
Abstract
Objective
This study investigates the effects of developing and implementing an integrated service model for antepartum, intrapartum, and postpartum care in maternal and child specialty hospitals under the deep integration of Internet technology. The goal is to provide practical references for addressing declining birth rate challenges and promoting the sustainable development of maternal and child specialty hospitals.
Methods
Using a convenience sampling method, 100 pregnant and postpartum women from a tertiary maternal and child health hospital in Chengdu, China, were selected as the participants for this study. A random number table was used to assign the participants into the control group and the intervention group, with 50 participants in each group. The control group received conventional nursing care, while the intervention group was provided with an integrated service model for antepartum, intrapartum, and postpartum care, fully implemented with Internet technology. A comprehensive comparative analysis was conducted between the two groups across several key dimensions, including the number of return visits within 42 days postpartum: The actual number of return visits for checkups, treatments, or consultations due to various health issues during this period was recorded and compared; Postpartum complications within 42 days: The occurrence rates of common complications, such as postpartum infections, hemorrhage, and milk stasis, were meticulously documented and analyzed for both groups. Service satisfaction: A nursing satisfaction questionnaire was used to objectively and comprehensively assess the satisfaction levels of participants in both groups with the care they received. Willingness for postpartum follow-up visits: Differences in participants’ subjective willingness and proactive attitudes toward arranging subsequent postpartum visits were thoroughly examined. Psychological indicators: Using psychological assessment scales, the psychological status of the two groups was evaluated from the establishment of personal health records to postpartum follow-up, analyzing the psychological differences between the two groups.
Results
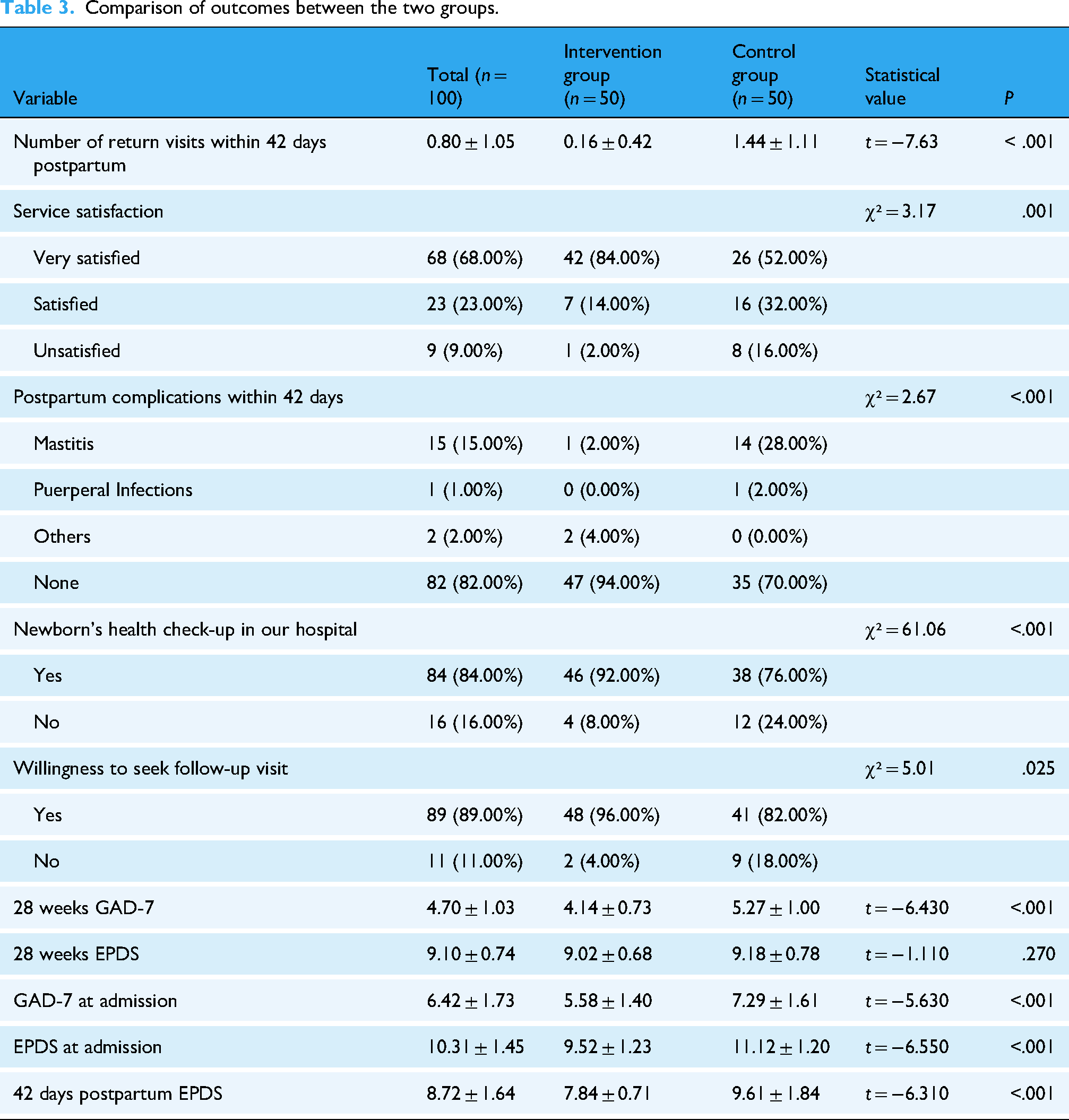
Through systematic data collection, organization, and rigorous statistical analysis, the results revealed that the average number of return visits within 42 days postpartum was significantly lower in the intervention group (0.16 ± 0.42) compared to the control group (1.44 ± 1.11) (t = −7.630, P < .001). For service satisfaction, 84.00% (42/50) of participants in the intervention group were very satisfied, significantly higher than 52.00% (26/50) in the control group (χ² = 3.170, P = .001). The incidence of mastitis within 42 days postpartum was 2.00% (1/50) in the intervention group, markedly lower than 28.00% (14/50) in the control group (χ² = 2.670, P < .001). For willingness to seek follow-up visit, 96.00% (48/50) of participants in the intervention group stated they would return to the hospital if they had health issues, compared to 82.00% (41/50) in the control group (χ² = 5.010, P = .025). 