, their work, whatever they need is really important for their mental health, and for everything. Right? So, we really work on their parenting skills, obviously. Right? But also getting mom mobilized so she can move on with life and get out of that cycle of poverty.
These distinctions underscored an important characteristic of mobilizing forward, that it was multifaceted and involved the consideration of a variety of complex aspects to be successful, including infant health, growth and development, parenting capacity, social and economic support, and general life course factors. What also became apparent across the analysis of this pattern, was that the success of mobilizing forward relied on specific actions taken by health and social care providers both in NICU and community settings. These actions included understanding the impact of the NICU experience for adolescent parents, establishing therapeutic relationships with these patients/clients, and facilitating supportive partnerships that connected the NICU with the home and community. These actions, and how they support mobilizing forward, will be considered in follow paragraphs.
Understanding Parental Impact
Providers consistently raised the issue of the profound, and predominantly negative, impact of the NICU hospitalization for adolescent parents; so much so, that a separate analysis describing how the NICU environment is thought to influence the care and supports provided to adolescent parents was warranted (Orr, 2021) . Providers described a stay in the NICU as ‘a traumatic experience’ for parents. Based on their extensive experiences, providers spoke specifically to the impact of the NICU environment and the overall hospitalization experience on attachment, confidence and competence in the parenting role, and mental health or well-being. These impacts were in addition to, or in some cases compounded by, experiences of actual or perceived judgement or stigma from the care team as well as others within NICU (including other families and visitors).
Understanding Parental Impact for Mobilizing Forward
From the providers’ perspective, the hospitalization of one’s infant in the NICU is such a profound experience that mobilizing forward required an acknowledgement of this impact for support to be effective, as this provider summarized, ‘these [parents], they recognize, and they see somebody that supported them in a really tough time'. Community providers also spoke to the impact on the parents’ mental health post-NICU, in particular the anxiety felt related to the infant’s well-being. They also described the impact on the development of parenting skills and confidence as well as bonding with their infant beyond the NICU stay: Well, I think it affected their confidence in terms of their own abilities to take care of these little babies. Because I think these young women already struggle with that and are judged by so many random people just by you know their look and their age. And I think in some part it affects their bond or their attachment with their babies from the beginning.
Providers also recognized the need to tailor their support in such a way that accounted for the impact of the NICU. A PHN described this kind of tailoring: And then parents get really fixed on the routine of being in the NICU. Right. So, they’re feeding every 3 hours, you know. You know, they’re used to looking at their vitals all the time and, you know, anticipating a spell. So then when they do go home, especially when I do see a family that had a baby in the NICU and had that public health experience like a home visit. You know, they’re really fixed on that routine still. So, when they’re home and the babies now doing really well and, you know, you’re trying to normalize the care that they’re doing at home.
We learnt that providers also rely on strong therapeutic relationships to mitigate the impact of the NICU experience. However, these relationships were often difficult to establish, particularly with adolescent parents.
Establishing Therapeutic Relationships
There was a pattern across providers’ descriptions of supporting the NICU-to-home transition that highlighted the importance of establishing therapeutic relationships with parents; a process that required both time and skill and centred around trust. Many providers, from both the NICU and community, described the increased length of time it took to establish a therapeutic relationship with an adolescent parent; something that NICU providers felt could not always be prioritized above the tasks of providing physical care to critically-ill infants, as this NICU nurse described Sometimes you’re so busy, you don't necessarily have, you know, maybe the half hour that she needs to sit and talk, because if you’ve got three babies and they’re due [to feed] every two hours, like you’re on your feet the entire time.
Different factors supported developing skill or expertise engaging with adolescent parents. Public health nurses often reflected on specific training, such as motivational interviewing or trauma- and violence-informed care that became part of their practice and ability to connect with their clients. The skill of establishing therapeutic relationships was also seen as developing with practice over time: So, I really know that vulnerable client and how to engage them …I really make sure it’s trauma informed, too … that’s really important because some of these [parents] have ... for being so young, have such traumatic histories, with sexual assaults ... so much trauma. Right. And I think it’s just nice to have like been around.
