
Abstract
Background
Being born with low birthweight is a major determinant of perinatal, neonatal, and infant survival. Even though low birthweight-related neonatal mortality is high, there is an information gap regarding the survival status of low birthweight neonates and their predictors of mortality in Ethiopia.
Objective
This study was conducted to assess the survival status and predictors of mortality among low birthweight neonates admitted to Amhara region referral hospitals in Ethiopia.
Methods and Materials
A retrospective follow-up study was conducted on randomly selected low birthweight neonates admitted to the Amhara region referral hospital between January 01-2017 and December 30-2018. Data were entered into Epi-data 4.4.2.1 and exported to Stata 14 for cleaning and analysis. A cox regression model was used to analyze the data. Tables, charts, and text were used to report the results.
Results
This study revealed that 35.2% of participants died with incidence rates of 37.86 per 1000 person-day observations (95%CI: 31.79-45.10). Sepsis (AHR:1.72(95% CI: 1.05-2.81), respiratory distress (AHR: 2.03 (95% CI:1.36-3.03), necrotizing enterocolitis (AHR: 2.47 (95% CI: 1.17-5.20), congenital anomalies (AHR:2.37 (95% CI: 1.36-4.13), extreme low birth weight (AHR:2.62 (95% CI:1.54-4.44) and prematurity (AHR: 2.55 (95% CI:1.10-5.92) were independent predictors of mortality.
Conclusion
Sepsis, respiratory distress, necrotizing enterocolitis, congenital anomalies, extremely low birth weight, and premature birth were the independent predictors of mortality. Therefore, it is better for all stakeholders to focus more on the early diagnosis and management of low birth weight neonates with the factors associated with mortality.
Introduction
Neonates weighing less than 2500 g measured within the first hour of delivery before significant weight loss occurs, irrespective of the infant's gestational age(GA) are considered low birthweight (LBW). 1 Although almost half of the world's newborns’ weight are not measured globally, in 2013 around 22 million (16%) of all neonates were low birthweight, of which South Asia and sub-Saharan Africa had the highest (41%) burden. 2 LBW neonates create a high emotional and economic burden on the family, society, and the world because of the long-term effects of LBW complications throughout life.2,3
Being born with low birthweight is a major determinant of perinatal, neonatal, and infant survival.3,4 LBW neonates are predisposed to infectious diseases due to their immature immune systems and develop severe complications such as; jaundice, respiratory distress syndrome (RDS), 5 sepsis, jaundice, apnea, and birth asphyxia.6,7 Most complications that occur due to LBW finally lead to mortality with various lengths of hospitalization6–8. Many studies have identified several risk factors for mortality of LBW neonates, although the severity of mortality differs depending on each birth weight category and burden of complications. 9
Globally, in 2017 there were approximately 5.4 million under-five deaths, of which 2.5 million died during the neonatal period; approximately 80% of the neonates were delivered with LBW. 10 Low and middle-income countries (LMICs) including; Asia, Africa, and Latin America hold a higher burden of neonatal morbidity and mortality at different neonatal periods due to the high number of deliveries of LBW neonates. 11
Africa, particularly sub-Saharan Africa including Ethiopia has a high prevalence of neonates born with LBW. 12 In 2021, the pooled prevalence of neonates who had been born with low birth weight in sub-Saharan Africa was 9.76%, of these, the highest low birth weight was recorded in Ethiopia, 16.21%. 13
In sub-Saharan Africa the magnitude of adverse birth outcomes was 29.7% and low birth weight was the most common adverse birth outcomes (31%). 14 According to World Health Organization, World Bank and United Nations health data estimates for the population in Ethiopia, in 2017 low birth weight was the ninth top cause of death which accounting for 23,091 (3.63%) deaths in the total population. 15 In different regions of Ethiopia, low birth weight was the major contributor to neonatal deaths, and neonates born with low birth weight have shown higher mortality during the neonatal period than neonates with normal birth weight16–18. The prevalence of proximate low birth weight in Ethiopia was 26.9%, out of which 17.1% was very low birth weight and 9.8% were under the category of Low birth weight. 18 Even though LBW-related neonatal mortality is high, there is an information gap about the survival status of low birth weight neonates and their predictors of mortality in Ethiopia. Therefore, this study aimed to assess the survival status of low birth weight neonates and identify predictors of mortality to fill this information gap.
The findings will highlight the causes and information gap of mortality among LBW neonates and suggest prevention strategies especially for health care providers in Amhara region referral hospitals. This study will also provide some insights for future research along these lines.