92.00% (46/50) of participants in the intervention group were willing to choose our hospital for the newborn's health checkup, significantly higher than 76.00% (38/50) in the control group (χ² = 61.060, P < .001). The 28 weeks GAD-7 scored lower in the intervention group (4.14 ± 0.73) than in the control group (5.27 ± 1.00) (t = −6.430, P < .001) and also lower in the intervention group than in the control group at admission (5.58 ± 1.40 vs. 7.29 ± 1.61; t = −5.630, P < .001). There was no significant difference in 28 weeks EPDS scores between two groups (9.02 ± 0.68 vs. 9.18 ± 0.78; t = −1.110, P = .270). The intervention group showed significantly lower EPDS scores at 42 days postpartum (7.84 ± 0.71 vs. 9.61 ± 1.84; t = −6.310, P < .001).
Conclusion
The integrated service model for antepartum, intrapartum, and postpartum care in maternal and child specialty hospitals, based on the “Internet+” concept, effectively integrates Internet technology with critical processes in nursing services. This model precisely and efficiently addresses pregnant and postpartum women's unique maternal and childcare needs at different physiological stages. It demonstrates significant advantages in optimizing medical resource allocation, improving the quality and efficiency of nursing services, and enhancing patients’ healthcare experiences and trust. The findings of this empirical study provide robust evidence for the model's effectiveness in nursing care. The successful implementation of this innovative service model offers new perspectives and directions for transforming and upgrading maternal and child specialty hospitals in the face of declining birth rates and the associated challenges and opportunities. It holds significant value for broader application and promotion, with promising prospects for further development.
With the continuous progress of socio-economic development and profound transformations in healthcare services, reproductive health has become a vital issue of widespread societal focus. In this process, traditional maternal and child nursing models have increasingly exhibited significant limitations in addressing emerging healthcare demands.1,2 From the perspective of care coordination, the critical stages of antepartum, intrapartum, and postpartum care are often fragmented in traditional models, with severe barriers to information flow and interaction. This lack of continuity and integration prevents the nursing service from forming a cohesive and systematic whole. Expectant mothers frequently need to shuttle between different departments or even multiple medical institutions, undergoing numerous repetitive examinations and consultations. This consumes significant time and energy for the patients and their families and exacerbates adverse outcomes due to incomplete or inefficient information transmission. 3 According to reports, under the current traditional care model, the overall satisfaction rate among mothers with the care they receive is only 77%, 4 highlighting the urgent need for improvements and optimizations in the traditional model.