It is possible that these skills may be lost or undervalued in the high-tech, fast-paced, medically focused environment of the NICU. Alternatively, NICU nurses are skilled at working within an interprofessional team and have the resources, such as social workers, available when their own comfort or skill with adolescent parents may be limited. Having someone else on the team with the skills to connect more easily with adolescent parents and provide psychosocial care may contribute to NICU nurses perceiving this type of care as not within their role: I think it’s sort of perceived as not being an ICU nurse’s job in a way. I also think we don't necessarily ... there might be a discomfort among nurses in engaging in that kind of conversation or care because maybe we feel like we don't know how ... so maybe people feel like they don't know how to ask families in that situation what they need, how we can help them. Maybe there’s also a lack of understanding about what is out there to help serve these families ... like in the community. But I do think it’s a little bit of ‘oh that’s not my job’, you know?
The difficulty with leaving the more challenging therapeutic relationships to other interprofessional team members, such as social workers, is that nurses in this context are then unable to develop or practice these interpersonal skills themselves. Where encouraging strong interpersonal skills, across all team members, could decrease the discomfort providers feel when working with parents and families that are more challenging to engage in a therapeutic relationship. Consequently, as providers become more comfortable with these interpersonal skills, the perception of judgement by NICU staff on behalf of adolescent parents may be relieved as they witness being treated similarly as adult-aged parents.
Trust was seen as central to establishing any therapeutic relationship, but no single element was perceived as more vital than trust when providing care specifically to adolescent parents: Honestly, I think that [trust is] one of the most important things that can happen, because I think we see the effect when it doesn’t happen. [If trust is not established], I think it really feels like you’re working upstream the rest of the time … I think that’s really essential, especially for a young parent who may already have experienced, who knows, comments through the pregnancy or a sense from others that this was not a good thing, that they were expecting a baby.
This account from an NICU nurse also highlights, as discussed prior, that establishing trust can be difficult to operationalize in the NICU context where adolescent parents may feel judged, stigmatized or even traumatized by the experience. From one PHN’s perspective, adolescent parents viewed the NICU as a ‘hostile environment’ and parents had to enter the ‘nurses’ house’ to be with their baby – when compared to the home visiting context where the nurse is a guest in the young person’s home and trust can be established more easily related to this more balanced relationship.
A significant barrier to establishing therapeutic relationships, in either context, was the parents’ past relationships with child protection services or the perception that letting a care provider engage in a therapeutic relationship was only for the purpose of reporting to child protection. Whilst not exclusive to the role, NICU social workers spoke specifically to this challenge: lots of times there’s that barrier of that defensiveness sometimes of ‘why are you talking with me’ and ‘are you just here because you are thinking I’m not capable to take care of this baby?’ And so, getting over that hurdle and normalizing things that ‘I’m here as a social worker here, a hospital social worker to provide you with support during your baby hospital stay just like I am for that baby in the bed next to you’. And, not making it about the fact that I’m seeing you because you’re an 18-year-old mom. I’m seeing you because you are a mom who’s had a baby who needs to be in special care nursery.
Some providers were able to skillfully navigate this and other barriers, whilst others felt that despite their best efforts, they were unable to connect with some parents; leaving the providers worried about the consequences of the inability to engage with an adolescent parent, ‘so I think my challenge too is not having a ... the ability to have a better relationship with them and often, as they leave, [I]think, oh, my heavens, I hope their family doctor is on top them'.
Establishing Therapeutic Relationships for Mobilizing Forward
The ability to connect on a therapeutic level with adolescent parents was also seen as essential to mobilizing forward. From the providers’ perspective, trusting therapeutic relationships moved young parents forward in their health and life journeys because they felt supported in their NICU experience: We’re there to care for all of them, not to take away control of their baby’s care from them. I think that’s really essential, especially for a young parent who may already have experienced, who knows, comments through the pregnancy or a sense from others that this was not a good thing, that they were expecting a baby. I think we have to work extra hard in those situations to develop that rapport.
