
Abstract
Background
The intensive care unit (ICU) is a separate area in which potential health care services for patients who are in critical condition with detailed observation, monitoring, and advanced treatment than other units. This study aimed to assess the incidence and predictors of inpatient mortality after inpatient treatment was started in Debre Markos Comprehensive Specialized Hospital.
Methods
A facility-based retrospective cohort study was employed among 384 ICU-admitted patients from December 30, 2020 to January 1, 2022. The collected data were entered into Epi Data version 4.2 and exported to STATA 14.0 for further analysis. The Cox proportional hazard regression model was fitted after checking using the Schoenfeld residual and log-log plot test. A categorical variable with an adjusted hazard ratio of 95% CI was claimed for predictors.
Result
Overall, 384 admitted adult patients were included in the final analysis with a mean (±SD) age of 42.1 (±17.1) years. At the end of the follow-up period, 150 (39.06%) cases died in the ICU. The overall incidence of the mortality rate was 16.9 (95% CI: 13.7-19.55) per 100 person per day. Epidemiologically, 347 (90.36%) cases were medical illness, 25 (6.51%) surgical, and 12 (3.13%) were obstetric cases, respectively. The median length of inpatient stay was found to be 4.9 (IQR ± 2.8) days. In multivariable analysis; being (+) for human immunodeficiency virus (AHR = 0.59, 95% CI: 0.39-0.91), age ≥65yearas (AHR = 1.61, 95% CI: 1.11-2.32), and admission on weekend-time (AHR = 1.48, 95% CI: 1.06-2.06) were predictors of inpatient death.
Conclusion
The overall in-hospital mortality rate was significantly higher than in the previous study in this hospital with a short median survival time. The inpatient mortality rate was significantly associated with age ≥65 years, being HIV positive, and admission during weekend time. Therefore, effective intervention strategies should be highly needed for ICU team members for early risk factors prevention.
Introduction
The intensive care unit (ICU) is a part of the hospital in which special treatment is delivered to severely ill patients. 1 It is typified by having a high level of monitoring and therapeutic technology, a very high degree of organization, and high staff-to-patient ratios1-3 with advanced monitoring and therapeutic technologies to deliver quality care for critical patients.4,5 Despite the high burden of critical cases who were admitted to ICU, most improvement points to discharged after critical care recorded post-admitted cases. 6 Although this significant proportion of ICU-discharged patients subsequently die is also evidenced with a rate ranging from 6 to 27%.5,7
Mortality in ICU is a global burden and it varies across the world and depends on ICU infrastructure, staff availability, training patterns, and the cause of ICU admission.1,7 In developed continents like North America, Oceania, Asia, and Europe, ICU mortality is relatively low with a rate of 9.3, 10.3, 13.7, and 18.7%,2,6,8 while in the rest of the world such as South America and the Middle East, the mortality was found to be 21.7 and 26.2%.3,8 In Africa, the ICU mortality rate is high compared to other continents; specifically in Nigeria, Uganda, Tanzania, and Kenya were 32.9, 40.1, 41.1, and 53.6%, respectively.1,9
The epidemiology and severity of cases were affected by two critical determinates including time of arrival at ICU and a skilled physician with mechanical equipment both for recovery and post-admission death. 9 The most frequently diagnosed and admitted cases for care at ICU were stroke, 10 respiratory failure, 1 road traffic accident, 9 cardiac failure, 11 medical comorbidities (diabetic mellitus, hypertension (HTN), and HIV/AIDS were prominent evidence.12-14
After inpatient cases were admitted to the ICU, there were two existing criteria including inpatient death or prognosis discharge. 15 A significant proportion of cases were faced subsequently dying after inpatient treatment was set with 6-27% ranges.3,16 The epidemiology of inpatient deaths was varied and the most commonly observed death reported was traumatic brain injury (TBI) which ranged from 40 to 40.5%,10,15 congenital malformation 27.3%, 16 and road traffic accident 67.5%. 15 Differences in patient characteristics including socioeconomic status, ICU admission threshold health care system, and multiple comorbidities determine inpatient death post-admission at ICU.6,10 The absence of prehospital care and increased age were the main predictive factors for in-patient death. 1
Studies done in Africa have shown that death in the ICU remains an area of higher mortality rate reported room in a given hospital 3 including developed countries as low as 6% in America 17 to as high as 52.3% in Turkey. 12 Likewise, in Sub-Sahara African (SSA) countries including Ethiopia, study reports indicated inpatient death varied from 28 to 50%.15,18-20 Post-admission ICU death was also significantly varied by health care facilities in Ethiopia including comprehensive specialized university hospitals such as 2.26% in Hawassa 8 and 38.7% in Gondar Hospitals. 8 Moreover, patient death at ICU varied with age with 32.5% for under 5 and 8.6% for adults. 16
Previous study findings on the burden of cases in ICU admission in Ethiopia were varied by facility and evidence in Addis Ababa, Hawassa, and Bahir Dar were 10.3, 12.7, and 25.3%, respectively. 15 The resource constraints and inconsistencies in clinical personnel training play an important role when considering the treatment of cases in the ICU. 7 Moreover, there were no studies on the outcome of ICU-admitted cases to assess post-admission inpatient death and predictors in Debre Markos hospital. Therefore, this study aimed to assess the incidence and predictors of inpatient mortality after the case started care in the ICU in Debre Markos referral hospital from 2020 to 2022.