Moreover, according to the United Nations’ World Population Prospects 2022, the global birth rate fluctuated between 140 million and 144 million from 2008 to 2017. From 2018 to 2021, however, the number of global births showed a year-on-year decline, dropping from 140 million in 2018 to 134 million in 2021, with the birth rate decreasing from 18.2‰ to 16.9‰. 5 In China, births fell sharply from 17.86 million in 2016 to 9.02 million in 2023. 6 These statistics illustrate a global trend of declining birth rates. The continuous decline in fertility poses unprecedented challenges to the operation and development of maternal and child specialty hospitals. The most direct impact is a significant reduction in patient numbers, further intensifying hospital competition. In such a competitive environment, patients are placing increasingly stringent demands on the quality and uniqueness of hospital services. To stand out and gain the trust and favor of patients, hospitals must focus on improving service quality and creating distinctive offerings. Additionally, declining fertility rates have triggered a chain reaction, significantly increasing the risk of resource underutilization within hospitals. 7 For example, healthcare workers may face reduced workloads, and medical equipment utilization rates may remain persistently low, leading to significant wastage of medical resources and potential threats to the hospital's financial performance and sustainable development.
However, with the rapid advancement of information technology, the innovative concept of “Internet+” has emerged and been widely applied across various fields, presenting new opportunities for the healthcare sector. 8 However, some studies have pointed out that pregnant women may face challenges during the use of “Internet+” nursing services, such as unfamiliarity with digital devices and poor coordination between online services and offline medical care, which can negatively impact the overall experience and effectiveness of nursing services. 9 In response to the theme of the 2024 International Nurses Day, “Our Nurses, Our Future, and the Economic Power of Care,” and to actively implement the directives of the Chinese Ministry of Health's Action Plan for Further Improving Nursing Services (2023–2025), our hospital h88as proactively explored and meticulously developed an “Internet+” integrated service model for maternal and child specialty hospitals covering antepartum, intrapartum, and postpartum care.
This innovative service model integrates distinctive service components across multiple dimensions, offering user-friendly equipment and ensuring seamless coordination between online and offline services. In the antepartum stage, it leverages the powerful functions of internet-based hospitals to provide expectant mothers with convenient online appointment booking, comprehensive prenatal health education, and professional online consultations, enabling them to receive precise and personalized guidance without leaving home. During the intrapartum stage, experienced midwives lead the entire delivery process to ensure safety, efficiency, and comfort. In the postpartum stage, an innovative “Internet+” home nursing service is introduced, where medical staff offer postpartum recovery guidance and newborn care training directly at the patient's home based on their specific needs.
This holistic and integrated service model utilizes the high efficiency of internet-based information transmission and sharing to achieve real-time data sharing and seamless connections across all stages of care. As a result, mothers can enjoy continuous, precise, and highly personalized nursing services throughout the childbirth process. This approach significantly enhances maternal and child health outcomes. It provides a novel pathway for the sustainable development of maternal and child specialty hospitals amid the macro backdrop of declining birth rates. This study was conducted in this context to explore the feasibility of applying this innovative model in practice. The research findings are reported in detail below.
Materials and methods
Study subjects
Study design
This study was a single-center, blinded, parallel-group, randomized controlled trial (RCT) with a 1:1 ratio of intervention to control groups. Conducted from January 2023 to October 2024 at a tertiary maternal and child specialized hospital in Chengdu, China, the study was registered with the Chinese Clinical Trial Registry (ChiCTR2500103547). All collected data are publicly available, and the study was implemented in accordance with the CONSORT guidelines.
Setting and participant recruitment process
The study was performed at a tertiary maternal and child specialized hospital in Chengdu, China. A total of 100 pregnant women who registered and delivered at the hospital were enrolled. Participants were randomly assigned to the intervention group (receiving “internet+” integrated service model for antepartum–intrapartum–postpartum) or the control group (receiving conventional nursing care). Recruitment was conducted from January 2023 to October 2024. The research team completed coordination with the obstetrics outpatient department and inpatient department 3 months prior to recruitment. Using the obstetrics outpatient department as the main site, eligible pregnant women were invited to participate through publicity at registration windows combined with oral recommendations during medical consultations. Researchers set up consultation points in the outpatient department to screen gestational age, health status, and smartphone usage ability through one-on-one communication. Eligible participants who met the inclusion criteria were provided with an informed consent form and enrolled after signing.