Additionally, providers believed that adolescent parents remained engaged in supportive programs and services post-NICU when they trusted the individuals connecting with them, ‘I think building a trusting, supportive, therapeutic relationship with [adolescent parents] is really, really important to engaging them and to help them want us to come back right?’
Strong therapeutic relationships with understanding of the impact of the NICU experience contributed to mobilizing forward and NICU-to-home transition success. However, these actions or this process was made easier when there was an effort to establish new relationships, or foster existing ones, with the aim of supporting adolescent parents in the NICU and beyond post-discharge.
Facilitating Supportive Partnerships
A third pattern across the providers’ perspectives was that parents, and especially adolescent parents, faced several challenges during the transition home that pointed to a system that is disconnected, with numerous potential gaps that place the young family at risk of poor health and social outcomes. Recognizing and marshalling existing supportive relationships or facilitating new partnerships – that bridged the NICU and home/community divide – were seen as important in closing these gaps and supporting NICU-to-home transition success.
The need for partnerships was particularly clear as providers described the NICU discharge process or the context in which NICU discharges took place. Discharges were described as happening very quickly and were often accompanied by the pressure of managing other patients or overall unit bed-flow; new admissions would regularly drive the need for more stable patients to be discharged or transferred to a lower level of care. An NICU RN described this pressure and how ensuring parents were prepared for discharge became less of a priority within this context of competing demands: We had 72 [infants] for 68 beds last week … So how do you have time to adequately prepare a young adolescent mom and potentially her partner for discharge when you’re putting out fires left, right and center, like you just need to get them out … if they’re going home, make sure they have the referrals if they need them and then ‘bye’. ‘You have a car seat - cool - see ya’. It’s awful. But that’s what happens.
Perspectives surrounding discharge, however, represented a large amount of variation in our analysis; with some providers speaking to a more organized and supportive discharge process. These accounts predominantly represented units designated for infants with less intensive care needs and included extra time ‘rooming-in’ (round the clock care by parents in preparation for home) for adolescent parents and referrals to supportive services in the community. However, a provider with experience in a regional NICU follow-up clinic setting noted significant variation across the numerous NICUs served regarding their discharge preparation processes: I’m not bashing [the NICUs]; it is just their resources and their focus ... But, you know, a baby that comes home from one level II community nursery [compared to a baby that comes to follow-up] from another ... there’s huge variations in what their focus at discharge is.
The void of established pathways and/or therapeutic partnerships between NICU and community-based providers such as PHNs was evident in NICU providers’ expressed sentiments of ‘hoping for the best’; as if there was no way of knowing if these families would succeed once discharged and that they were being released into an unknown system where there is just ‘hope’ that families, especially those from marginalized groups – including adolescent parents, would be able to navigate successfully: Because honestly, I don't know how [the adolescent parents] do when they get home. We just hope that things go well for them and we never hear from them again. And you just hope that everything that they’ve learned when they were in the hospital, they’re able to manage it at home.
Similarly, another provider shared: So, I think a lot of it’s kind of like, you know, tell them what they need to know to get through these next four days and then the doctor will tell them everything. And probably not ... they probably go to their doctor for their well-baby [check-up] or whatever checkup and the doctor’s like ‘Okay, great. Yeah. So all’s well.’ And they still go home with no answers and no idea what they’re doing ... and it’s a little bit scary.
In contrast, when describing an NICU discharge that went well for her adolescent parent client, this PHN emphasized the importance of partnering with community providers early and throughout the discharge planning process. In this case the PHN was brought into the NICU circle of care to help prepare her young client for discharge: I just had one that was discharged from NICU and we had a beautiful discharge conference, right? With [child protection services] and with the father of the baby and his mother, the client and her mother, and myself, everybody was there. So, I asked a lot of questions about, about the feeding, the preparation of the formula ... and all that kind of stuff. So that really helps when we are transitioning them. So, we know what to look forward to as far as whatever the concerns they had in NICU.