Methods
Study Area and Period
This study was conducted in the Amhara region, North West Ethiopia, in Debre Markos Comprehensive Referral Hospital. Debre Markos town is located 300 km away from the national capital city of Ethiopia and 265 km away from the Bahir-Dare regional city of the Amhara region. Accordingly, this hospital has been giving overall care to more than 3.5 million catchment population per year, including referred cases for inpatient care. 9 This hospital has 193 inpatient beds and 11 intensive care beds with 3 functional ventilators. The emergency department of the hospital provides services to more than 112,053 patients a year. This hospital has two main ICUs for adults and pediatrics in different rooms and an open ICU system run under the Department of Internal Medicine.9,21
Study Design
A hospital-based retrospective cohort study was carried out in ICUs from December 30, 2020 to January 1, 2022.
Source of Population
All adult admitted patients who got surgical or medical diagnoses and admitted to the ICU at Debre Markos referral hospital.
Study Population
All adults were admitted for inpatient care in the ICU at Debre Markos Hospital from December 30, 2020 to January 1, 2022.
Inclusion and Exclusion Criteria
All adults were admitted for inpatient care in the ICU at Debre Markos Hospital from December 30, 2020 to January 1, 2022.
Exclusion Criteria
Missed and incomplete patient medical files and under including children <12 years since adult and child admission units were separated, we excluded those files.
Sample Size Determination
The sample size for this study was determined by using the single population proportion principle using the underneath formula and parameters
Variable
Dependent and Independent Variables
The dependent variable was the clinical outcome of ICU admitted cases (death/cured) whereas the independent variables were sociodemographic variables, diagnosis at admission, presence of comorbid illness, source, frequency and category of admission, vital signs at admission, trauma type, time of admission, source of referral, and need for mechanical ventilation were some of categorical variables.
Operational Definition
Event is defined as a patient who died after being admitted to an ICU room.
Censored refers to patients who were discharged alive from the PICU or those with no event of interest
Data Quality Control
The English version of the data extraction checklist was developed from previous different literature from literature.8,10,15 The data were extracted from the patient's records and operation notes using a data extraction tool for the occurrence of the event. The data collection checklist consists of demographic characteristics, clinical and laboratory findings, and patient management variables. Two BSc nurses were recruited after being well-trained by the principal investigator about the purpose of the study and how to extract the data and fill the checklist properly. Before the actual data collection was accompanied, a 5% pretest was conducted and the necessary amendment was given to the checklists. Data were checked daily for completeness and consistency throughout the data collection period.
Data Analysis and Used Software
The inpatient mortality rate of cases in the ICU was calculated using the total number of people per observation day's year (PPD). Descriptive non-parametric statistical tests such as the Kaplan–Meier plot were used to estimate the survival time using the following formula
22
ni = number at risk at the beginning of the ith interval [t−1, ti) di = number events/TB/incidence during the interval [t−1, ti) Ci = number censored in the interval [t−1, ti).
The final semi-parametric regression was used for identifying predictors for inpatient mortality using Cox regression after checking the necessary assumptions (Cox, 1972). This is checked using a graphical diagnostic based on a log–log survival curve and observed versus expected graph. The multivariable Cox proportional hazard equation of the Cox model is expressed as follows:
22



The term h0 is called the baseline hazard (constant HR) and is the value of the hazard if all xi is equal to zero (the number exp(0) equals 1). That is, h(t) reminds us that the hazard may (and probably will) vary over time for the event of interest (Incidence of mortality). Variables with p value < .25 in the bivariable Cox regression analysis were included in the multivariable Cox regression model to determine the factors associated with inpatient death in the ICU room. Akaike's information and Bayesian information criteria were used to compare and check the final model. The model with the smallest value of the information criterion will be selected as the final model of the analysis after checking the Nelson-Alan and Cox Snell residual test for the final model adequacy tested. Independent variables that are significant at p value less than .05 levels in the multivariable Cox regression models were considered predictors of mortality. Finally, narration tables and graphs were used to present the findings of the study.