Methods and Materials
Study Area and Period
This study was conducted in selected referral hospitals in the Amhara region. Among all four referral hospitals in the region; FelegeHiwot Referral Hospital (FHRH), Debremarkos, Dessie, and Debrebirhan, two of them were selected using lottery method (FHRH, Dessie referral hospitals) for the study. This study was conducted between December 2018 and June 2019.
Study Design
An institutional based retrospective follow-up study was conducted among LBW neonates admitted to the NICU wards of selected Amhara region referral hospitals between January 01-2017 and December 30-2018.
Population, Eligibility Criteria
All neonates with birthweight <2500g who were admitted to the Amhara region referral hospitals of the NICU ward were the source population. All neonates with birthweight <2500g admitted from January 1-2017 to December 30-2018 were the study population. Live birth neonates with birthweight for <2500g were eligible for the study.
Sample Size Determination
The sample size was determined by using Stata version 14 statistical packages by using Cox proportional hazards (CPH) model by considering the following assumptions: Confidence level (CI:95%),Power = 80%,Variability(SD) = 0.4, and the previous study hazard ratios was immunization status = 5.1(20). The probability of an event/death observed in a previous similar study was = 0.053. 19 After adding a 10% non-response rate for incomplete data /missing key information and lost medical charts, the final sample size utilized for this study was 384.
Sampling Techniques and Procedure
From four referral hospitals in the Amhara region, FHRH and Dessie referral hospitals were selected using the lottery method. The two-year data of all LBW neonates admitted to the NICU wards between 01 January 2017 and 30 December-2018 were enrolled by using the admission registration book by recording their medical record numbers sequentially. A total of 840 and 630 LBW neonatal medical registrations were obtained from FHRH and Dessie referral hospital, respectively. The samples were proportionally allocated to each hospital (219 from FHRH and, 165 from Dessie referral hospital). Subsequently, based on the allocation for each hospital, the required number of medical registration cards was selected by a simple random sampling technique using a computer random number generating system in Excel. The selected medical cards were obtained from the medical records office.
Variables of the Study
The dependent variable was the survival status of low birthweight neonates dichotomized as death or censored.
The independent variables of the study included the following
Operational Definitions
Data Collection Tools and Procedures
After reviewing different types of literature, the checklist was adapted to address the objectives of the study. The checklist consists of information on maternal and neonatal socio-demographic data, neonatal- related factors, LBW-related complication/ co-morbidity factors, and maternal and obstetric-related factors. Data were extracted from neonatal medical charts using a structured checklist by two BSc nurses and supervised by an MSc nurse at each hospital
Data Processing, Analysis, and Presentation
After checking data completeness and consistency, the collected data were coded and entered into Epi- data version 4.4.2.1(www.epidata.dk/download.php), exported into Stata version 14 (www.stata.com) for cleaning and analysis. During the analysis, we used hospitalization outcome as a dependent variable indicating death as an event of interest.
“Kaplan-Meier survival estimates” were used to estimate the median survival time, cumulative probability of survival and survival differences between covariates. The Log-rank test was also used to compare the statistical survival differences between the categories of different explanatory variables.
The CPH model was used to identify the independent predictors of mortality. Based on bivariate analysis, those variables with a p-value< 0.25 in the bivariate analysis were transferred to the multivariable analysis, and finally in multivariable analysis those variables having a P-value < 0.05 at a 95% confidence level were considered as an independent predictors of mortality in LBW neonates.
Results
Neonatal and Maternal Socio-Demographic Characteristics
During the follow-up period, 1470 LBW neonates were admitted to both hospitals. Of these, 384 LBW neonatal medical charts were reviewed based on the required samples. A total of 384 LBW neonates’ medical charts were reviewed, and 26(6.77%) medical charts were excluded as 20 charts were not available and six of them were incomplete. The remaining 358 LBW neonates were included in the analysis making a response rate of 93.23%.
Two hundred twenty- four (62.57%) of the study participants were males. Three hundred fifty-one (98.04%) neonates were in the age category of ≤ 7 days Two hundred fifty- five (71.23%) mothers were belonging to the age category of 20-34 years. The median age of the mothers was 26 years with an interquartile range of (22.70-30.00) (Table 1).
Socio-Demographic Characteristics of low Birth Weight Neonates and their Mothers Admitted from 01 January 2017 to 30 December 2018 to the NICU of the Amhara Region Referral Hospitals, Ethiopia, 2019.