However, when probed about other experiences supporting clients in the NICU, this partnership between NICU and public health was more of an exception rather than a normal occurrence; a response that was echoed by other community providers. One PHN expressed that if the NICU staff were provided with inter-agency opportunities to learn more about public health nursing roles and services provided to their more vulnerable parents, that partnerships could be facilitated in the future – despite seeming unrealistic: [Speaking to relationships between NICU and NFP] Realistically, I know that would never happen, but I think it’s a nice thought. I know like even for me going between the two, like public health and hospital, I still get jabs from everyone saying, ‘hey, you’re not a real nurse, you have the cushy job’. So, they’re not keen on public health to begin with. But I don't know ... I think honestly, more education surrounding these young moms, the higher risk and nature of health equity as well, because that’s a big piece that I think the hospital staff is missing.
The potential for partnership between NICU and public health programming aimed at supporting parents in the postpartum period was also emphasized by community providers that did not have pre-existing relationships with the parents prenatally, but who are trying to connect with them and provide postnatal support: And we’ve had this discussion many times at our different tables of how to engage families while they’re still in hospital so that we’re a known support with a face to a name that families feel comfortable engaging with prior to leaving the hospital ... and just sort of have that soft transition in place before they’re discharged as opposed to, you know, really relying on follow up after discharge, just start building the relationship, because I think the sooner that we can be involved and have face to face with a family
Thus, our analysis highlights a paradox in the NICU-to-home transitions experience for adolescent parents. That is, NICU providers want to feel better about the support given to young families post discharge, rather than simply hoping for the best; and community providers were hoping to provide this type of support but needed to feel invited into this circle of care earlier in the NICU hospitalization – certainly as discharge plans were being made. Unfortunately, this type of coordinated support and NICU-community partnership was often only realized if the parents themselves initiated it, as this PHN explained: The only way that I knew they were being discharged was that the moms tell me. And I’m always like ‘have you got any word?’ like that ... cause I know it’s kind of a day by day process. I would say to them like ‘if they tell you you’re going home like let me know’ so then we can ... I can plan to follow up with them very quickly in the community.
Facilitating Partnerships for Mobilizing Forward
Partnerships between the NICU and home or community were, from the providers’ perspective, a core ingredient in mobilizing adolescent parents forward. NICU providers that understood the impact of the hospitalization for adolescent parents and who were able to establish therapeutic relationships still recognized the importance of partnership as part of mobilizing forward. This was seen as most successful when pre-existing home and community supports were identified and incorporated into the NICU circle of care: We have lots of moms who come in who are involved already with the Nurse-Family Partnership Program. And so that’s really great because they’re already working with the public health nurse during the pregnancy and they already have established that support network.
Even social support persons such as friends or family members were seen as vital – especially since the support of the NICU staff ends with discharge: Like maybe whoever is going to help, because usually there’s somebody at home helping that teenager. Right. Like whether it’s the mom, or grandma or partner or whoever. So just to engage them with the whole process of all the teaching that needs to go on. And it would be nice for [PHNs] to know what they’ve been taught too. So, if we got a copy of that, that would be really nice. So, we could reinforce that kind of stuff, too, at home.
As providers discussed the ideal support for adolescent parents transitioning home from NICU, the ‘who’ of such a support system was discussed less specifically than the ‘what’; and the ‘what’ often included the concept of facilitating a partnership that starts in the NICU and continues beyond discharge. As this NICU provider described: So, I think having a person that can kind of talk the NICU talk and engage with the families while they’re there and do some preliminary teaching, preliminary like I don't even want to just say teaching, but engaging with the family and even just speaking about life after the NICU and then actually be able to visit them at home once they’re home. I think that would be so amazing. And that to me, like having a person that basically goes from the NICU stage to your home, like the same person that knows the family really well and maybe could work with the family like even after a year or something would be so amazing.