Ethical Clearance
The ethical review board of Debre Markos University College of Health Science ethical review board cleared this research to be conduct after checking the compatibility with human subjects based on the Helsinki Declaration with refill number (Refill:-DMU-CHS-0015/2015). In addition, the IRB board of Debre Markos University has approved written informed consent from each study subject before that data was collected. Since the data was recoded and review of the documentation, the university board waived the written informed consent from each study participant with no contact directly with the admitted patients.
Result
A total of 384 medical files were reviewed for final analysis. However, 18 individual files were excluded due to incompleteness. The overall response rate was found to be 95.8%.
Sociodemographic Characteristics of Admitted Patients
The majority 264 (61.46%) of the admitted were females and 260 (67.71%) of them were from rural. The mean (±SD) age of the study patients was 42.13 (±17.5) years. More than half of the participants 232 (60.42%) had health insurance during treatment, but 137 (35.68%) and 15 (3.91%) were private and free service user groups. More than half 199 (51.82%) of the cases were transferred directly from the emergency room for critical care. Two hundred and forty-five cases (63.8%) were admitted during working time, but only 139 (36.2%) were on weekend days (Table 1).
Baseline Sociodemographic Characteristics of Patients Admitted in the ICU at DMRH, Northwest Ethiopia, 2019.

Epidemiology of ICU-Admitted Cases
Epidemiologically, more than two-thirds, 285 (74.2%) of the admitted cases were noninfectious, whereas the remaining 99 (25.78%) were admitted due to serious infectious causes. More specifically, 347 (90.36%) admitted cases were medical, 25 (6.51%) surgical, and the rest 12 (3.13%) cases were gynecological and obstetric cases, respectively. More specifically, 46.2% of cases were cardiovascular disease, 55 (19.23%) chronic obstructive pulmonary disease, 45 cases (11.72%) involved HIV (+), and the remaining 24 cases (54.17%) involved road traffic accidents. The mean length of inpatient stay after ICU treatment was set to 4.28 (±3.9) days (Table 2).
Baseline Clinical and Treatment-Related Characteristics of Patients Receiving Treatment in ICU at Debre Markos Comprehensive Specialized Hospital.

Treatment Outcomes and Incidence of ICU Mortality
Overall, 384 cases were followed for 1668 person-per-day observations. At the end of the study period, 150 (39.06%) cases were died after starting ICU treatment. The overall incidence of inpatient mortality rate was found to be 16.9 (95%CI: 13.7-19.55) per 100 people per day, whereas the remaining 193 (50.26%) were cured, 25 (6.51%) were referred and 16 (4.12%) patients were left to medical advice (Figures 1 and 2).

Outcome of adult patients admitted in the adult ICU room in Debre Markos Hospital.

Kaplan–Meier hazard estimate of adult patients admitted in the ICU compared by day.
The majority 90 (60%) dying cases were reported within 3 days post admission. The median length of inpatient stay was found to be 4.9 (IQR (IQR ± 2.8) days (Figures 3 and 4).

Kaplan–Meier failure estimate of adult patients admitted in ICU compared by age group.