Maternal and Obstetrics-Related Characteristics
Two hundred thirty-eight (66.48%) neonates were born to mothers of a single pregnancy. Fifty-one (14.25%) neonates were born from mothers who have developed pregnancy-induced hypertension during pregnancy (Table 2).
Maternal and Obstetrics-Related Characteristics of low Birth Weight Neonates Admitted from 01 January 2017 to 30 December 2018 to the NICU the Amhara Region Referral Hospitals, Ethiopia, 2019.

HIV = human immune virus, DM = diabetes Mellitus, PIH = pregnancy induced hypertension.
Low Birth Weight-Related Complications/co-Morbidities Characters
Hypothermia 258 (72.07%), sepsis 244 (68.16%), RDS 153(42.7%), jaundice 55 (15.36%), congenital anomalies 34 (9.5%) complications were identified among LBW neonates (Table 3).
LBW-Related Complication Characteristics of low Birth Weight Neonates Admitted from 01 January 2017 to 30 December 2018 to the NICU of the Amhara Region Referral Hospitals, Ethiopia, 2019.

RDS = respiratory distress syndrome.
Neonatal-Related Characteristics
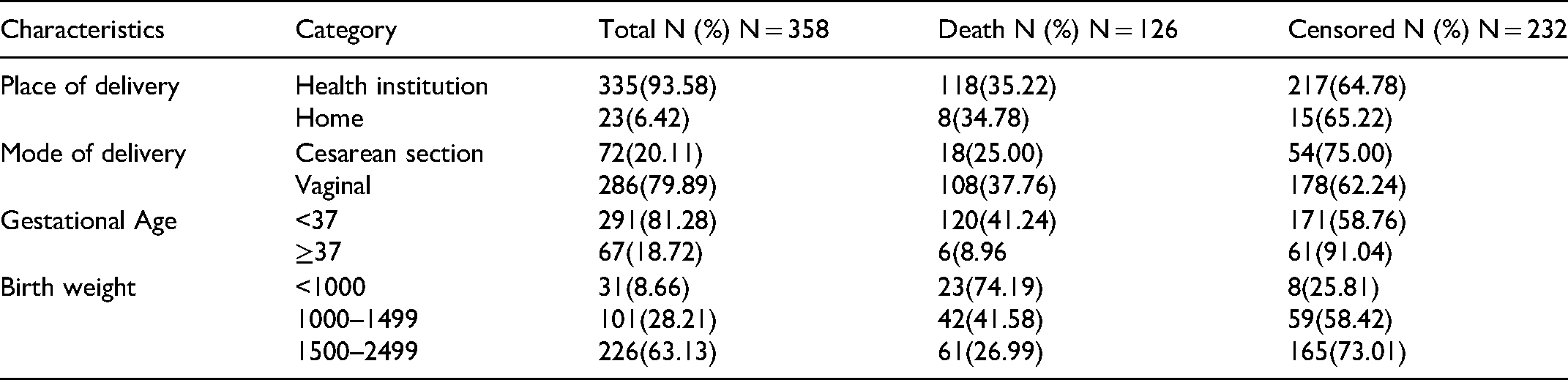
Three hundred thirty-five (93.58%) neonates were born in health institutions and 286 (79.89%) neonates were born with spontaneous vaginal delivery. Two hundred ninety-one (81.28%) neonates were born preterm. Two hundred twenty- six (63.1%), 101(28.2%), 31(8.7%) neonates were born LBW, VLBW, and ELBW respectively. The overall median weight of LBW neonates was 1600g with an interquartile range of (1300-1920g) (Table 4).
Neonatal-Related Characteristics of low Birth Weight Neonates Admitted from 01January 2017 to 30 December 2018 to NICU of the Amhara Region Referral Hospitals, Ethiopia, 2019.
Survival status, Mortality Rate, and Median Survival Time among LBW Neonates
A total of 358 LBW neonates were followed for 0–28 days. From three hundred fifty-eight neonates, 126(35.2%) (95%CI: 30.4-40.3) died during the follow-up period/ hospitalization period, and 232 (64.8%) were censored (out of which, 153 (42.73%) were discharged to home, 63(17.60%) were discharge left against medical advice, 14 (3.91%) were alive at the end of the study period and the remaining two (0.56%) of them were transferred to other institutions).