For public health providers that were involved in adolescent parents’ lives antenatally, they were already providing a version of this ideal support, however, NICU providers needed to recognize this existing support, and tap into it to promote successful transition, as one PHN explained I was like it would never happen, but having a relationship between the teams ... meeting us, getting to know us, getting to know our programming ... if there was a client and they were comfortable with the hospital calling and saying, ‘hey, [nurse] I have blah, blah, blah in the nursery, do you want to come in and visit them?’ Realistically, I know that would never happen, but I think it’s a nice thought.
Neonatal Intensive Care Unit, Home and Community Contextual Factors Influencing Mobilizing Forward
Mobilizing forward post-NICU for adolescent parents, is the culmination of understanding the parental impact of the NICU hospitalization, establishing therapeutic relationships and facilitating supportive partnerships between providers that can continue beyond the NICU and bridge the NICU and home/community divide. Mobilizing forward also requires a consideration of the influence of NICU, home and community contextual factors related to successful NICU-to-home transition (see Figure 1).
Neonatal Intensive Care Unit Context
From the providers' perspectives, the NICU environment can contribute to, and even escalate, the negative impact of the NICU experience for adolescent parents. Providers described the decreased privacy faced by parents and how this can impact the development of trusting relationships between parents and staff. Additionally, the proximity to other infants and families or the use of communal spaces such as lounges and waiting rooms (where privacy can be difficult), was also seen as contributing to the emotional burden experienced by parents – as witnesses to others’ suffering or grief. All of which can contravene mobilizing forward.
Provider participants also described the acuity (or high level of critical illness) of the NICU environment and the subsequent lack of staff time affecting the overall NICU experience. One provider, who had roles both within the NICU and as a PHN in the community described a tension between knowing how much she could support adolescent parents in the NICU based on her knowledge and skill acquired from her PHN role, but that this was hampered by the NICU environment and demands placed on nurses’ time in this context.
For many adolescent parents, access to reliable or affordable transportation to the hospital on a regular basis and then costs such as meals whilst staying at the hospital were common barriers that were perceived to limit parents’ ability to spend extensive and regular periods of time with their infant in the NICU, time essential for attachment and developing parenting skills and developing parental role identity. Whilst it was noted that this barrier was not exclusive to young parents, participants indicated that this was not always recognized by NICU staff as an issue of access and instead became a point of judgement.
Visiting rules or restrictions were another element of the NICU context that impacted the overall NICU experience and ultimately mobilizing forward. Based on providers’ accounts, NICU visiting guidelines were often a reflection of more traditional families (2 parents) or more traditional support patterns for parent in the postpartum period (i.e. mother and her mother). These rules or guidelines demonstrated a lack understanding of the different types of support systems individuals may have outside of more traditional definitions; this was perceived as impacting the adolescent parents specifically.
When the NICU care context was perceived to be negative or traumatic, or when the abovementioned factors were seen to undermine an adolescent parent’s confidence or attachment to their infant, this was perceived to impede the mobilizing forward efforts and ultimately transition success. For example providers caring for parents post-NICU discharge described developmental transition difficulties such as trouble adjusting to the parental role, as well as health-illness transition challenges such as ongoing mental health concerns including anxiety and depression, and fear of ongoing stigma. Additionally, when barriers such as cost or access were not addressed in the NICU, these were seen to continue post-discharge and had an impact on participation in neurodevelopmental follow-up and engagement with other supportive services for parent and infant, thus, impacting the situational transition from hospital-to-home as well as the health-illness transition for the infant.