Eligibility criteria
Randomization and allocation
Randomization was performed using a random number table method. A dedicated person not involved in subsequent study procedures generated random numbers for subjects 1–100, which were sorted in ascending order. The first 50 subjects were assigned to the control group, and the latter 50 to the intervention group. Blinding was applied to data collectors and analysts to reduce selection and information bias.
Blinding
The grouping process was independently managed by a dedicated person not involved in subsequent procedures. Data collectors and analysts were blinded to group assignments to minimize information bias. However, blinding of pregnant women and the nursing team was not feasible due to obvious differences in intervention models.
Sample size calculation
For this RCT, the intervention group received internet+ integrated service, and the control group received conventional nursing care. The primary outcome was the number of hospital visits within 42 days postpartum. A pilot study (January 2023–March 2024) showed that the control group had 1.56 ± 1.14 visits, and the intervention group had 0.62 ± 0.42 visits. Using the formula from Chow 10 with two-sided α=0.05, power = 0.9, and 1:1 group ratio, n=【(Zα+Zβ)²×2σ²】/δ², each group required 31 cases. Considering a 20% dropout rate, at least 39 cases per group were needed. This study enrolled 100 subjects, meeting sample size requirements.
Ethical statement
This study adhered to the World Medical Association Declaration of Helsinki and was approved by the Ethics Committee of Chengdu Women's and Children's Central Hospital (Ethics 202463). All pregnant women received oral and written informed consent, and study data are publicly accessible.
Research methods
Control group: conventional nursing care model
The control group adopted the general nursing mode. After the pregnant and postpartum women come to the hospital to register, they should come to the hospital for prenatal checkups on time according to the rules of prenatal checkups. During the prenatal checkups, they should participate in two health classes organized by our hospital's midwife school to learn about childbirth knowledge. In addition, during the registration process, the examining doctor also requires the pregnant women to go to the midwife clinic for delivery consultation and evaluation of the delivery mechanism between cycles 26 and 32. Health education will be provided at the time of discharge, and a 42-day postpartum examination form will be issued. If any problems arise during the stay at home, patients can promptly come to the hospital for diagnosis and treatment.
Intervention group: “internet+” integrated service model for antepartum, intrapartum, and postpartum care
Establishment of the research team
A joint implementation team was established, comprising the hospital's deputy director, the nursing department, the medical affairs department (Internet Hospital Office), the finance department, the medical insurance office, the logistics support department, the equipment department, the information technology department, the legal affairs department, and the obstetrics department. The roles and responsibilities of each team member were clearly defined. The deputy director served as the overall coordinator. The nursing department was responsible for establishing the work model, determining service items, formulating work protocols, organizing the service team, revising operational processes, and preparing service tools. The technique company ensured the development and support of the information platform. The finance and medical insurance departments were tasked with setting service prices, streamlining related procedures, calculating platform revenue, and allocating nurses’ performance incentives. Other respective departments fulfilled their designated responsibilities accordingly.
Defining the care model
The hospital's Internet Hospital Office was designated as the primary management body for the online service platform, leveraging the hospital's WeChat public account and Internet applications. The service model adopted an “online application and offline service” approach. Clients could purchase nursing care service packages through the “Internet+” nursing care service platform. The offline services were coordinated by platform administrators, who reviewed the applications and assigned or selected appropriate service nurses. The platform then sent dispatch notifications to the designated nurse and the patient, facilitating home-visit services.
Establishment of the “Internet+” integrated service platform
A dedicated “Internet+” integrated nursing service menu was added in a prominent position on the hospital's WeChat public account, integrating the service information platform. The platform consists of three components: the Nurse Portal, the Client Portal, and the Management Portal, with functionality modules designed as follows: Client Portal: Built on a lightweight framework utilizing mobile internet technology for secure interaction with the server. Its features include health information inquiry, appointment scheduling, access to health education materials, and communication with healthcare professionals. Clients can view their health information, book medical services, obtain stage-specific health knowledge, and consult with healthcare providers online. Nurse Portal: Integrated with the hospital's internal system using a layered architecture. Its main functions include client care management, health data monitoring, communication, and education. Nurses can manage care plans, monitor health data with real-time alerts, and provide guidance and communication with clients and their families. Management Portal: Designed with a centralized architecture to connect multiple portals and other systems. It encompasses personnel and resource management functions, data statistics and analysis, and system maintenance and security management. This portal allows for managing healthcare staff and resources, analyzing various data, and ensuring system security and stability.