LBW Neonates were followed for 3328 person-day observations, with an incidence rate of 37.86 (95%CI: 31.79-45.1) deaths per 1000 person-day–observations (hospitalization period). LBW Neonates were followed for 358 person-day observations, with an incidence rate of 111.73 (95%CI: 81.95- 152.32), 1423 person-day observations, with an incidence rate of 40.05 (95%CI: 30.89-51.92) and 884 person-day observations, with an incidence rate of 20.36 (95%CI: 12.82-32.32) on the first-day observations, seventh day-observations and 14th day-observations respectively. The overall median survival time of LBW neonates in this study was 27 days (95%CI: 21-,). In this study the median survival time of neonates in each birth weight category were 2 days and 26 days for Extreme low birth weight (<1000g) and very low birth weight (1000-1499g) neonates respectively (Table 5).
Incidence Rate and Median Survival Time of low Birth Weight Neonates in Each Birthweight Category Admitted from 01 January 2017 to 30 December 2018 to NICU of the Amhara Region Referral Hospitals, Ethiopia, 2019.

Comparison of Mortality Rate and Mortality-Free Survival among low Birth Weight Neonates
The Kaplan Meier graph shows, the overall cumulative survival, and failure probability among LBW neonates (Figure 1).
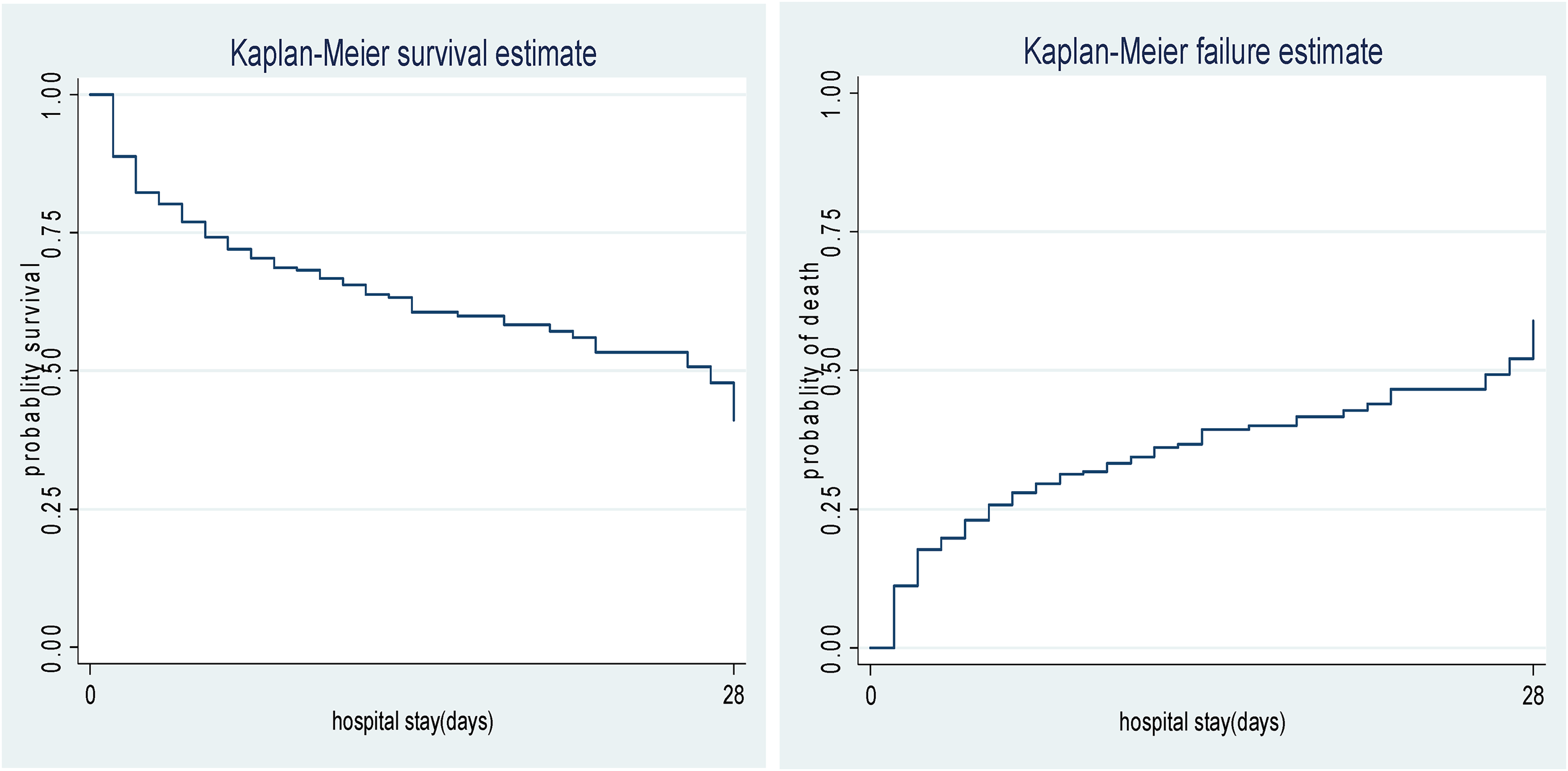
Overall Kaplan-Meier survival and failure estimate of low birth weight neonates admitted from 01 January 2017 to 30 December 2018 to NICU of the Amhara region referral hospitals, Ethiopia, 2019.