Home and Community Context
From the providers’ perspectives, factors in the home and community that related to successful transitions from NICU to home – or mobilizing forward – centred around the relationships within these settings available to support adolescent parents and their infants during their time in the NICU and post-discharge. These relationships were both social, including partners, family members, friends and neighbours/community members, as well as professional, including midwives, family physicians, lactation consultants, PHNs, maternity home workers and mental health professionals. Recognizing the limits of this type of support was another essential aspect of understanding the home and community context. An NICU social worker described the importance of identifying sources of social support as well as situations where the inclusion of more professional support may be needed; noting that there is significant range of support needs among the younger parent population. Importantly, when the NICU staff was able to recognize these support networks in the home and community – both social and professional – and facilitate partnerships that extended beyond the NICU, mobilizing forward was considered more likely to be successful.
Discussion
The purpose of this study was to explore what can be learnt about supporting NICU-to-home transitions for adolescent parents from the expert providers that care for this population. Improving care transitions is a global priority (World Health Organization [WHO], 2016). With an increased focus on quality transitions from inpatient settings to the community – to curb costs associated with readmission rates, emergency department use and adverse events post discharge (Health Quality Ontario, 2020) – our analysis adds to the available understanding of the NICU-to-home transition with a unique focus on adolescent parents.
The findings also support the complexity of multiple overlapping and intersecting transition experiences as outlined in Transitions Theory (Meleis, 2010). Our analysis points to the thoughtful and skilled intervention required for individuals and families experiencing transitions and the need for consideration beyond the situational aspects of NICU-to-home (e.g. supporting parenting role development, considering adolescent specific needs and supporting parental well-being). Additionally, our discussion contributes to the evolving conversation of how to best support healthy transitions and, more specifically, on how tailored approaches can more meaningfully address the unique needs of the individual and overall transition success. The main element related to transition success in this study was the ability to partner with adolescent parents, their individual social support systems, and supportive services in the community.
Partnership in the Neonatal Intensive Care Unit
Providers in this study consistently spoke to the importance of facilitating supportive partnerships as a core ingredient in mobilizing adolescent parents forward in their health and life journeys. This finding was driven by the fact that most community provider participants in this study deliver a targeted public health intervention program, the NFP home visiting program (Dawley et al., 2007). As NFP nurses, these PHNs understood the importance of partnering with young parents and their support systems to promote optimal health and social outcomes for parent and infant. Importantly, these nurses also had the knowledge and skill to operationalize these partnerships. For NICU providers in the current study, whilst understanding the importance of partnership is a core principle of Family Centred Care (FCC) (FCC is the guiding framework for care and treatment most NICUs (Dennis et al., 2017)), partnership appeared challenging to operationalize, especially with adolescent parents. This finding of difficulty practicing according to the principles of FCC is supported by a recent review of parents’ and nurses’ experiences of partnership in the NICU context (Brodsgaard et al., 2019). Like the findings of the current study, this review concluded that successful relationships between parents and nurses depended upon being respected and listened to, establishing trust and allowing parents to develop competencies whilst negotiating roles. Furthermore, a study of former NICU families and their experiences of FCC found that perceived staff judgement and a lack of meaningful relationships with nurses contributed to unmet needs of partnership in care (Sigurdson et al., 2020). Together these findings point to a need to better operationalize the principles of FCC.
Family Integrated Care in the Neonatal Intensive Care Unit
One shift that is currently occurring in NICUs in North America, is the implementation of the Family Integrated Care model (FICare) (O’Brien et al., 2013); a model of NICU care, based on FCC principles, that requires extensive parental participation in their infant’s care and bi-directional communication with the NICU team (Hall et al., 2017). In addition to improving important infant outcomes such as weight gain and breastmilk feeding; evaluations of FICare have demonstrated decreases in parent stress and anxiety and improvements in parental confidence and role attainment (Broom et al., 2017; O’Brien et al., 2018). FICare was also perceived to require less hands on-care by nurses, thus, leading to more time spent educating and supporting parents (Broom et al., 2017). FICare could go a long way in establishing supportive partnerships with young families, whilst also empowering parenting capacity that extends well beyond the NICU hospitalization (Hall et al., 2017; O’Brien et al., 2018). However, parent participants included in studies of FICare interventions are significantly older than the adolescent parent population, with mean participant ages over 30 years reported in the pilot study as well as subsequent evaluations of the intervention (Benzies et al., 2020; Broom et al., 2017; O’Brien et al., 2013); thus, further research evaluating FICare is warranted among adolescent parents. Additionally, strategies to reduce the actual and perceived stigma adolescent parents experience as they encounter health care and social care systems, including the NICU, need to be incorporated into any intervention aimed at promoting partnership, otherwise the effects of stigma could impede any benefit from such interventions (SmithBattle, 2020).