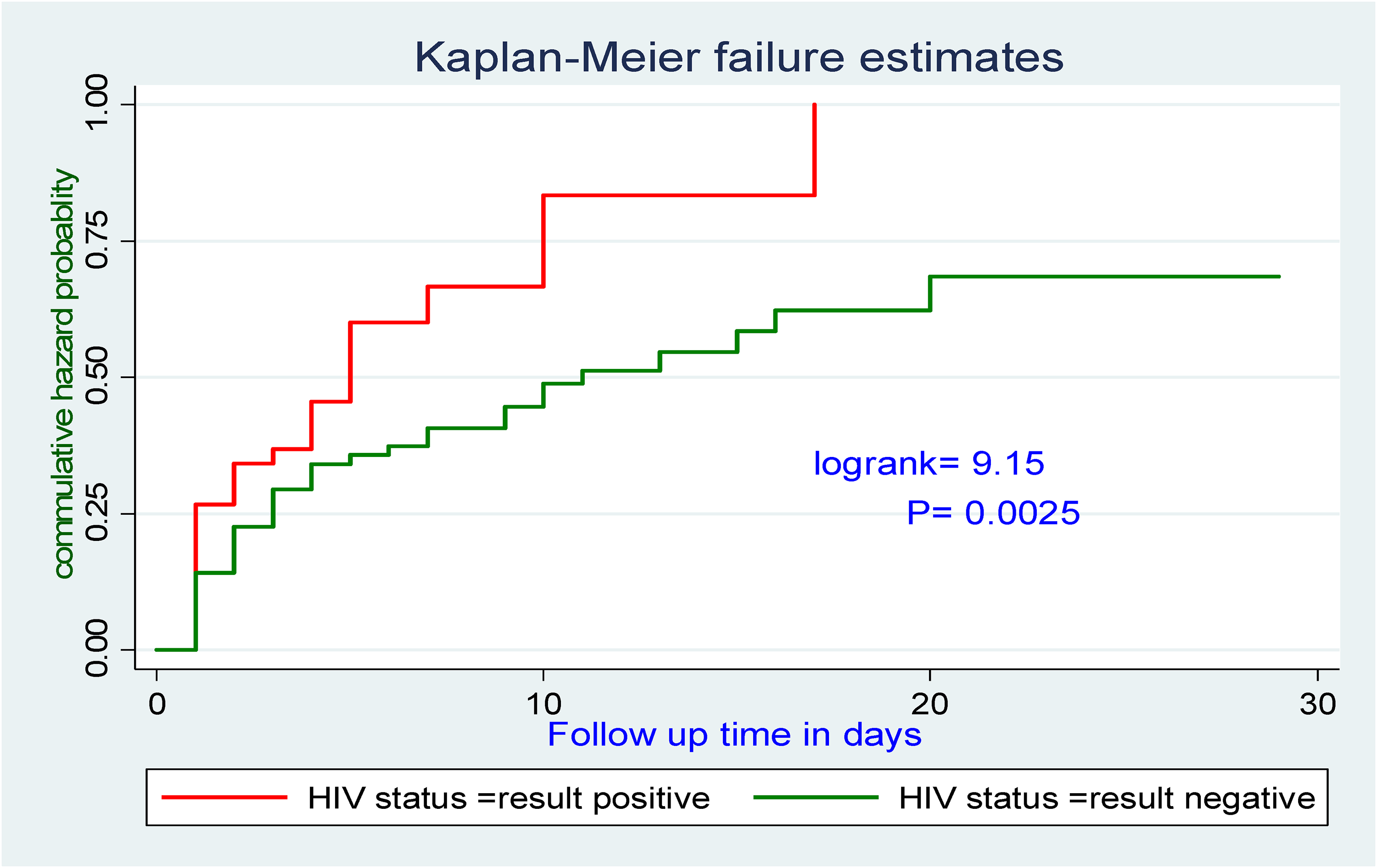
Kaplan–Meier failure estimated by HIV status of patients admitted in the ICU.
Predictors for ICU Inpatient Mortality
In the bivariable analysis of the selected baseline, clinical and management variables showed an association with time to death at a p value < .2 including case admission during (working/weekend) days, patient age, HIV-infected patient, treatment cost, admission source (referral or new), partner, length of ICU inpatient stay, and multiple comorbidities have an association with the rate of inpatient death.
However, in the final multivariable Cox-proportional hazard model; after controlling certain confounding, three categorical variables were independent predictors of ICU death. Accordingly, the risk of inpatient ICU death among cases with age ≥60 years was nearly two-fold (AHR = 1.61, 95%CI: 1.11-2.32) times increased inpatient mortality as compared with <60 years. Likewise, Patients admitted to the ICU during weekend days were nearly two times increased as compared with working days (AHR = 1.48, 95% CI: 1.06-2.06). Finally, HIV-negative ICU cases were 41% less likely to die as compared with those HIV-positive admitted cases in ICU(AHR = 0.59, 95% CI: 0.39-0.91; Table 3).
Bivariable and Multivariable Cox Regression to Identify Predictors of Mortality in the ICU, Debre Markos Specialized Comprehensive Hospital, Northwest Ethiopia.

*p<0.05 indicates statistically significant association with outcome variable.
Discussion
This study found that 150 (39.06%) adult ICU cases died during the follow-up period made the overall incidence of mortality rate 16.9 (95%CI: 13.7-19.55) per 100 people per day. This is higher than the study done in Hawassa 148 (12.7%). 10 This could be due to the result of a lack of prehospital care, scarcity of ventilators and ICU beds, limited surgical capacity, and poor adherence to protocols in Debre Markos Hospital. Conversely, the final report is lower than 39% finding in St. Paul Hospital, 37.7% in Jimma University medical center, 18 41.4% in Tanzania, 14 52.3% in Turkey,12,20 28.4% in Iran, and 26.1% in Kenya. 23 The discrepancy may be because of the differences in the study population as well as levels of ICU structure in terms of skilled staffing, study setting, and period could be the reasons for the variation reported between the study and different health facilities.