By using the Kaplan Meier estimator of survivor function in this study, the highest 62(49.2%) proportion of mortality occurred on the first two days of the follow-up period. Moreover, by using the Kaplan Meier estimator of survivor function, the cumulative probability of survival at the end of 1day, 7 days, and 28 days of the follow-up period were 88.83% (95%CI: 85.08-91.68), 70.37% (95%CI: 65.00-75.08), 41.07% (95%CI: 28.88-52.85) respectively.
Comparison of Survivorship Functions for Different Categorical Variables
Comparisons of the survival time difference between different groups of categorical covariates were done through the Kaplan-Meier survival graph and statistical log-rank test. In this study LBW neonates born through vaginal delivery (P = 0.047), born from mothers with PIH (P = 0.03), neonates with sepsis (P = 0.002), congenital anomalies (P = 0.0354), birthweight of <1000g (P = 0.000), Preterm neonates (P = 0.0001), RDS (P = 0.001), NEC (P = 0.0124) had lower survival time as compared with their counterparts. However in categories of sex of neonate (P = 0.2058), maternal age (P = 0.6416), pregnancy status (P = 0.4492), maternal placental abruption (P = 0.1747), jaundice (P = 0.8565), hypoglycemia (P = 0.1920) and place of delivery (P = 0.9621) had no survival time difference as compared to their counterparts.
Cox Proportional Hazard Assumption Test
Assumptions of the Cox proportional hazard model were assessed by using Schoenfeld residual/ global test, which became non-significant, (0.2194) indicates the proportional hazard assumption of CPH regression was met. The Multi-collinearity of each independent variable was checked using the variance inflation factor and the mean VIF for those variables was 1.13.
Cox Proportional Hazard Model Fitness Test
The fitness of the final model was checked graphically by using the Cox Snell residual; shows the hazard function follows the 45° line closely confirmed that the final model is a good fit (Figure 2).

Cox-Snell residual, Nelson -Aalen cumulative hazard graph on low birthweight neonates admitted from 01 January 2017 to 30 December 2018 to NICU of the Amhara region referral hospitals, Ethiopia, 2019.
Predictors of LBW Neonate's Mortality
In this study LBW, neonates with sepsis had a 72% higher hazard of mortality as compared to neonates without sepsis (AHR: 1.72 (95% CI: 1.05-2.81)). The hazard of death for LBW neonates with RDS was 2.03 times higher as compared to LBW neonates without RDS (AHR: 2.03 (95% CI: 1.36-3.03). LBW neonates who had NEC haves a 2.47 times higher risk of death as compared to LBW neonates without NEC (AHR: 2.47 (95% CI: 1.17-5.20). LBW neonates with congenital anomalies have 2.37 times higher risk of death as compared to LBW neonates without congenital anomalies (AHR:2.37 (95% CI: 1.36-4.13). The hazard of mortality was 2.62 times higher for LBW neonates born with birthweight <1000 as compared to those neonates with birthweight 1500–2499g (AHR: 2.62(95% CI: 1.54-4.44). LBW neonates with GA<37 weeks have a 2.55 times higher hazard of death as compared to those LBW neonates GA> = 37 weeks (AHR: 2.55 (95%CI: 1.10-5.92) (Table 6).
Results of the Bivariate and Multivariable Analysis of low Birth Weight Neonates Admitted from 01January 2017 to 30 December 2018 to NICU of the Amhara Region Referral Hospitals, Ethiopia, 2019.