Partnership Beyond the Neonatal Intensive Care Unit
Whilst facilitating partnerships between parents and NICU staff is important, we learnt from providers in this study that partnerships also need to extend beyond the NICU to ensure adolescent parents are successful in their hospital-to-home transition experiences. Whilst there exists a wide range of programs and services available to parents and infants post-NICU discharge, they are often left to navigate these unfamiliar, complicated and fragmented systems alone (Murch & Smith, 2016). Parents become caught between systems with different priorities and funding models that are not built to handle complexity, thus, leading to inequities.
This problem was highlighted by our providers’ accounts in that NICU providers are not equipped to support the complex needs of the adolescent parent in the NICU and preparing for home, and community providers – who are equipped – are not brought in to the NICU circle of care to help fill these gaps. The literature supports the need for an integrated approach to NICU-to-home transitions with NICU and community providers having equal responsibility to pursue collaborative relationships with each other; understanding each other’s languages, systems and constraints (Murch & Smith, 2016).
Integrated Care
Integrated care approaches are recognized as promising solutions to support transitions from hospital-to-home and community; with integrated care being most effective among populations with complex needs (Brown & Menec, 2018). Integrated care strategies may operate horizontally and or vertically. Horizontal integration links similar levels of care, for example community-based health and social services; where vertical integration links different levels of care, for example primary care and specialist or tertiary care (Valentijn et al., 2013). The findings of this study suggest both horizontal and vertical integration are needed to support the NICU-to-home transitions for adolescent parents. This is supported in the integrated care literature where strategies reflecting both levels integration are often needed to counteract fragmentation of services within a health system (Axelsson & Axelsson, 2006; Valentijn et al., 2013).
The shift toward integrated care for NICU patients and families will require adopting shared goals and an integrated care culture across all levels involved in the integrated system (Valentijn et al., 2013). An example of such a shift in NICU practice is evidenced in a position paper calling for neonatal health care providers to accept the responsibility to address social determinants of health inequities among infants and families requiring neonatal intensive care (Horbar et al., 2020). In lieu of the traditional neonatal practice of follow-up, which focuses primarily on medical conditions and assessment of neurodevelopment post-discharge, authors propose follow-through, an approach focused on partnership between health professionals, families and communities to meet social as well as medical needs of infants and families. Adopting follow-through as a philosophy in the NICU could serve as a foundation to a more integrated approach to the care of NICU patients and families in the NICU and post-discharge.
Some features of integrated care initiatives include care coordination between care settings, use of individual care coordinators, home visits and co-location of staff (e.g. community providers in the hospital) (Brown & Menec, 2018). Promising NICU initiatives that incorporate some of these features include, (1) the Calgary Neonatal Transitional Care Program, that uses Clinical Nurse Specialists to deliver neonatal follow-up, in the home setting, post-NICU discharge (Lasby et al., 2004); (2) the Transition Home Plus program, that incorporated supportive services both before and after discharge from the NICU including social worker support post discharge, a home visit by a Neonatal Nurse Practitioner, and integration with primary care providers post-discharge (Liu et al., 2018) and (3) the Coached, Coordinated, Enhanced Neonatal Transition, a pilot intervention using a nurse navigator role, including care coordination up to 12 months post-NICU discharge (Esser et al., 2019). Missing from these models, however, is the partnership with PHNs that that have the specific knowledge and skill related to navigating supportive services in the communities that the families live, as well as the expertise establishing relationships with adolescent parents and mobilizing their support networks. Additionally, the presence of a provider who has an established therapeutic relationship with an adolescent parent prior to the NICU (i.e. that begins antenatally) and who is providing support through home visits in the postpartum period and beyond (such as the Nurse-Family Partnership), is valued by community and hospital stakeholders alike for the more seamless transition from community to hospital and back to community. This constant provider ensures that whilst the infant’s medical needs are met in the NICU, someone familiar to the parent and family remains available to attend to their social, emotional and educational needs.