Defining nurse qualifications
Following the guidelines outlined in the “Internet+” Nursing Care Service Pilot Work Plan issued by China's National Health Commission, the qualifications for home-visit nurses were restricted to registered nurses with at least five years of clinical nursing experience and a professional title of Nurse Practitioner or above. Additionally, these nurses must hold relevant specialty nursing certifications. For nurses providing services in the Internet-based outpatient, corresponding specialty certificates are also required. Before the commencement of the project, eligible individuals could voluntarily apply and participate in training. Only those who passed the training assessment were issued a certification for “Internet+” nursing care services by the hospital, qualifying them to join the service. The training content included “Home-visit Nursing Care Service Procedures,” “Introduction to Service Items,” “Communication Skills,” “Emergency Management for Patients,” and “Nursing Practices.”
Determining service items and pricing
The selection of service items adhered to the principles of high demand, low medical risk, and ease of operation. Based on references11,12 and preliminary survey results (a market survey conducted in 2024 involving 500 postpartum women from three maternal and child specialty hospitals in Chengdu, with a questionnaire covering preferred services and pricing), discussions among relevant personnel determined two main categories: primary nursing care and maternal-infant nursing care. Pricing was set under Document No. [2023] 18 issued by the Sichuan Provincial Healthcare Security Administration, “Notification on the Publication of New and Revised Medical Service Pricing Items in Sichuan Province for 2023.” Prices were determined by referring to hospital service pricing guidelines, with service fees independently set by the hospital. After extensive research and market inquiries, the pricing was established as follows: medical service fee + service fee of 200 CNY per visit, which includes treatment and material costs. For service distances exceeding 10 km, an additional charge of 3.8 CNY per km was applied to the service fee.
Antepartum stage: Set up online midwife and nursing clinics, allowing pregnant women to make advance consultations through the online hospital platform, remotely assess the delivery process, provide online guidance, offer home nursing care services, enhance confidence in childbirth, and ensure the safety of mothers and babies. Intrapartum stage: Warm and safe deliveries are led by nurse specialists. Midwives provide continuous companionship and support throughout the birthing process. Using wearable devices and mobile applications, real-time monitoring of the maternal vital signs and fetal heart rate is conducted, and the data is recorded and shared online. An online platform is created using information technology, enabling family members to track the progress of labor in real time and provide accompaniment and support via video calls. Postpartum stage: Launch “Internet+” home-visit nursing care services, providing home visits and nursing services to monitor the recovery of postpartum women. Women can place orders online according to their needs. At the same time, establish an online community for maternal and infant health, making it easier for mothers to exchange experiences and share insights. The specific projects are listed in Table 1.
Home nursing service items. 13

Establishing safety measures
To ensure the safe and effective operation of the “Internet +” integrated service, a series of standardized procedures were formulated: Service hours: The “Internet +” integrated service operates daily from 07:00 to 20:00. Real-name registration: Clients must register with their real names, uploading real-time photos of themselves, both sides of their ID card, a photo of them holding the ID card in front of their chest, and medical documentation such as a diagnostic certificate or discharge summary. Relevant medical documentation must display the healthcare institution's official stamp to verify the registered users’ authenticity. Order risk assessment: Review staff assess clients’ medical conditions and potential order risks over the phone, documenting the evaluations. GPS tracking: Once nurses begin their services, their location is tracked in real-time using GPS. In emergencies, a one-click alarm system allows the platform to pinpoint the nurse's location and respond promptly. Client assessment and consent: Nurses must re-assess the client's condition and evaluate potential operational risks before performing nursing procedures. Clients or their families must sign an online informed consent form for home nursing services in person to minimize nursing disputes. Insurance coverage: The hospital provides personal accident and medical liability insurance for home-visit nurses and body cameras to enhance risk protection.
Continuous improvement and optimization of service quality
The service purchase process allows clients to select and adjust nursing care service items as needed. Regular quality-focused discussion meetings address patient feedback and suggestions, ensuring continuous optimization and improvement of the services provided.