Meanwhile, the median length of inpatient stay was found to be 4.9(IQR (IQR ± 2.8) days with 0.75 (95%CI; 0.701-0.796) survival rate. In this point, the most frequent stay was 64 (49.8%) was 1 day with a maximum of 4. This report is consistent with previous findings in Gonder Specialized Hospital,8,16 which is more than one in five, 118 (23%) of cases were stayed exactly 24 h, patients who stayed in ICU for less than 24 h were more likely to die than patients who stayed four. This might be explained due to late arrival in the ICU and delayed intervention, shortage of crucial emergency drugs; and the absence of mechanical ventilation equipment in the ICU highly increased inpatient deaths.
In this report, the risk of inpatient death for admitted cases with age ≥ 60 years was nearly two-fold (AHR = 1.61, 95%CI: 1.11-2.32) increased as compared with age <60 years. This is consistent with the previous findings in St. Paul's Hospital, 24 Kenya, 23 and previous studies.25-27 This may be because the older patients were affected by many other concomitant chronic diseases and did not easily respond to any invasive treatment physiologically when age increased inversely, when body immunity is decreased, and even highly susceptible to hospital-acquired infection post-admission and inpatient death is inevitable in the ICU.
In the multi-variable of this study, we revealed that patients admitted in ICU on weekend hours were at higher risk of dying as early as compared with patients admitted on working days. This is consistent with the findings in the Gondar referral hospital 16 and the Netherlands. 28 However, our finding was not supported by two American studies and studies done in the UK. 29 This may be due to a lack of skilled senior physicians on weekends, because of the difference in the study area in which the number of special ICU professionals and staffing models may vary from area to area.
In this study, HIV-positive patients were at higher risk of early death compared to HIV-negative patients. This finding is supported by previous findings in Spain.30,31 This may be because of the general immunosuppression of HIV-positive patients and the inability to cope with a critical illness. Consistent with previous studies’ suggestion in Ethiopia8,16 admission with multiple-comorbidity were significantly associated with post-admission death in the ICU, mainly cardiovascular (36% and chronic respiratory (17.9%) cases with other multiple comorbidities accounted for more than half of ICU death. 8
The final report of this report indicated that patients admitted in the ICU during weekend days were nearly two times increased as compared with working days (AHR = 1.48, 95% CI: 1.06-2.06). HIV-negative ICU cases were 41% less likely to die as compared with those HIV-positive admitted cases in ICU (AHR = 0.59, 95% CI: 0.39-0.91). This is evident from previous literature suggestions that4,6-8,10,11,32 weekend admission by emergency physicians increases the load and burden cases for quality care and specifically which is not supported with trained human resources and material inpatient death in the ICU unit is inevitable unless effective prognosis-tailored care and resource utilization were invested.6,16 This is evidenced in the finding of this work, which is more than one in every third 139 (36.2%) admitted cases were started ICU care on weekend admission by emergency physicians.
Unlike previous research findings in Ethiopia such as Debre Markos, Hawasa, and Gondar referral hospitals8-10,15,16 with a significant cases fatality ratio for patients admitted with age ≥60 years, cardiogenic shock, admitted with intubation, and traumatic brain injury, however, in this study, there was no significant association with cases admitted cardiogenic shock, and admission with intubation. However, medical cases accounted for more than 89% of ICU admissions and needed significant work on modifiable risk factors, increased recovery rate, and further load of ICU admission.
Limitations of the Study
The findings of this study might suffer from the fact that it is a retrospective design and the chart recorded review evidence, and some variables were missing while others were not recordable. This study failed to track and indicate the death that occurred at home and this might be an underestimated mortality rate because cases discharged with some medical instants and agents were at higher risk of complications and death.
Conclusion
The overall in-hospital mortality rate was significantly higher than in the previous study in this hospital with a short median survival time. The inpatient mortality rate was significantly associated with age ≥ 65 years, being HIV positive, and admission during weekend time. Their effective intervention strategies should be highly needed by ICU team members for early risk factors prevention.
Footnotes
Acknowledgments
The authors would like to express our deepest gratitude to the Ethical Review Board of Debre Marcos University College IRB board ethically cleared us to conduct this research. Also, we would like to thank data collectors, supervisors, and data clerk staff for their unreserved collaboration during data collection.
Authors’ Contributions
TS contributed to conceptualization, data curation, formal analysis, funding acquisition, methodology and investigation, project administration, resources, software, and writing–review and editing. FK contributed to methodology, project administration, resources, software, and writing–review and editing for final submission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The data set for this research is from the corresponding author upon reasonable request.