Discussion
This retrospective follow-up study was carried out to determine the survival status of LBW neonates and predictors of their mortality. In this study, the overall incidence rate of mortality was 37.86 per 1000 person-day observations (95%CI: 31.79-45.10). This result is higher than the studies conducted in Burkina Faso 19 and Felege Hiwot Comprehensive Specialized Hospital, Ethiopia in 2020. 20 This marked difference with study done at Burkina Faso, 19 might be because this study focused on LBW neonates admitted to neonatal intensive care units with complications that may have a high risk of mortality, whereas the study in Burkina Faso includes all LBW-born neonates who were not admitted to NICU. Additionally, the difference with study done in Felege Hiwot Comprehensive Specialized Hospital, Ethiopia in 2020 20 might be due to variation in the number of study setting. This study was multi-centric and covers the larger area that is appropriate for generalizability of the findings. While, the study done in Felege Hiwot Comprehensive Specialized Hospital, Ethiopia in 2020 20 was single site study.
This study revealed that the overall probability of survival for LBW neonates at the end of follow-up period was 41.07%(95% CI:28.90-52.90),which is lower than the study done in Telangana, India. 21 The possible reason for the difference might be service provision differences. The study finding revealed that LBW neonates diagnosed with sepsis had higher mortality as compared to their counterparts. This result is supported by studies conducted in Oidisha, India, 7 and Gujarat, India. 21 This might be due to the that sepsis by itself facilitates death.
The study also showed that LBW neonates diagnosed with RDS had a higher hazard of death as compared to non-RDS LBW neonates. Other studies conducted in Bangladeshi, 6 Gujarat, India, 21 and Zimbabwe 22 supported these result. The possible reason might be the fact that LBW neonates with RDS mostly have the risk of lung collapse leading to hypoxia and finally may end up with death. LBW neonates diagnosed with NEC had a higher hazard of death as compared to their counterparts. This result is supported by other studies conducted in South Africa, 23 and Johannesburg. 24 This might be because neonates with NEC have intestinal stenosis and dehydration that can cause mortality. This study also demonstrated that neonates born with congenital anomalies had a higher hazard of death than their counterparts did. This finding was supported by studies conducted in Thailand, 25 Latvia, 26 and Cuiaba, Mato Grosso. 27 The possible reason might be neonates with congenital anomalies have the risk of developing different complications of neurological, cardiovascular, and GIT, which can lead to mortality.
In the current study LBW, neonates with a birth weight less than 1000g during birth had a higher hazard of mortality than neonates whose birthweight was between 1500–2499g.The current findings are supported by other study findings such as in Bangladeshi, 28 Northeast Brazil, 29 India, 30 Thailand, 25 Latvia, 26 South Africa 24 and China. 31 This might be because ELBW neonates have high body surface area and less body brown fat that makes them predisposed to many complications of hypothermia and hypoglycemia that leads to death.
In this study LBW neonates born at GA<37 weeks had a higher hazard of death as compared to those LBW neonates born at GA≥37weeks.This result is supported by different studies conducted in Bangladesh, 28 Burkina Faso 19 and Cuiaba. 27 This might be because premature neonates are born with an immature immune system, less adipose tissue, and incomplete organ formation predisposes them to a risk of complications that can lead to death.
The following limitations should be considered concerning this study. Data were collected from secondary source and some important predictors that can't be found in the patient medical chart, which might have a significant association with LBW neonatal death, may be missed. Besides, since patients with lost card and incomplete records were excluded which may underestimation the result can be possibly happened.
Conclusion
In this study, the incidence rate of LBW neonatal mortality was high and continues as a public health issues. The overall median survival time of the neonate was twenty-seven days. The factors that were significantly associated with mortality were having sepsis, RDS, NEC, congenital anomalies, ELBW, and preterm. Therefore, special attention should be given to those identified predictors of mortality by the responsible body
Footnotes
Acknowledgments
Mekelle University College of health science, school of nursing is acknowledged for providing this opportunity to conduct this study. Our thanks also go to Felegehiwot referral hospital, Dessie referral hospital staffs of pediatric, neonatology care- team, and the card extractors. It is also our pleasure to thank the data collectors and supervisors.
Availability of Data and Materials
The raw data file could be provided for research purposes only, upon request via e-mail of the corresponding author
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
To conduct this study ethical clearance letter was obtained from the institutional review board of Mekelle University, College of health sciences with ref number 1270/2019. Permission letters were written for Dessie and FHRH hospitals. Then, data were collected after consent of cooperation was obtained from Dessie referral hospital and FHRH referral hospital administrator focal person to use the secondary data for this study. Confidentiality of the information was secured throughout the study process.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.