Quality control
Pre-implementation phase: development and standardization
The “internet+” integrated service model was formulated based on evidence-based literature review and pre-study surveys, minimizing protocol flaws. The hospital established standardized operation procedures for all service items. All nurses involved in the project received uniform training and passed qualification assessments to ensure strict adherence to standardized protocols. Regular spot checks were conducted to implement continuous quality improvement. Additionally, the study underwent ethical review (approved by the Ethics Committee of Chengdu Women's and Children's Central Hospital, No. Ethics 202463) and filing with medical insurance and pricing authorities prior to initiation, safeguarding the rights and reasonable interests of pregnant women. Baseline data (including age, gestational age, obstetric history, etc.) were balanced between groups, with no statistically significant differences (P > .05, see Table 2), effectively controlling confounding factors.
Comparison of general information between two groups.

Implementation phase: dynamic monitoring and compliance management
Comprehensive, process-oriented dynamic tracking was implemented, supplemented by relevant insurance to ensure the safety of nurses and pregnant women. From enrollment to the end of intervention, participant compliance was systematically supervised. The research leader automatically tracked module usage frequency and task completion rates (e.g., fetal heart monitoring upload rate, knowledge learning duration) via the online platform daily. Telephone follow-ups were conducted every 2 weeks antenatally and weekly postnatally to verify nursing plan implementation. For low-compliance participants, causes were analyzed, and intensified interventions were applied to ensure study feasibility.
Post-implementation phase: data management and security
Data were double-checked by postgraduate students before entry to ensure accuracy. The internet platform signed a patient information confidentiality agreement with the hospital, storing data on a secure cloud platform to protect patient privacy.
Evaluation indicators14,15,16
The differences between the two groups were compared based on the following indicators: the number of return visits within 42 days postpartum, postpartum complications within 42 days, nursing service satisfaction, and willingness to seek follow-up care.
Number of return visits within 42 days postpartum: The number of return visits to the hospital by postpartum women and their newborns within 42 days due to illnesses was recorded for both groups.
Postpartum complications within 42 days: The occurrence of postpartum complications within 42 days was evaluated. These included mastitis, puerperal infections, others, or no complications.
Service satisfaction: A satisfaction scale was developed based on references, categorizing responses into “very satisfied,” “satisfied,” and “unsatisfied.”
Willingness to seek follow-up visits: This indicator consisted of two questions: Whether the client intends to vaccinate their child at the hospital (yes/no). Whether the client would return to the hospital for medical care if they have health issues (yes/no).
Psychological status: The Generalized Anxiety Disorder Scale (GAD-7) 17 and Edinburgh Postnatal Depression Scale (EPDS) 18 were used to assess participants’ psychological status. The GAD-7) consists of 7 items, using a 0–3 point scoring method, with a total score ranging from 0 to 21. A score of ≥5 suggests the presence of anxiety symptoms. The EPDS consists of 10 items, using a 0–3 point scoring method, with a total score ranging from 0 to 30. A score of ≥10 suggests the presence of depressive symptoms. This scale has been confirmed to be effective in measuring both before and after childbirth. The GAD-7 and EPDS evaluation were completed at the time of admission, at 28 weeks, and upon admission for delivery. EPDS was also done during the postpartum check-up at 42 days.
Statistical methods
Data were analyzed using SPSS 26.0. For continuous variables, the Shapiro-Wilk test was first used to assess normality, and Levene's test was used to assess homogeneity of variance. If the data met the assumptions of normal distribution and homogeneity of variance, they were described using means (standard deviations), and independent samples t-tests were used for between-group comparisons. If the assumptions were not met, data were described using medians (interquartile ranges), and comparisons were conducted using the non-parametric Wilcoxon rank-sum test. In this study, all continuous data met the assumptions of normality and homogeneity of variance; thus, independent samples t-tests were used. Categorical variables were presented as frequencies (percentages), and between-group comparisons were performed using the chi-square (χ²) test.
Results
Basic characteristics of the study population
A total of 109 study subjects were eligible for evaluation. Among them, three research subjects were excluded because of their refusal to participate. Finally, 106 subjects were included in the study and randomized. The control group (n = 51) received the conventional nursing model, while the intervention group (n = 55) received the “Internet+” integrated service model. During the prenatal follow-up phase, one study subject in the control group lost follow-up due to transfer, and four study subjects in the intervention group lost follow-up (3 transferred to hospital, one born prematurely due to illness). During the 42-day postnatal follow-up period, there was no loss of follow-up in the control group, while one study subject in the intervention group refused to continue participating in the study due to postnatal bleeding. Finally, 50 study subjects were each group entered the final assessment (Figure 1). There were no statistically significant differences between the two groups regarding age, education level, primiparity status, abnormal labor, monthly household income, rooming-in status, conception method, pregnancy complications, regular prenatal checkups, feeding method, delivery mode, GAD-7 and EPDS scores at the time of health record establishment (P > .05). Details are presented in Table 2.