Strengths and Limitations
The findings of this study provide a rich understanding of NICU-to-home transitions for adolescent parents; however, they represent providers’ perspectives of the phenomenon. Even though some participants had over 30 years of clinical expertise and spoke to supporting multiple cases of NICU-to-home transition; to continue to develop and extend what was learnt from this study, the transitions experiences of adolescent parents, from their own perspective, needs to be investigated. This perspective is especially important in understanding contextual factors in the NICU, home and community that facilitate mobilizing forward.
Whilst recruitment for this study was not restricted by discipline, most participants were nurses. In the NICU context this likely reflects the role that nursing and social work play in the discharge process (compared to other multidisciplinary team members who have more active roles throughout the NICU stay e.g. respiratory therapists and pharmacists). However, in the community context, several community providers that support younger parents post-NICU discharge, including family physicians, midwives and maternity home staff were not captured through participant recruitment, therefore, future study could explore how these programs/services facilitate NICU-to-home transitions for adolescent parents. A strength of the participant group was that many of the PHNs in this study were employed in programs that start working with clients early in pregnancy and provide regular support until the infant is 2 years of age; as such they can truly speak to the transition experience – as they are present both prior to hospitalization in the NICU and post-discharge. Additionally, the inclusion of different nursing roles as well as different provider disciplines (i.e. nursing and social work) allowed for triangulation of data sources and both divergent and convergent perspectives were presented in the findings.
Quality Considerations
Thorne (2016) offers a set of criteria by which studies adopting an interpretive description design may be evaluated; these include epistemological integrity, representative credibility, analytic logic, interpretive authority, moral defensibility, disciplinary relevance, pragmatic obligation, contextual awareness and probable truth. Careful attention to these criteria was maintained throughout the study and can be exemplified by (a) the development of research questions and selection methods consistent with interpretative description design and for the purpose of informing practice; (b) the presentation of findings that moved beyond description of the phenomenon (e.g. what is happening) toward interpretation (e.g. highlighting patterns, relationships and variation) and were grounded in the data affording the reader access to the researchers line of reasoning and (d) the discussion of findings within the context from which they were generated, and clear statement regarding the limits of these findings.
Conclusions
In this study, providers involved in the care of young parents offered a critical look into the complexities of ensuring a safe and healthy transition-home for this population of parent/infant dyads. Analysis revealed key ingredients to support the goal of a successful NICU-to-home transition. However, this way forward was considered by providers to be idealistic or unrealistic within the current NICU and community structures, with only exceptional cases able to navigate successfully. Findings suggest that integrated models of care, focused on meaningful partnerships between and across systems, could ensure mobilizing forward for all families who experience hospitalization for their infant shortly after birth – and especially those most at risk.
Supplemental Material
sj-pdf-1-qhr-10.1177_10497323221079785 – Supplemental Material for Mobilizing Forward: An Interpretive Description of Supporting Successful Neonatal Intensive Care Unit-To-Home Transitions for Adolescent Parents
Supplemental Material, sj-pdf-1-qhr-10.1177_10497323221079785 for Mobilizing Forward: An Interpretive Description of Supporting Successful Neonatal Intensive Care Unit-To-Home Transitions for Adolescent Parents by Elizabeth Orr, Marilyn Ballantyne, Andrea Gonzalez and Susan Michelle Jack in Qualitative Health Research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Hamilton Community Foundation (20190754).
Supplemental Material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.