Flow chart of participant enrollment, allocation, and follow-up.
Outcome indicators of the two groups
The intervention group had fewer return visits within 42 days postpartum and a lower incidence of pregnancy complications compared to the control group (P < .05). Additionally, the intervention group demonstrated higher service satisfaction and willingness to seek follow-up visits than the control group (P < .05). The intervention group's GAD-7 scores at 28 weeks, GAD-7 scores at admission, EPDS scores at admission, and EPDS scores at 42 days postpartum were lower than those of the control group (P < .05). The results are presented in Table 3.
Comparison of outcomes between the two groups.
Discussion
The “internet +” integrated service model optimizes nursing processes in maternal and child specialty hospitals
The study showed that the intervention group had an average reduction of 1.28 ± 0.69 hospital visits by mothers or newborns within 42 days postpartum, confirming that the intervention nursing model optimized care processes and improved medical resource utilization efficiency. Traditional nursing, constrained by time-space limitations and information asymmetry, often forces pregnant women to make multiple hospital visits. In contrast, this model leverages internet technology to provide online health education and appointment services antenatally, reducing unnecessary hospital visits; enables real-time medical data transmission intrapartum for prompt clinical management, minimizing postpartum complication-related readmissions; and offers online rehabilitation guidance and home nursing postnatally to meet domiciliary care needs. Multiple studies19,20,21,22 have shown that internet technology enhances information transfer efficiency and reduces patient travel, consistent with our findings. This study systematically constructed a full-process integrated nursing model, breaking the limitations of fragmented care across stages to achieve seamless care service docking.
The “internet +” integrated service model improves service satisfaction
The study revealed that the nursing satisfaction rate in the intervention group was 98%, representing a 14% increase compared to the traditional model, indicating significant advantages of this nursing model in meeting the needs of pregnant women. The intervention model covered prenatal, intrapartum, and postpartum stages, providing comprehensive and personalized services: diversified health education was conducted antenatally to help pregnant women understand the childbirth process; intensified communication with family members and professional nursing were provided intrapartum to enhance maternal security; and home services and online guidance were offered postnatally to address practical problems. Meanwhile, internet technology broke through time-space barriers, enhancing the timeliness and convenience of interaction among healthcare providers and patients, enabling rapid response to pregnant women's needs.23,24 Existing studies 25 have confirmed that the comprehensiveness and personalization of nursing services, as well as good communication, are key to improving satisfaction. This study formed a complete service chain by integrating full-cycle nursing services, precisely meeting the needs of pregnant women at different stages.
The “internet+” integrated service model enhances healthcare quality
The study demonstrated that the provision of three-dimensional convenient services and timely, accurate health guidance across prenatal, intrapartum, and postpartum stages significantly improved medical quality, with a 24% reduction in maternal complication rates. This improvement is attributed to: prenatal health management that identifies and intervenes in potential risks in advance; intrapartum professional care ensuring delivery safety; and postpartum home nursing guidance facilitating rapid maternal recovery. Tight integration across stages prevented complications caused by care gaps or delays. 26 Existing studies have confirmed that comprehensive and continuous nursing services play a positive role in reducing maternal complications.27,28 By leveraging the internet, this study constructed a three-dimensional nursing system covering the entire perinatal period, transforming the relatively independent stages of traditional nursing into a systematic medical service, thereby enhancing overall medical quality.
The “internet +” integrated service model enhances the hospital's influence
The study demonstrated that the intervention group showed a 16% increase in the child health checkup rate at our hospital and a 14% rise in the preference for seeking treatment at our hospital when health issues occurred, significantly enhancing the hospital's service influence. This nursing model provided pregnant women with high-quality prenatal, intrapartum, and postpartum care experiences, improving their and their families’ recognition of the hospital's overall services, thereby extending trust to related departments such as the child health care department and neonatal department. Existing studies29,30 have shown that high-quality obstetric care services often drive the business development of other related hospital departments (e.g., neonatal and child health care departments), as patients tend to choose other services from the same hospital after receiving excellent care.31–33 Against the backdrop of global fertility rate decline, this study proposes a new approach for the transformation and upgrading of maternal and child specialized hospitals by constructing an integrated model from the perspective of maternal and child care, which differs from the traditional single-department service improvement model.
The “internet +” integrated service model improves the psychological status of pregnant and postpartum women
The intervention group had significantly lower GAD-7 at 28 weeks, GAD-7 at admission, EPDS at admission, and EPDS scores at 42 days postpartum compared to the control group, indicating that this model has a significant effect on improving psychological conditions such as anxiety and depression in pregnant women. The reason is that the Internet plus integrated nursing model plays a role in improving the accessibility of mental health services through multiple dimensions: in the prenatal stage, pregnant women can query the prenatal examination results in real time through the patient side, and their information needs are responded immediately, effectively alleviating the anxiety caused by information asymmetry. During the delivery phase, nurses rely on real-time data monitoring and intelligent warning systems to provide professional support throughout the entire process, significantly enhancing the sense of safety of postpartum women. During the postpartum stage, mothers can consult nursing issues at any time through the patient end, and nurses can use the nurse end to provide remote guidance and home care, timely solving practical difficulties and reducing psychological pressure caused by poor postpartum adaptation. It is reported that 34 the timeliness and accessibility of nursing services are the key factors affecting the mental health of pregnant and lying in women. This study broke the time and space constraints through Internet technology, and built a full cycle, seamless nursing service system, which is just in line with this, and effectively improved their psychological status.
Limitations
This study has several limitations. First, the sample was derived from a specialized maternal and child hospital in a specific region. Affected by regional disparities in medical resources, economy, and culture, direct promotion may be difficult in grassroots areas with weak informatization, limiting generalizability. Second, some data relied on self-reports and measurements by pregnant women. Due to insufficient professional knowledge, measurement bias and comprehension errors may occur, affecting result reliability. Third, although baseline data showed no statistical differences, with the expansion of sample regions and scale, individual differences in maternal age, physical condition, educational level, etc., may interfere with the stability of research findings. To address these shortcomings, future research could be optimized in three aspects. First, expand the sample coverage to include pregnant women from medical institutions in different regions and levels, compare the application effects of the nursing model under diverse backgrounds, and verify generalizability. Second, explore the introduction of intelligent and standardized measurement equipment, combined with AI technology to assist data collection and analysis, reducing human errors. Third, establish a multi-dimensional individual characteristic assessment system, use big data to analyze the correlation between individual traits and model effectiveness, achieve precise intervention, and provide more robust evidence for model promotion.
Conclusion
This study shows that the Internet plus Maternity and Children's Specialized Hospital prenatal midwifery postpartum integrated nursing model can reduce the rate of return to hospital and the incidence of complications after childbirth, and improve nursing satisfaction and mental health. In future clinical applications, it is recommended to embed this model into hospital information systems to achieve full process data exchange, build a multidisciplinary collaboration mechanism, provide integrated services, and strengthen pregnant women's training through maternity schools, expand service coverage in conjunction with community health centers, provide door-to-door guidance and publicity, and provide better, safer, and more convenient services for women and children.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076251357657 - Supplemental material for Development and implementation of an “Internet ” integrated service model for antepartum, intrapartum, and postpartum care in maternal and child specialty hospitals: A randomized controlled trial
Supplemental material, sj-doc-1-dhj-10.1177_20552076251357657 for Development and implementation of an “Internet ” integrated service model for antepartum, intrapartum, and postpartum care in maternal and child specialty hospitals: A randomized controlled trial by Chen Shaochuan, He Lianci, Zhang Qiongyue, Wang Xin, Xie Huiqiong, Tan Ying, Feng Xiaohui and Li Huimin in DIGITAL HEALTH
Footnotes
Acknowledgements
Special thanks to the medical department, information department, medical insurance department, and all nursing staff in the obstetrics department of Chengdu Women and Children's Center Hospital for their support in the model construction.
Ethical considerations
This study was approved by the Ethics Committee of Chengdu Women and Children's Central Hospital (Approval No. 202463).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chengdu Medical Research Project, Sichuan Province Health Informatics Research Project (grant nos. 2024099 and 2023014).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The transcribed interview data are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.